
Abstract
Introduction
Sarcoidosis is a systemic inflammatory condition characterized by non-caseating epitheloid granulomata that classically affect the chest. Extra-pulmonary granulomata occur in over 75% of cases, but genitourinary sarcoidosis (GUS) is very rare with just over 60 cases reported. 1, 2 We discuss an unusual presentation of GUS in a patient with known sarcoidosis who developed a testicular mass, and discrete liver and splenic lesions mimicking metastatic testicular cancer.
Case presentation
A 50-year-old Nigerian man who had lived in the UK for 30 years presented to our respiratory clinic with a dry cough and cervical lymphadenopathy for three months. He denied constitutional symptoms or tuberculosis contacts. He was a non-smoker with no significant medical history and took no regular medications. Clinical examination was normal except for palpable cervical and submandibular lymph nodes. His initial blood tests were normal except for raised lactate dehydrogenase (LDH) of 261 IU/L (0–250) and angiotensin-converting enzyme (ACE) of 149 U/L (10–70). His chest radiography demonstrated bilateral hilar lymphadenopathy. He did not attend for Mantoux testing but cervical lymph node biopsy showed confluent non-caseating granulomata staining negative for fungi or acid-fast bacilli, and tuberculosis culture negative. A diagnosis of sarcoidosis was made.
He failed to attend further follow-up preventing monitoring or treatment but re-presented one year later with lethargy, weight loss and a palpable left scrotal mass. Blood tests were normal except for cholestatic liver function; alkaline phosphatase (ALP) of 281 IU/L (30–120), gamma glutamyl transferase (gamma-GT) of 315 IU/L (0–54). Serum ACE was 246 IU/L (10–70) and LDH was 328 IU/L (0–250). Ultrasound scan showed a poorly-defined 9-mm vascular lesion in the left testis with a hypoechogenic centre and several well-defined hypoechogenic lesions within the liver (largest 22 mm). Computer tomography (CT) imaging confirmed these findings with additional well-defined lesions within the spleen (Figure 1) and widespread lymphadenopathy (cervical, supraclavicular, supramediastinal, mediastinal, para-aortic, iliac and bilateral inguinal). Tumour markers were negative (alpha feto protein [AFP], beta human chorionic gonadotrophin [beta-HCG], CA19-9 and carcinoembryonic antigen). Although these lesions could represent systemic sarcoidosis, we felt it important to exclude advanced metastatic testicular malignancy so corticosteroids were withheld.
He underwent left orchidectomy and histology demonstrated non-caseating granulomata
throughout the testis, epididymis and spermatic cord ( Axial computer tomogram of the abdomen showing widespread well-defined lesions
within the liver and spleen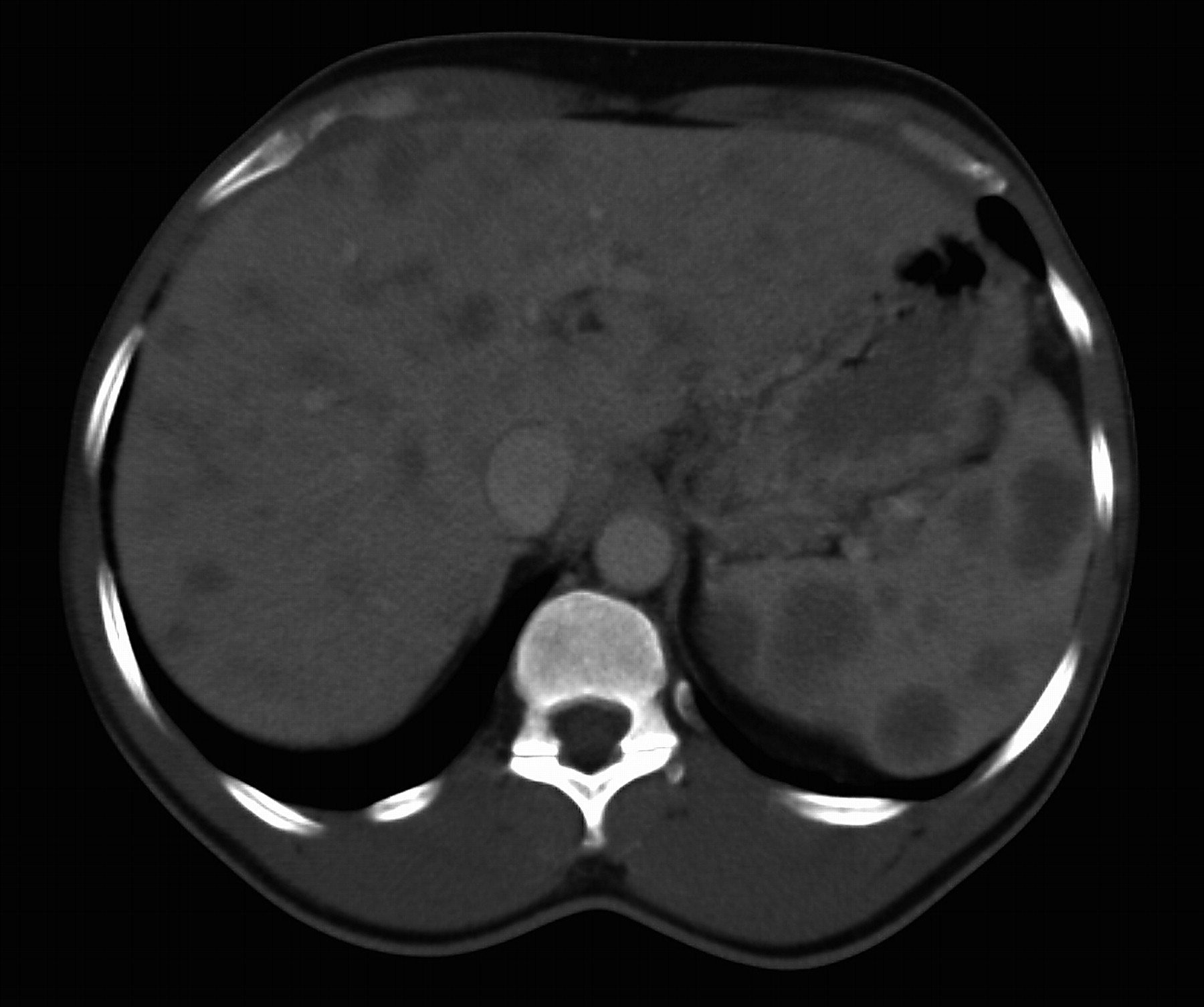
Liver biopsy demonstrated normal liver architecture with no evidence of fibrosis. One periportal and several intralobular non-caseating epitheloid granulomata were identified consistent with liver sarcoidosis.
By the time of histological diagnosis the patient was increasingly fatigued with further weight loss (2 kg), persistent cholestatic liver function and hypercalcuria of 14.85 mmol/24h (0–7.5). He was therefore commenced on corticosteroid therapy (40 mg Prednisolone daily, reducing to 10 mg daily maintenance) with a proton pump inhibitor and bisphosphonate. He had a good response within two months with weight gain of 10 kg, no fatigue, reduced cervical lymphadenopathy and normalized liver function tests. This gentleman remains well two years since starting corticosteroid therapy.
Discussion
There is a recognized association between sarcoidosis and testicular cancer. The incidence of sarcoidosis in patients with known testicular cancer is approximately 100-fold higher than in a matched population of young Caucasian men. 3 However, just 14% have a diagnosis of sarcoidosis before the development of testicular cancer. 4
GUS can present with many testicular symptoms from acute pain to painless swelling;with or without constitutional symptoms. We describe the second case of GUS presenting in association with discrete liver and splenic lesions mimicking metastatic testicular cancer, however, our patient had known sarcoidosis and subsequently developed testicular swelling with new adenopathy. 5
A testicular mass has many differential diagnoses including testicular malignancy. Cancer markers (AFP, beta-HCG and LDH) and a chest radiograph should be arranged but inguinal orchidectomy with CT staging is the primary management for most patients with a testicular mass suspicious of tumour. 6, 7
Clinical features suggesting a benign diagnosis of GUS include bilateral lesions and Afro-Caribbean ethnicity (three-fold higher incidence of GUS; just 3.5% of total testicular cancer cases). 1, 2, 8 Sarcoidosis is not known to cause false-positive results for AFP or beta-HCG serum levels and should be baseline investigations. 9 Conversely, as in our case, sarcoidosis can cause a raised LDH and is not a reliable diagnostic test for testicular malignancy. 9
Imaging is central to investigating testicular lesions but poorly differentiates between
GUS and malignancy. The most common sonographic finding in GUS is a hypoechoic mass
affecting the testis or epididymis but this is not specific to GUS and a coarsened
testicular echo-texture is also described.
10,
11
Testicular cancer can metastasize to the mediastinum causing adenopathy on CT
imaging but this is rare without associated retroperitoneal lymphadenopathy.
4
Microscopic testicular cancer metastases are also associated with a sarcoid-like
granulomatous reaction that can cause mediastinal adenopathy.
4
Additionally (as in our case) Light micrograph of histological specimen from left orchidectomy demonstrating
non-caseating epitheloid granuloma. Seminiferous tubule is seen to the right of
the image (haematoxylin and eosin stain; original magnification x 100)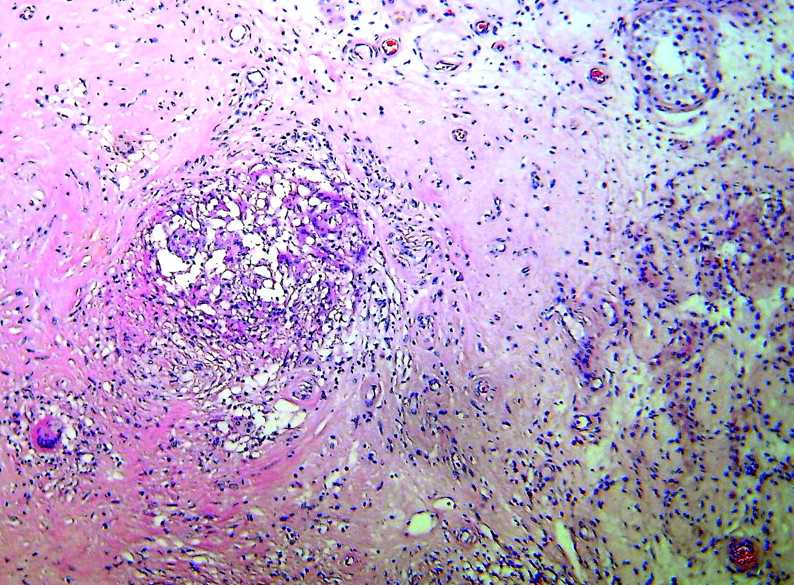
Histological examination remains the most reliable way to confirm sarcoidosis and orchidectomy is the primary radical treatment for testicular mass suggestive of tumour. When deciding to biopsy or remove the affected testis, conserving fertility and testicular function must be considered through sperm storage and avoiding unnecessary orchidectomy. In one GUS case-series 45% underwent biopsy, 35% radical orchidectomy/epididymectomy and 20% clinical surveillance. 2 There are various approaches to testicular biopsy but they must consider potential malignant diagnoses, avoiding potential seeding of malignant cells. An inguinal approach open biopsy with intra-operative clamping of the spermatic cord allows intra-operative frozen sections for histological examination (and potential testicle preservation) but can progress to radical orchidectomy if biopsy is equivocal or suggests malignancy. 12 Other centres advocate radical orchidectomy whenever there is a potential diagnosis of testicular malignancy to preventdiagnostic delays or errors. 13
Corticosteroids are indicated in GUS as they can reduce testicular pain and improve associated azoospermia. 14, 15 Our patient had also developed constitutional symptoms and hypercalcuria. 16
All physicians who manage patients with sarcoidosis should be aware of GUS and the association between sarcoidosis and testicular cancer. We have discussed clinical parameters that indicate the benign diagnosis of GUS but histological examination remains the most reliable way to exclude malignancy.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
The authors would like to thank the patient for allowing us to write this report. The authors would also like to thank Steven Hazell (Consultant Histopathologist, Imperial College Healthcare NHS Trust, London) for preparing the histological image