
Abstract

Case history
A 54-year-old woman presented to hospital with an episode of haematemesis and four episodes of malaena. She was haemodynamically stable. Her admission bloods showed a haemoglobin of 11.0 g/dL with a MCV of 100.5 fL, urea 8.8 mmol/L, INR of 1.5. She was known to have hypothyroidism and a gastric ulcer 30 years ago; she drank 2 units of alcohol a day but she was otherwise fit and well.
On the first day, an endoscopy was performed, which showed a small amount of fresh blood in the stomach with two sites of possible, but not convincing, bleeding high on the greater and lesser curves. There was also fresh blood in the second part of the duodenum but virtually none in the first part. In the second part of the duodenum, one small erosion was found where the mucosa was quite oedematous but there was no site of actual bleeding. The erosions were cauterized using a gold probe.
She had five further large episodes of malaena with a subsequent haemoglobin drop to 7.2 g/dL. Her systolic blood pressure dropped to 80 mmHg and her pulse was 120 bpm. Despite transfusion of 3 units of packed red cells and 3 units of fresh frozen plasma, her haemoglobin remained at 7.4 g/dL and she continued to have malaena.
The next day, a further endoscopy in theatre was performed under general anaesthetic, which once again showed some fresh blood in the stomach and duodenum but no varices. She proceeded to have a CT scan of the abdomen with intravenous contrast (Figures 1 and 2) which showed that the distal duodenum was markedly abnormal with mucosal thickening and some inflammatory stranding into the adjacent fat. The thickened area of mucosa enhanced vividly and contrast appeared in the lumen during the portal phase. The aetiology of this was uncertain from the CT scan, with possibly an inflammatory pathology being the cause, such as Crohn's disease. The liver was normal and the portal veins were patent. At this point she was transferred to a regional specialist unit.
Following a third endoscopy which found no additional findings, a fourth endoscopy (now four days after the first admission) showed bleeding duodenal varices and an oesophageal varix (not bleeding). Glue was injected into the duodenal varices, which was successful in stopping bleeding overnight but once again she started having large episodes of malaena. A transjugular intrahepatic porto-systemic shunt (TIPS) was subsequently inserted, which although a difficult procedure, was successful in stopping the bleeding. At the same time, a transjugular biopsy of the liver was taken. The histology showed established cirrhosis consistent with alcoholic liver cirrhosis and associated alcoholic hepatitis.
CT scan of the abdomen with IV contrast (images taken in the portal phase): Horizontal section. Arrow points to site of bleeding varices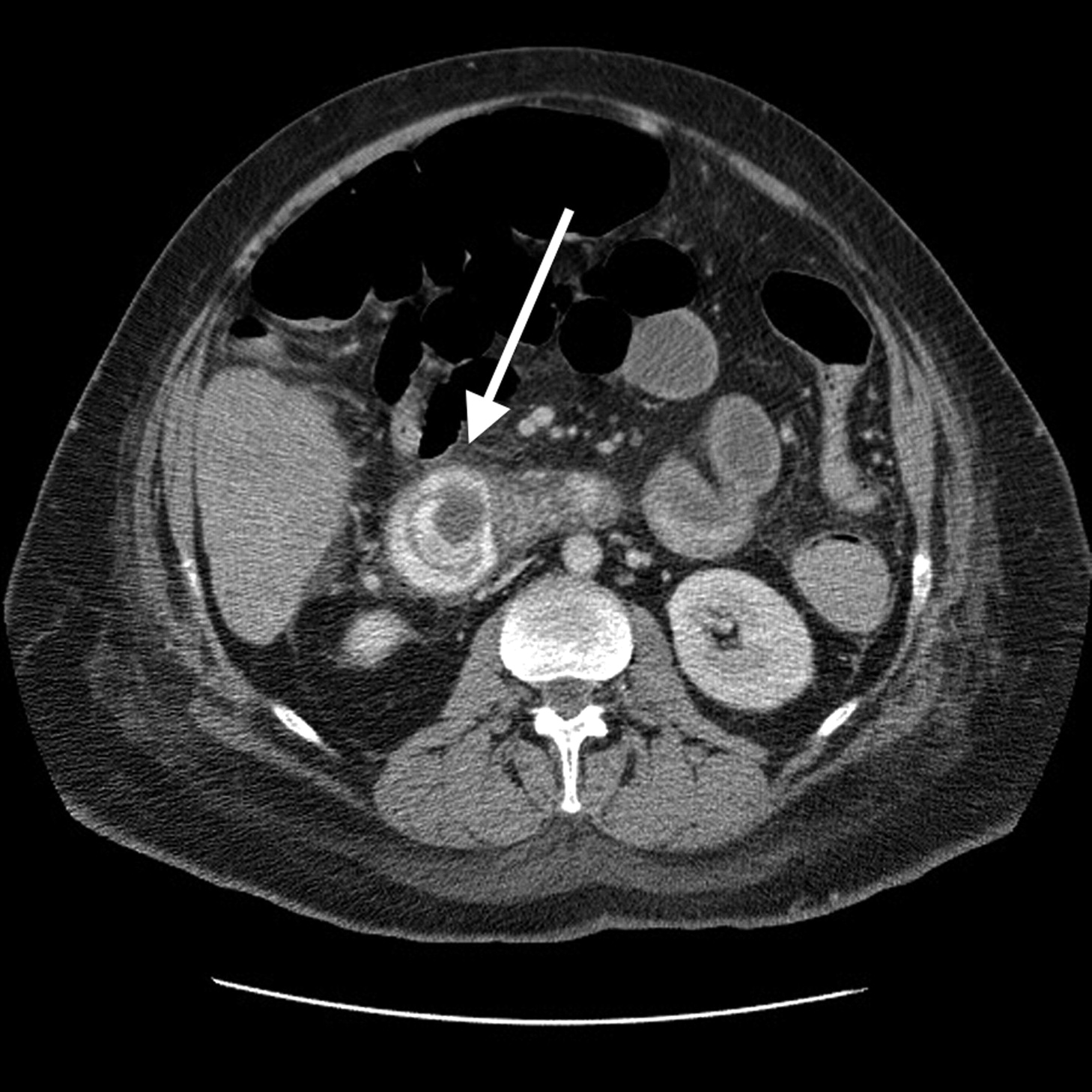
She was difficult to wean off the ventilator because of development of hepatic encephalopathy and so went on to have a tracheostomy. Her abdomen became increasingly ascitic and unfortunately she started passing further amounts of malaena. A tipsogram showed good flow through the stent so no dilatation was needed, however, this was consistent with end stage portal hypertension. She was given intravenous Terlipressiin 1–2 mg QDS during these episodes of recurrent gastrointestinal bleeds following the TIPS procedure.
The malaena subsequently stopped and she has been stable enough to be discharged home.
Discussion
In portal hypertension, collateral venous circulation develops to relieve the portal obstruction. At the sites of anastamosis between the portal and systemic veins, portal hypertension creates engorged veins that can become so dilated that they are prone to rupture. They are not reported to have great physiological benefit to the patient. 1 The most common site for this to occur is at the gastro-oesophageal junction, between the oesophageal vein draining into either the azygous vein or the left gastric vein. Collaterals can actually occur anywhere, where the portal venous system is in apposition to systemic veins. Ectopic varices (varices that occur outside of the gastroesophageal junction) are a rare (5% of all variceal bleeding 2 ) but important cause of gastrointestinal haemorrhage as they may be difficult to diagnose and less amenable to standard treatments due to their inaccessibility. They may occur in the stomach, duodenum, remainder of the small bowel, colon, at the haemorrhoidal plexus, the periumbilical plexus and at stomal sites.
Duodenal varices arise via increased shunting of blood via the portosystemic communication from the pancreaticoduodenal veins via the veins of Retzius to the inferior vena cava. 1 A review of 105 cases found duodenal varices to be most common at the duodenal bulb, the frequency of which decreases the more distally you get in the duodenum. 3 Haemorrhage from ectopic varices is often massive and life-threatening. They account for between 1–5% of all variceal bleeding. 1 Approximately one-third of patients with varices experience haemorrhage. 4 Six-week post variceal haemorrhage mortality is approximately 30%. 5 The prevalence is not well-known. Diagnosis is notoriously difficult as duodenal varices are difficult to identify on endoscopy due to their serosal and submucosal location. 6 The pathology may also not be recognized as it is so rare. Additionally the endoscope may not reach the lower portions of the duodenum. However, endoscopy is crucial in the diagnosis of duodenal varices as it can provide an accurate identification of the source of the bleeding and potential for intervention and treatment in the form of sclerotherapy and banding. Other methods of variceal detection include angiography and transhepatic portography.
Unfortunately there are no randomized control trials relating to the management of this life-threatening condition because it is relatively uncommon. Literature regarding treatment options is thus limited to single cases, or small series. After initial resuscitation and direct treatment of the varices, the mainstay of treatment is to reduce portal pressure either by pharmacological measures or interventional measures if these fail, such as TIPS or balloon occluded retrograde transvenous obliteration. 7
A retrospective study of 21 patients that underwent TIPS for ectopic varices was successful in 19 patients. 8 However, the ectopic varices were still noted to bleed despite a reduction in portosystemic pressure gradient as was the case in this patient. There is also a risk of thrombosis and stenosis. It also increases the risk of encephalopathy and the outcome is still poor.
Conclusion
Coronal reconstruction of CT scan with IV contrast. Arrow points to site of bleeding.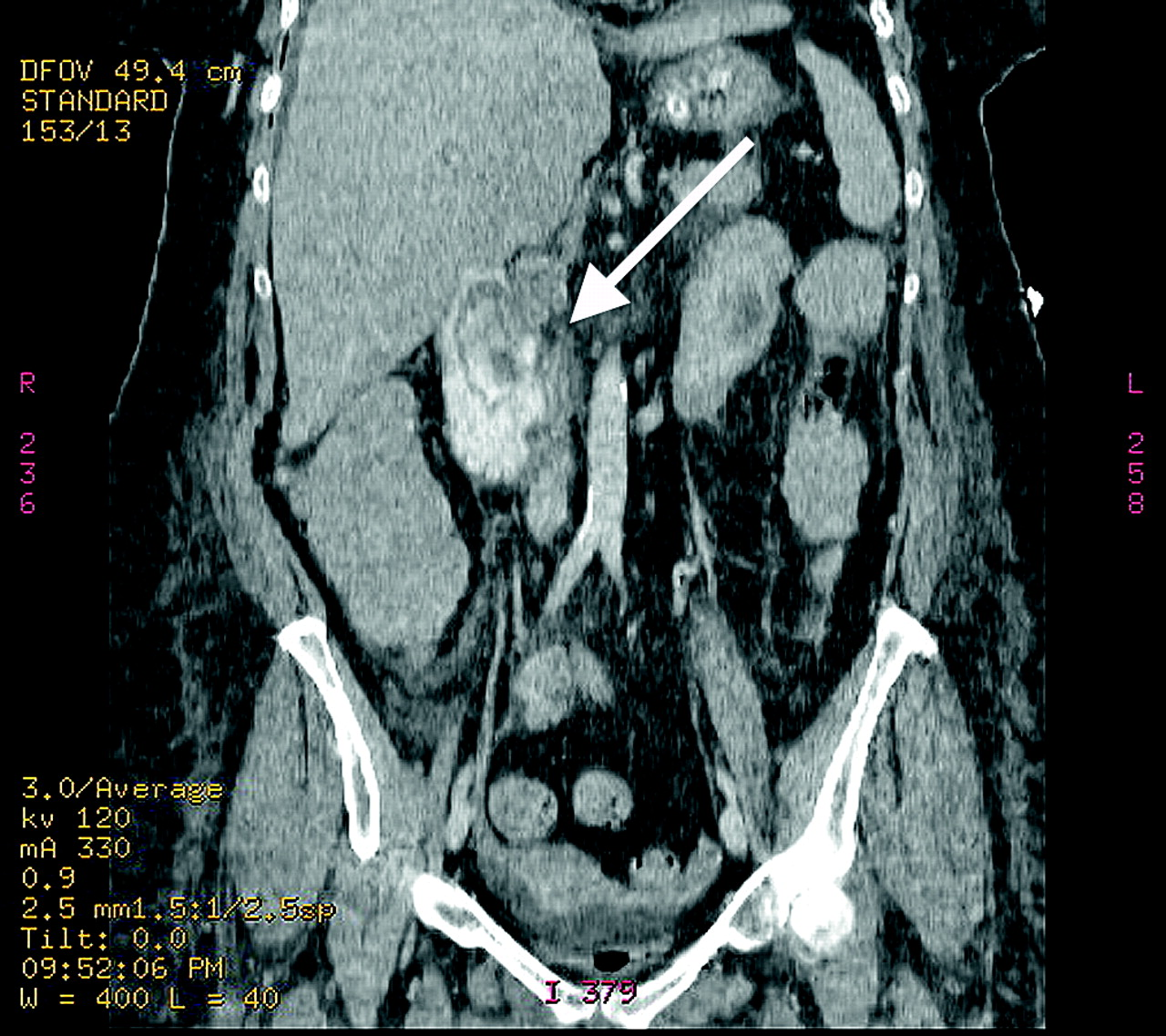
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
Patient consent was obtained