
Abstract
Introduction
Proximal humeral fractures are common injuries, especially in the elderly population. Palvanen et al. 1 found an increase in the incidence of these injuries of 13.7% per year with an overall five times increase in their incidence between 1970 and 2002. These injuries are generally caused by falls and more than 70% of these patients are over 60 years of age. Seventy-five percent of these injuries occur in women. Most fractures of the humerus in the elderly are treated conservatively. Most of these patients are either discharged from the Emergency Department and followed up as outpatients or admitted to a rehabilitation ward without further surgical review or reassessment of the neurovascular status of the affected limb.
Vascular complications of these injuries are rare, and tend to present acutely. We discuss a case of delayed presentation of a pseudoaneurysm of the subclavian and axillary arteries after a proximal humerus fracture which was treated conservatively. The pseudoaneurysm evolved over a period of two days and required emergency vascular surgical intervention upon diagnosis. This case highlights why these injuries should be managed with a high degree of vigilance, reviewed regularly and referred early for specialist input. It emphasizes the absolute necessity of thorough neurovascular examination when assessing these patients.
Clinical case
An 85-year-old right-hand-dominant woman presented to the Emergency Department after she tripped and fell indoors, striking her left shoulder. Her past medical history revealed a history of mild dementia and osteoporosis. At presentation, her left shoulder was swollen with mild bruising and acutely tender, but she had no other injuries. Motor and sensory examination of the radial and axillary nerves was normal on initial examination.
X-ray studies revealed a Neer Type IV fracture of her left proximal humerus with proximal and medial displacement of the distal fragment into the axilla (Figure 1). Her initial haemoglobin concentration was 14.1 grammes per deciliter (g/dL). She was admitted under the Care of the Elderly medical team for rehabilitation and pain control prior to being discharged home – normal practice for proximal humeral fractures at our institution. No initial orthopaedic or surgical review was sought.
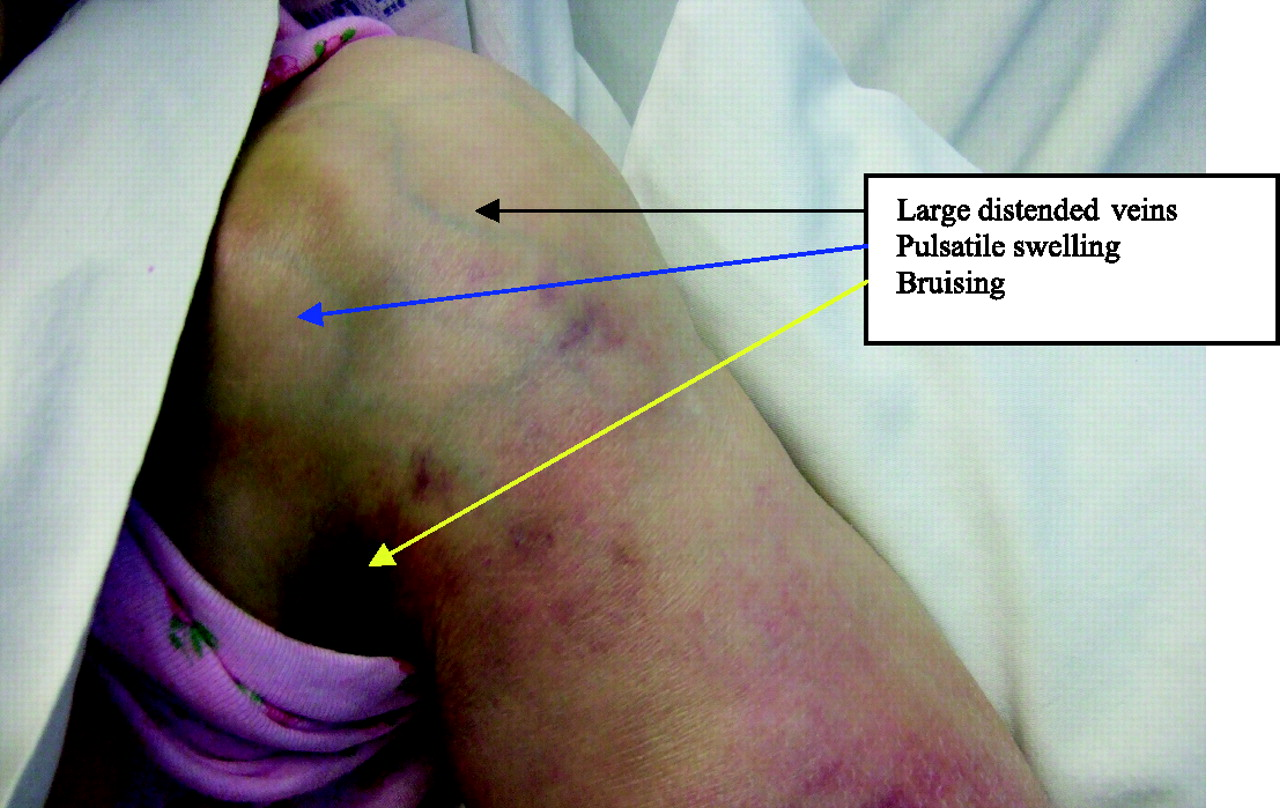
Several hours after admission, bruising developed around her shoulder and her haemoglobin dropped to 9 g/dL at 48 hours after admission. Over the next 24 hours, she developed a large ill-defined tender pulsatile mass on the anterior aspect of her right shoulder. Distended superficial veins were noted overlying this area and distal to it (Figure 2 ). She also developed a motor and sensory radial nerve palsy with weakness of the triceps muscle as well as wrist extensors. Distal pulses were palpable but of decreased amplitude compared to the contralateral side. A clinical diagnosis of an aneurysm of the axillary artery was made.
Duplex Doppler studies and CT pulmonary angiogram (CTPA) showed aneurysmal dilatation of the subclavian and axillary arteries. Flow in the aneurysm was bidirectional but proximal and distal flow were unhindered. Immediate consultation from a vascular surgical team was sought and the patient was transferred to a vascular unit where the aneurysm was treated using an intraluminal stent. This was performed using interventional radiology techniques ( X-ray study on presentation. Neer type 4 fracture of the proximal humerus Clinical presentation of the pseudoaneurysm
Discussion
Proximal humerus fractures are common injuries with an incidence of 73/100,000 of the population. Seventy-five percent of proximal humeral fractures occur in elderly patients. Vascular complications occur in 5% of these cases. 2 Such complications secondary to fractures of the proximal humerus have been recorded in the literature from as early as 1956 3 affecting both adult and paediatric patients. 4 The axillary artery is affected in 5% of cases and is especially vulnerable to damage in its third part at the origin of the anterior and posterior circumflex humeral arteries due to the intimate relationship of this segment of the vessel to the surgical neck of the humerus where most proximal fractures occur. 5 The presentation in all documented cases has been acute with ‘barn door’ signs of a pulseless limb and expanding haematoma around the fracture site – all very classic signs of vascular injury.
Subclavian artery injuries in this setting are much less common. These occur in 0.1% of all patients and are mainly due to atherosclerotic changes of the vessel walls. 6 Axillary-subclavian aneurysms are extremely unusual and are most commonly due to trauma. 7 These often contain thrombus and tend to present with embolic phenomena to the fingers, rupture or thrombosis. 6 Despite the impressive array of modern diagnostic facilities and surgical options available, up to 21% of patients with axillary artery damage may require amputation 8 and this figure rises to 50% in cases of delayed diagnosis. 9 This alone emphasizes the need for vigilant reassessment and for making an early diagnosis in such cases.
In our case the axillary arterial injury was located in its first part and associated with subclavian artery injury. This is not only unique anatomically but also in its delayed presentation. In much earlier studies Drapanas et al. 10 found that 27% of patients with significant arterial injury also had palpable radial pulses and normal capillary refill due to the excellent collateral circulation around the shoulder. O'Gorman and Feliciano 11 showed that 13% of patients with this injury required surgery.
Though there are many non-invasive methods of imaging available such as computerized tomography (CT) angiography, magnetic resonance angiography (MRA) and colour duplex Doppler imaging, arteriography remains the investigation of choice. Its sensitivity and specificity for detecting major arterial injury is 98.3% and 98.5%, respectively, with a positive predictive value of 100%.
12
It has also been shown to reduce the need for unnecessary surgical exploration by 73% in the same study. The other main benefit of arterio graphy is that interventional techniques such as Fluoroscopic image of the aneurysm Successful deployment of the stent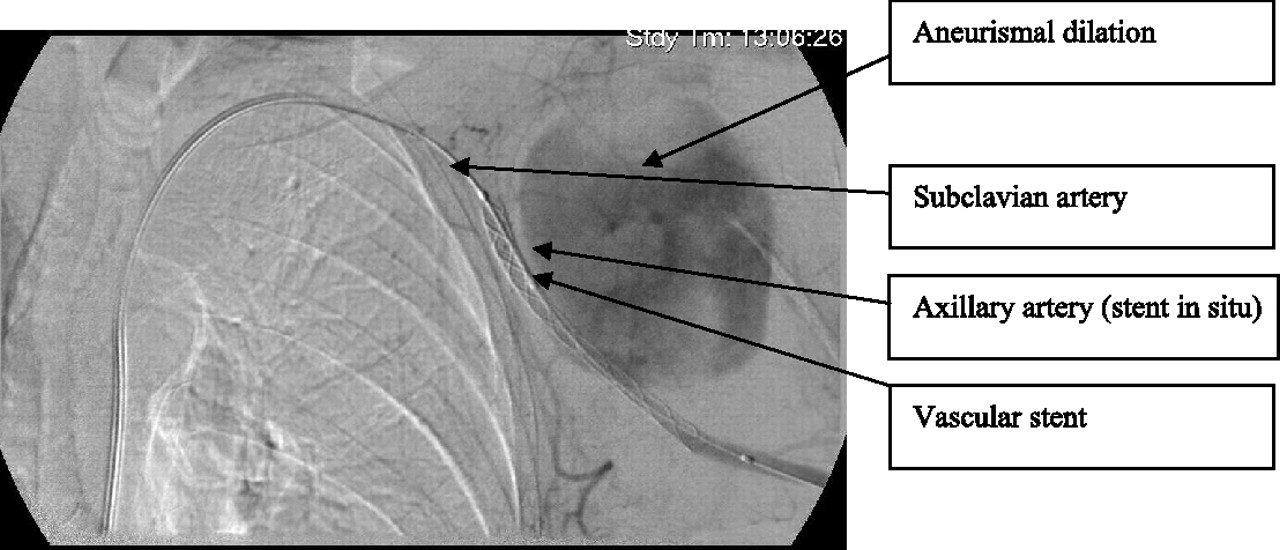

A review of the literature has revealed no reported cases of delayed presentation of axillary-subclavian pseudoaneurysms. The symptoms experienced by our patient included progressive pain and swelling over the shoulder. The signs were those of a pulsatile, expanding tender swelling on the anterior aspect of her shoulder as well as overlying distended superficial veins due to subclavian vein compression. Her ipsilateral radial pulse was present but its magnitude was decreased.
The important learning points from this case are that all such cases should be treated with a high degree of suspicion for vascular injury especially when there is superomedial displacement of the distal fracture fragment as in our patient and they should be regularly reassessed. There is also the possibility that the vascular injury was caused after the initial event by the medially displaced distal fracture fragment and that early surgical stabilization of the proximal humerus might have prevented this. Investigations performed at our unit and the vascular unit suggested that there was no impingement of the bone fragments upon the arteries hence conservative management was advocated in this case.
Signs of vascular injury can appear up to 48 hours after the initial presentation. Associated neurological injuries are often present on the initial assessment of the patient and should not distract the clinician from assessing the vascular system thoroughly. We also recommend regular reassessment over the first 48 hours after presentation by an experienced physician preferably a member of the orthopaedic or vascular team with clear documentation in the case-notes.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
None