
Abstract

Introduction
Acute aortic dissection is associated with poor outcomes. 1 Aortic dissection is classified as Stanford Type A when involving the ascending aorta and Type B when involving the descending aorta or arch. 2
Stanford Type A has a well-accepted management algorithm with aggressive control of blood pressure and immediate transfer to a cardiac surgery unit for surgical intervention (American Heart Association Guidelines [AHA] and European Society of Cardiology 3, 4 ). Stanford Type B, however, has been shown to have significantly better outcomes when treated medically (International Registry Aortic Dissection [IRAD] 1 ). As such simple uncomplicated acute Type B aortic dissection within the UK has for decades largely been treated in non-specialized departments with attempts to refer to cardiac services rebuffed. The incidence and prevalence of Type B aortic dissection in the UK is unknown and there has been no systematic collection of data on diagnosis, management or outcomes. These patients are commonly young and they are not served well by the current often indifferent attitude of concerned specialties.
Type B aortic dissection is a complex dynamic disease with true and false lumens, rentry sites and malperfusion syndromes affecting multiple organs. Selected complicated cases with malperfusion syndromes are accepted into specialized units for intervention, either open, endovascular or hybrid approaches, however, the majority are managed medically. Managing blood pressure is complex in this setting and on occasions requires high-level care with invasive monitoring including arterial lines and spinal drainage. As thoracic aortic intervention in the UK enters a new era, it is incumbent on us to set standards for best care. Our suggestion is that it is no longer an acceptable standard of care to leave management of patients with acute Type B aortic dissections to non-specialized units.
We review current relevant guidelines and develop a case for registration and or transfer of all Type B aortic dissections to centres which offer a subspecialized aortic service which is multidisciplinary team (MDT)-led and capable of offering a full range of interventional services whether open surgery, endovascular or a hybrid procedure.
Acute aortic syndrome
Acute aortic dissection is included within a spectrum of disease termed acute aortic syndrome. 5 The syndrome includes diseases from intimal tear, localized/extensive dissection, intramural haematoma, penetrating atherosclerotic ulcer, and injury from trauma. Acute aortic dissection by definition involves an entry tear in the intima and commonly an exit tear and may well be complex with multiple tears and flaps. Figure 1 shows a representation of this disease process as cyclical with initiation and propogation of the injury superimposed on spectrum of chronic disease processes. The representation demonstrates several very interesting aspects in the concept of aortic dissection and its natural history. First, and as suggested by Vilacosta and San Roman, 5 penetrating atherosclerotic ulcer and intramural haematoma may be preludes to full-blown dissection which introduces dilemmas in the management of these entities and predicting their behaviour. Following from this is the second interesting aspect which is that studies have shown reversibility and intramural haematoma may progess to full dissection or even regress. 6 Understanding the regulatory points in this cycle is key to predicting behaviour and treating the condition in a patient-specific manner.
In contradiction to management of acute Type A aortic dissection which has a mortality of 50% over the first week when managed medically versus 30% when managed surgically, acute Type B dissection has a higher mortality when managed operatively (30%) compared to medical management (10%). 1 More recently the concept of endovascular intervention with fenestration and/or stenting has been reported and is of noticeable success in complicated cases with end-organ compromise. 7 The role of endovascular therapies in modifying the natural history of uncomplicated acute type B dissection remains uncertain. A recent trial (INSTEAD) has shown no additional benefit to this approach in simple uncomplicated acute Type B dissection. 8
The natural history and management of these conditions are further complicated by the frequent presence of aneurismal disease and connective tissue disorders. Given the dynamic and often unpredictable natural history of these conditions, there requires a strong element of multidisciplinary experience as well as capacity for monitoring end-organ perfusion, repeat scanning and multimodality therapy to achieve a successful outcome. The exact form of intervention in these different maladies is reviewed in several publications but is best summarized in the American Heart Association Guidelines 3 and is beyond the scope of this essay which concentrates on organization of services.
UK national and international outcomes
We have no good data on the national incidence of acute Type B aortic dissection in the
UK. Neither do we know how many of these patients are treated medically or how many
undergo surgery or endovascular treatment. We do not know the immediate survival or
long-term outcomes for this disease in the UK. The regulatory societies of relevant
specialties (Society of Cardiothoracic Surgery [SCTS; see Acute aortic syndrome. This figure depicts the acute aortic syndrome described
by Vilacosta and San Roman
5
as a process of initiation (e.g. high blood pressure) and propagation
(degenerative tunica media). Underpinning the pathogenic processes are other
risk factors for ASS such as aneurysmal size (<4 cm, 4–6 cm and >6 cm)
and tissue disorders such as Marfan syndrome and other connective tissue
disorders. The end result is entry into the pathogenic process which is
represented as a cyclical process from intimal tear, intramural haematoma,
localized and extensive dissection to contained and uncontained leak resulting
in death. Each entity within the process has a regulatory element. As
represented there may be regression of the process at each point. The acute
aortic syndrome may result in malperfusion and end-organ compromise. AAS =
acute aortic syndrome; CTD = connective tissue disorder; Type A and B =
Stanford Type A (ascending aorta) and Stanford Type B (arch and descending
aorta) (in colour online)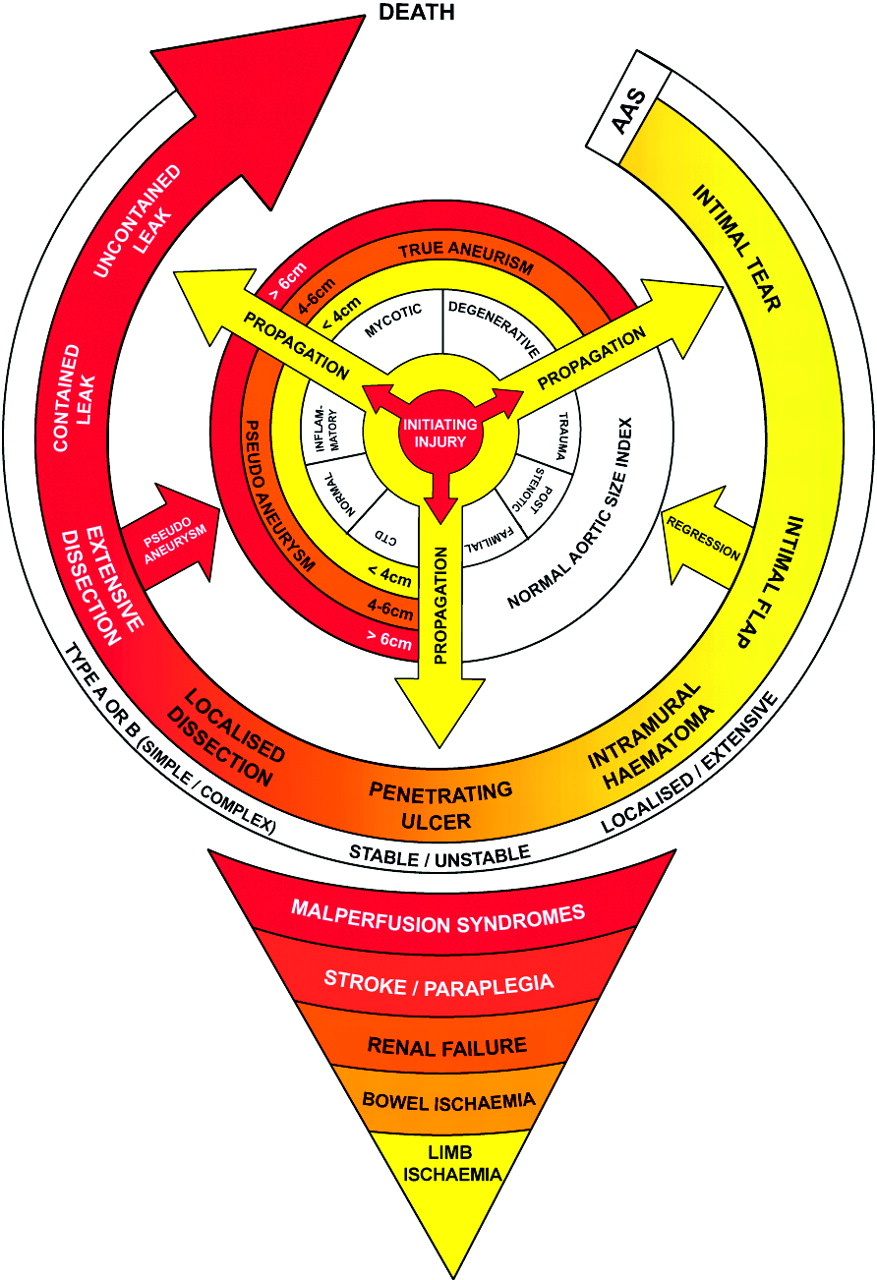
Our first suggestion in this essay is that we systematically collect data on admissions and outcomes for dissection of the aorta both Type B and Type A. Voluntary registers are rarely comprehensive, accurate or maintained over the long term. We suggest a simple approach would be to campaign for ICD codes to make the simple distinction between Type A and Type B making it easy to identify patients, cross-check with their HES data and survival rates using the national tracking service.
Existing service arrangements: who and where?
Current service provision is mixed at best. Acute Type A aortic dissection is transferred to Cardiac Surgery Units for immediate surgery. Type B aortic dissection in the acute phase may either be managed medically in non-specialized units or, if complicated, transferred to either Cardiac Surgery, Vascular Surgery, Cardiology or Interventional Radiology. Long-term follow-up of Type B aortic dissection is equally variable depending on local arrangements. We suggest there needs to be some compulsory service arrangements to oversee this process. While we acknowledge local service arrangements will always prevail since it reflects historical service development, specialization and interest, we suggest the process should be overseen by a MDT ensuring registration of cases, patient-specific intervention and audit of process and outcomes. We suggest this oversight should be enshrined in National Institute for Health and Clinical Excellence (NICE) guidelines or European guidelines on managing aortic dissection. Retrospective discussion of acute Type A dissection and ‘rolling discussion’ of acute Type B dissection should be mandatory.
What do UK governing bodies say about service provision of acute Type B?
NICE guidelines
NICE guidelines exist entitled Endovascular stent-graft placement in thoracic
aortic aneurysms and dissections (Guidance 127) (see Current evidence on the safety and efficacy of endovascular stent-graft
placement in thoracic aortic aneurysms and dissections indicates that it is
a suitable alternative to surgery in appropriately selected patients,
provided that the normal arrangements are in place for consent, audit and
clinical governance; Clinicians should enter all patients having endovascular stent-graft
placement in thoracic aortic aneurysms and dissections into the thoracic
stent-graft registry supported by the Vascular Society of Great Britain and
Ireland and the British Society of Interventional Radiology; The procedure should be performed by a multidisciplinary team with access to
facilities for cardiothoracic surgery and cardiopulmonary bypass.’
The merits of open versus endovascular treatments of these conditions is beyond the scope of this manuscript, however, several important aspects of care are stipulated. First, whatever procedure is performed, it should be MDT-led. Second, if endovascular intervention is indicated it should be performed in a facility with provision for on-site conversion to an open procedure with cardiopulmonary bypass. Last, processes should be in place for consent, audit and clinical governance. Consent implies an appropriate specialist should see the patient to have a full discussion about all options either open, endovascular or hybrid. Audit and clinical governance implies a facility for registration of activity and outcomes.
The UK Department of Health ‘Service Framework for Cardiovascular Health and Well Being’
The national service framework covering vascular diseases has been published by the
UK government Department of Health (see
Points of interest in this document include performance indicators. In order to improve performance there must be audit processes in place. While this document divides intervention between specialties based on anatomy, we suggest this is divisive and stipulates a general preference for endovascular or hybrid solutions to the arch and descending thoracic aorta. We suggest the process should be patient-specific and based on the anatomy of the pathology and patient co-morbdities and, therefore, should be MDT-led not ‘intervention-led’.
The Vascular Society of Great Britain and Ireland
The Vascular Society published The Provision of Service for Patients with
Vascular Disease in 2009 (see
An encouraging theme running through this document is the support for the MDT as a conduit through which all activity should be entered.
The Society of Interventional Radiology and Society of Cardiothoracic Surgery
Joint guidelines have been issued with the British Vascular Society and The Society of Interventional Radiology as described above. The SCTS has no specific recommendations on intervention and management of Type B aortic dissection.
What information on service provision can we extract from international studies and guidelines?
The American Heart Association
The newly published AHA guidelines
3
on thoracic aortic disease has a specific section referring to service
delivery in Section 17.1 entitled ‘Recommendations for Quality Assessment and
Improvement for Thoracic Aortic Disease (AHA Guidelines)’. Although not specifically
for Type B aortic dissection they remain broadly relevant. Class I recommendations
with Level C evidence state: Hospitals that provide regional care for patients with acute sequelae of
thoracic aortic disease (e.g. procedures for thoracic aortic dissection and
rupture) should participate in standard quality assessment and improvement
activities, including thoracic aortic disease registries. Such activities
should include periodic measurement and regional/national interfacility
comparisons of thoracic aortic disease-related procedural volumes,
complications and risk-adjusted mortality rates; Hospitals that provide regional care for patients with acute sequelae of
thoracic aortic disease (e.g. procedures for thoracic aortic dissection and
rupture) should facilitate and coordinate standardized quality assessment
and improvement activities with transferring facilities and emergency
medical service teams.
Cooperative joint facility meetings to discuss opportunities for
quality improvement; and Interfacility and emergency medical services team comparisons of
pretransfer care based on available outcome data and future
performance measures developed in accordance with guidelines.’
Suggested domains of quality include procedural volumes (facility and operator), outcomes (risk adjusted mortality, readmissions or complications), time to diagnosis and intervention and structural measures (distance to nearest referral centre, services available and contingency planning).
These recommendations are pivotal in defining a mechanism for ensuring quality of services relevant to this area of medicine and argue in favour of the suggested service organization suggested here.
The International Registry of Aortic Dissection?
The IRAD franchise collect and publish data on aortic dissection but have offered no
suggestions for service provision (see
The European Society of Cardiology (ESC)?
The ESC has issued very detailed guidelines on diagnosis and management of aortic dissection but offer no advice on service provision. 4
The Cochrane Library?
The Cochrane Collaboration has published a meta-analysis in this area but it
specifically attempts a comparison between TEVAR and open surgery for thoracic aortic
aneurysm (see
A ‘hub and spoke’ model for care of aortic dissection in Minnisota
A recent paper published in Circulation (Cardiovascular Quality and Outcomes) describes an interesting MDT-based model for regional care of aortic emergencies. 9 Based in Minneapolis, the tertiary specialist centre has set up a programme of region- wide education and protocols to increase awareness, diagnosis and improve early management and transfer to specialist services. This approach has had a dramatic effect on time to intervention and outcomes for these patients.
Proposal for UK and implementation
Acute aortic syndrome is a complex dynamic disease whose natural history can be managed with favourable outcomes providing the patient is able to access the appropriate specialist facilities in a timely manner. A recent meeting of the SCTS (Liverpool 2010) has highlighted the need for centralization of aortic dissection services (Type A) to a few centres within the UK with the intent of improving outcomes. Ideally we suggest this should be extended to Type B dissection. Simple and complicated Type B dissections should all be referred to specialized centres for consultation. All cases should be registered and discussed at a thoracic aortic MDT. Advice should be issued and arrangements made for follow-up care. Complicated Type B dissections should be transferred to specialized units and admitted to intensive case for treatment by an MDT involving cardiac surgeons, vascular surgeons, interventional radiologists and intensivists. All treatment modalities should be available. Centres with the capacity and the interest should be encouraged to transfer all Type B dissection. (simple or complicated) for centralized specialized care. Attempts should be made to create local area networks to improve the efficiencies and outcomes of the service. Follow-up specialized services should be available and there should be audit and good clinical governance. We suggest NICE Guidelines, as well as supporting statements from national and European societies should mandate true prospective and retrospective MDT discussion. Recognition of regional networks treating these patients, by the UK Government Care Quality Commission, should in a part be based on evidence of this multidisciplinary process and, of course, outcomes.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
The service arrangements described in this essay largely describe an existing multidisciplinary team process for processing thoracicaortic aneurysms in Liverpool. As such many specialties are involved, far too many to acknowledge in authorship. We would like to acknowledge several individuals who are key to this process including: Abbas Rashid, Michael Desmond, Jonathan Kendall, Hilary Fewins, Rao Vallabhenini, Richard McWilliams, Francesco Torella, Rob Fisher and John Brennan