
Abstract

Introduction
In cystic fibrosis (CF), chronic respiratory failure typically develops towards the end of life and represents irreversible organ failure. Traditionally, the perceived futility of invasive mechanical ventilation (IMV) has precluded its use in CF chronic respiratory failure. However, it can be difficult to estimate the relative contribution of acute reversible exacerbating factors and chronic irreversible changes.
DECLARATIONS
None declared
None
Not applicable
PS
Both authors contributed equally
We present the outcome of a 3-year-old girl who was diagnosed with CF during an episode of acute respiratory failure (ARF). She failed to respond to conventional IMV and was treated with extra corporeal membrane oxygenation (ECMO) therapy.
Case report
A 3-year-old Caucasian girl presented to her local hospital with a three-week history of increasing cough and exertional dyspnoea despite treatment with amoxicillin and bronchodilators instituted by her general practitioner. On the day of presentation she had deteriorated further with fever and tachypnoea. On examination there were reduced air entry and widespread inspiratory crepitations, her oxygen saturation was 87% in room air. The initial chest radiograph showed bilateral consolidation, bronchial wall thickening and possible cystic changes (Figure 1).

Initial chest radiograph showing bilateral consolidation, bronchial wall thickening and possible cystic changes
Her past medical history was characterized by persistent cough, steatorrhoea and faltering growth with height and weight on the 3rd percen-tile at presentation having been on the 50th at birth.
Despite five days of treatment with intravenous antibiotics, bronchodilators and facemask oxygen she became more hypoxic and hypercarbic. She was intubated, mechanically ventilated and retrieved to a paediatric intensive care unit (PICU). One day prior to the PICU retrieval a sweat test performed on a sweat volume of 50 microlitres showed a chloride of 101 mmol/L (normal below 40 mmol/L).
Over the next few days, the patient developed septic shock with disseminated intravascular coagulopathy and was treated with colloids, inotropes and blood products. She also received physiotherapy and dornase alfa for copious airway secretions. Nasopharyngeal and tracheal aspirates, as well as blood cultures grew Pseudomonas aeruginosa and antibiotic cover with piptazo-bactam and amikacin was initiated. Aspergillus was isolated on bronchoalveolar lavage and lipo-somal amphotericin added on day 3 of her PICU admission. Nevertheless, her ventilatory requirements continued to rise and inspiratory pressures of up to 45 cm H2O were employed following which a left-sided tension pneumothorax developed on day 4. A pleural drain was inserted and high frequency oscillatory ventilation commenced in conjunction with inhaled nitric oxide. One dose of surfactant was administered via the endo-tracheal tube. Despite these measures her tissue oxygenation remained inadequate with an oxidation index of 45.
Her renal function, echocardiogram and electroencephalogram remained normal and on day 5 of her PICU stay, she was cannulated for veno-arterial ECMO in view of single organ failure and her good premorbid condition. Discussions quoted a 50% chance of survival.
The ventilator was switched to ‘rest settings’ at pressures of 20/10 at a rate of 12 in air, but lung recovery appeared poor on radiographs over the following two weeks. On day 15 a trial off ECMO was unsuccessful with respiratory acidosis despite adequate oxygenation on settings of 35/10, a rate of 40 and FiO2 0.7. In view of continued deterioration in her status a multidisciplinary meeting was convened to discuss withdrawal of therapy. Doubts were raised over the validity of her sweat test since it was performed using a small sample size and under physiological stress. She had been exposed to whole blood products in the ECMO circuit and received packed red cells. For this reason a buccal scraping was taken to confirm the serum genotyping. Both samples revealed homozygosity for the AF508 mutation and a diagnosis of CF was made. Given that she had only just been given the diagnosis and had not benefited from any CF care it was elected to continue the ECMO run and intensify the CF lung care with physiotherapy and mucolytics. On day 19, she had worsening perfusion with continued dependence on high ECMO flows, a broken down neck wound and a deteriorating chest radiograph appearance. A team decision was taken to withdraw her from ECMO on to mechanical ventilation with a view to palliation should this fail.
She was separated from the ECMO circuit successfully and today, the patient is nearly 15 years old and well. Both height and weight plot on the 75th percentile. She has not required any courses of intravenous antibiotics over the past four years and spirometry shows FVC 3.18 L (87% of height predicted) and FEV1 2.6 L (77% of height predicted) with an upward trend (Figure 2).
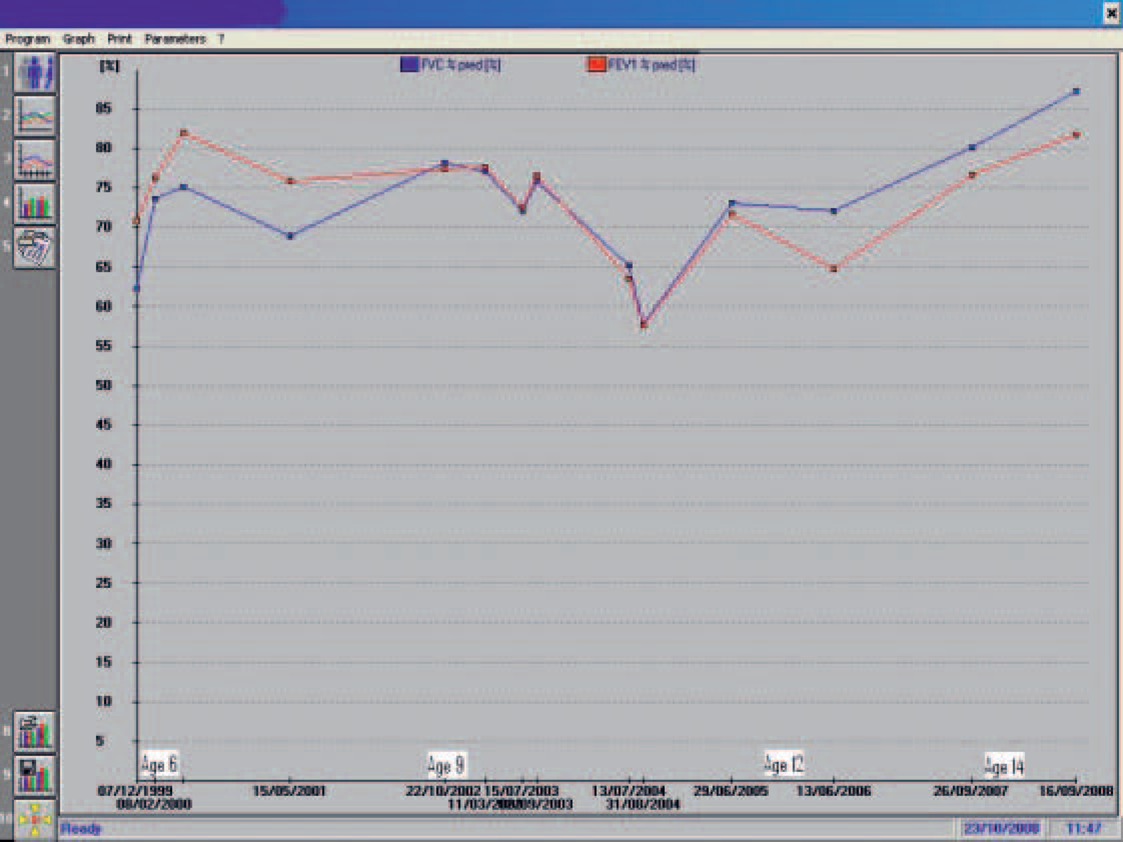
Graph showing the patient's progress
Discussion
This case raises several issues for discussion:
The clinical and economical benefits of a newborn screening (NBS) programme;
The technical aspects of making a CF diagnosis on ECMO;
The use of ventilatory support in CF;
A good outcome following severe acute deterioration requiring ECMO support in a child newly diagnosed with CF.
Newborn screening (NBS)
Clinical benefits
With hindsight, our patient had symptoms suggestive of CF prior to her acute presentation. Newborn screening for CF, pioneered in Australia in the 1980s, was introduced nationally in the UK in July 2007, nearly 15 years after this patient was born. Reservations about the introduction of national NBS for CF included the value of presymptom-atic treatment 1 and the potential high rate of false-positive immunoreactive trypsinogen (IRT) results,2–4 as well as the psychological impact of this disease label in an otherwise healthy newborn.5–8 Evidence of nutritional benefit, 9 improved growth, 10 cognitive function11,12 and survival 13 as well as possible pulmonary benefit 14 is now emerging. Since the landmark recommendation issued by the Centers for Disease Control and Prevention (CDC) in October 2004, 15 NBS programs have proliferated around the world and are soon expected to be in use throughout the USA. 16 In Europe, 19 out of the current 26 programs incorporate IRT and DNA analysis from blood spots on the Guthrie card to reduce the number of children who have to undergo sweat testing.
Economic benefits
A recent cohort study compared treatment costs of 189 children aged 1–9 years who had CF identified by NBS with those of 950 children in the same age group who were diagnosed after clinical presentation. Savings were found to offset the actual costs of the screening program as it currently exists in Scotland. 17
Using our case report as a model, based on current figures, a 19-day ECMO treatment course including assessment, admission and post ECMO phases costs approximately £200,000 (personal communication, ECMO co-ordinator, Great Ormond Street Hospital). When the CF NBS program was implemented in England, funding for the whole screening process to include laboratory costs, giving carrier results and counselling was based on £4 per baby (personal communication, programme manager, UK Newborn Screening Programme), a considerable saving for this individual patient.
Diagnosing CF on ECMO
CF was suspected but not diagnosed when the patient arrived on PICU. The single sweat sample was of low volume for the diagnostic methods at the time and taken at a time of physiological stress. The influence of multiple pharmaceutical agents further complicates the interpretation. A repeat sweat sample on PICU was insufficient, presumably due to sepsis and associated oedema. Non-CF conditions that could have caused transiently elevated sweat chloride levels in our patient include adrenal insufficiency and malnutrition.18
A molecular diagnosis was sought. DNA can be isolated from a variety of sources including anti-coagulated whole blood, clotted whole blood, buffy coat cells, frozen white blood cell pellets, cryopreserved lymphocytes, lymphoblastoid cell lines and buccal epithelial cells. In practice, anti-coagulated whole blood is the most convenient source of cells. Red cells (that do not contain a nucleus and hence no DNA) are lysed and the haeme washed out to avoid inhibition of downstream processes. DNA is eventually extracted from lymphocytes so that packed red cell transfusions are not expected to play a confounding role.
As our patient was exposed to blood products the validity of genotyping via blood sampling was questioned. A blood sample on ECMO showed homozygosity for the ΔF 508 mutation. A faint normal band was also visible on the PCR gel. Since the same band was seen in a control sample, it was concluded that contamination in the laboratory rather than from a blood donor was the most likely explanation.
To confirm this finding, a buccal scraping was obtained. Buccal swabs provide a large yield of high quality DNA from epithelial cells and are easy to collect. Modern analysers like the oligonucleotide ligation assay are sensitive enough to extract sufficient DNA even from small paediatric sample sizes.
Ventilatory support
Respiratory failure remains the leading cause of death in CF. As gas exchange deteriorates, support can be introduced and escalated from oxygen supplementation to more aggressive treatments like non-invasive mask ventilation, IMV and, finally, pulmonary bypass in the form of ECMO or newer pumpless arteriovenous systems.
Non-invasive ventilation
Non-invasive ventilation is used as adjunct to airway clearance techniques and may improve gas exchange during sleep to a greater extent than oxygen therapy alone. Its impact on pulmonary exacerbations and disease progression remain unclear as recently ascertained by a Cochrane review. 19
Mechanical ventilation
For more aggressive interventions, the distinction between chronic and acute respiratory failure is important in determining outcome. Historically, the prognosis for patients requiring IMV is poor with mortality rates as high as 60–90% in the adult population. 20 More recently, IMV has produced higher survival rates in adults. 21
Data about the effect of pretransplant IMV are conflicting. Since prospective studies with randomization are for obvious reasons not ethically possible only retrospective studies with inherent methodological flaws are available. While some centres report no adverse effect on outcome measures including 5-year survival 22 others show significantly worse immediate post-transplant outcomes like early graft dysfunction and prolonged mechanical ventilation as well as higher 1-year mortality. 23 Possible explanations for this discrepancy include selection bias, differences in treatment protocols and timing of transplant.
Short- and long-term prognoses are better in children who are mostly ventilated for acute respiratory failure (ARF). In a study of 31 patients with ARF, age was a statistically significant risk for poor outcome: all five children (under 2 years of age) survived while only seven out of 26 adults survived. When compared with non-ventilated age, sex and genotype matched controls, the ventilated children did not differ in lung function and CF related complications 5 years later. 24 A study with similar design by Garland et al. supports this notion: five ventilated infants all survived and did not differ from their age matched control subjects in number of hospitalizations, Shwachman scores and mortality 1 to 6 years following the ARF episode. 25 Another retrospective cohort study examining the outcome of 33 CF patients requiring IMV also found that older age was the only factor significantly associated with mortality. The mortality for children under the age of 5 years was 22% and only 12.5% for children less than 1 year of age while 5–34-year-olds had a 75% mortality risk. 26
Although our patient had longstanding pulmonary symptoms prior to the acute deterioration it might be assumed that in view of her young age there was relatively less irreversible organ damage. The decision to treat her aggressively is supported by the CF Foundation's recommendation to intubate and ventilate infants and young children with ARF. 27
ECMO
ECMO is used when oxygenation cannot be achieved using conventional ventilation. It carries a significant complication rate in terms of throm-boembolism, haemorrhage and infection. In CF, ECMO has been used successfully as bridge to transplantation 28 and for organ salvage in primary graft dysfunction following lung transplantation in adolescents and adults.29,30 In a 30-year-old CF patient with ARF due to Pseudomonas aeruginosa infection ECMO was used electively to avoid baro-trauma and await resolution of severe bronchial obstruction. The patient was transplanted 26 days after being disconnected from bypass. 31 There is only scanty evidence on its use in children.28,31,32 To our knowledge, the present case is the first report of long-term outcome following ECMO treatment in a young child with CF.
Conclusion
This report highlights an excellent long-term outcome for a child with CF following a life-threatening episode of respiratory failure requiring prolonged ECMO support. Adult data indicating futility of aggressive ventilatory support is based on historical cohorts and relates to patients with chronic respiratory failure. It need not be extrapolated to children with ARF who have a greater potential for recovery. This case also highlights the potential clinical and economical value of NBS for CF.
Footnotes
Acknowledgements
The authors would like to thank all the members of the CF team at the Great Ormond Street Hospital