
Abstract

Celebrating 20 years of breast screening
Breast screening with mammography was introduced in the UK in 1988, and the Annual Review 2008 from the NHS Breast Cancer Screening Programme (NHS BSP) summarizes the 20-year experience.
Twenty years is a long time and it seems reasonable to ask what might be expected from such a review from a public health institution. First and foremost, one would expect to see an analysis that shows that screening has lowered breast cancer mortality in the UK. Secondly, one would wish to see a comparison of this benefit with a quantification of the most important harms, as this would allow the readers to judge for themselves whether the programme has been worth its large cost.
If the screening programme had lived up to the expected mortality reduction that was the basis for its introduction, it should have been easy for the NHS Breast Cancer Screening Programme to demonstrate this for the politicians and other interested parties.
This is not what the 26-page publication does, however. It celebrates 20 years of breast screening, as one of the headlines says. 1 As with all good birthdays, it is the qualities of the celebrated that are mentioned, not the shortcomings. In line with the positive framing, the first sentence in the Review refers to the 20th anniversary as a ‘momentous occasion’. The Review exaggerates the benefit, omits the harms, and looks like propaganda aimed at persuasion. It comes wrapped in a beautiful layout that would pride any marketing department if it had been a sales brochure for a drug (Figure 1). The first words on the cover page are: ‘Saving lives through screening’, and the symbolism is strong. Most of the cover space is taken up by a picture of a delicate rose in the distinctive pink colour that has become iconic for the fight against breast cancer. The rose is transparent, symbolizing the scientific illumination and radiological technique through which the programme operates.
Does screening save lives?
There is nothing as convincing as the demonstration that an intervention saves lives. We think that the Annual Review's failure to demonstrate this is because it is not possible.
Highlighted on the first page of the report is a statement that the ‘NHS Breast Screening Programme is now estimated to save 1,400 lives each year’. This message has appeared elsewhere and is effectively used as a shield or mantra in public announcements to counter criticism of the programme. 2, 3 The 1400 lives saved are called a ‘key fact’, and one would therefore think that this estimate comes from a scientific publication. However, the reference offered in its support is to another NHS BSP publication, which has not been peer-reviewed. 4 This reference states: ‘the totality of the evidence from randomised trials shows that regular mammographic screening commencing at ages 50–69 years reduces mortality from breast cancer by about 35%’. 4 There is no explanation how the 35% estimate was derived, but the report states later on that breast cancer mortality is reduced ‘from 8.0 to 5.2 per 1,000 women in the target age range if they are regularly screened over a 10-year period’. 4 The origin of these rates is not explained either, but the reduction equates to 35%.
It is not possible to save 3 women out of 1000 from dying from breast cancer through 10
years of screening. An overview of the Swedish mammography screening trials showed a
reduction in breast cancer mortality of 29% and reported that 1 per 1000 women was saved
after 10 years.
5
A more recent overview of The cover page from the NHS Breast Screening Programme Annual Review
20081

If the expectations from 1986 had been met and screening had reduced breast cancer mortality by 35% ‘in the targeted age range’, 4 it should have been easy to see this in national mortality statistics. However, real-life statistics tell a different story (Figure 2). The decline in breast cancer mortality after 1989 was 41% in women aged 40–49 years, who were not invited to screening, 41% in women aged 50–64 years who were invited from 1988, and 38% in women aged 65–69 years who were invited from 2001. 10 Further, the drop in breast cancer mortality in the relevant age group began before the screening programme started and was largest in the age group too young to be screened, if the whole observation period is considered (Figure 2). 10 This suggests that if screening has had an effect on breast cancer mortality in the UK, it must have been small. It seems impossible that the NHS Breast Screening Programme could have saved anywhere near 1400 lives each year, as there were 3500 annual deaths from breast cancer in the relevant age range in 2003. 4 Most of the pronounced decline in breast cancer mortality is likely caused by improved treatment, which can explain why it has been similarly large among the young women who have not been invited to screening. Other factors, such as increased ‘breast awareness’, may also have contributed.
Data from other countries support the findings from the UK. In the European Union, the decline in breast cancer mortality has been considerably larger among young women who are not invited to screening than among those who are invited (13.5% versus 9.8%). 11 In the USA, it has been estimated that screening has led to a 15% reduction in breast cancer mortality, 12 but this result is likely a random high, as there has been an unusually large change in the mortality curve in USA that coincided with the introduction of screening. 13 Sweden introduced screening in 1986 and has one of the longest running programmes with one of the highest attendance rates, but the mortality curve has been slowly declining for over 35 years, with no visible change in the trend in the screened age group. We will soon present detailed data on breast cancer mortality in Sweden before and after mammography screening.
Breast cancer mortality in the UK. The vertical dotted line indicates the start
of the NHS Breast Screening Programme (from 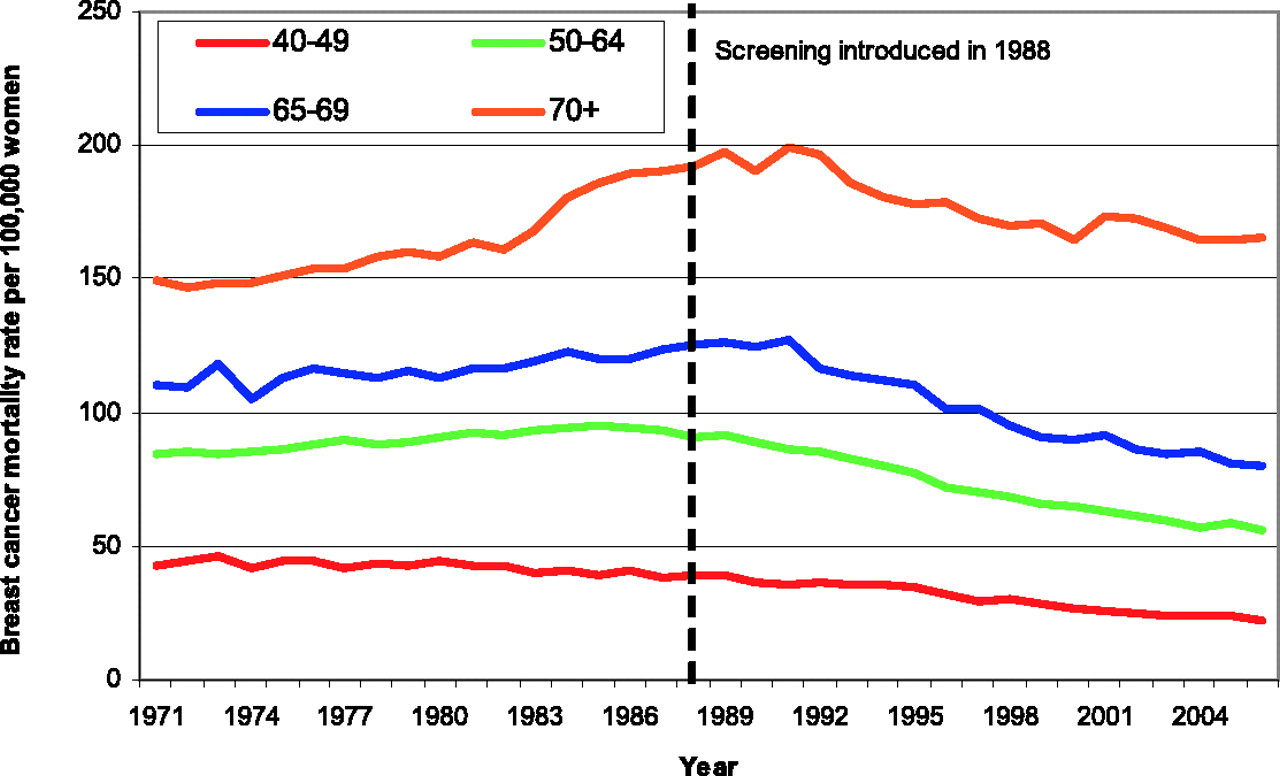
Overdiagnosis
The most serious harm of screening is over-diagnosis and overtreatment of healthy women
who would not have acquired a breast cancer diagnosis in their lifetime if they had not
attended screening. The Annual Report does not mention overdiagnosis at all.
1
We have estimated that, in the randomized trials, about one in four diagnoses
are overdiagnosed cases.
7
In England and Wales, about one in three of the cancers in the screened age
group are unnecessary diagnoses.
14
As 21,683 women were diagnosed with breast cancer in 2006 in the invited age
group (50–69 years),
15
this is equivalent to about 7000 unnecessary breast cancer diagnoses per year in
the UK.
1
The Review not only ignores this harm, it converts it into something positive:
‘A huge number of breast cancers, over 100,000, have been detected since 1988,
highlighting the importance of the screening programme in the early detection of breast
cancer in England’.
1
However, it cannot be an objectivein itself that the programme
detects many breast cancers. The objective must be to reduce mortality from the disease,
and it is quite possible to detect too many cancers. This is an example
of ‘the popularity paradox’: the more harm through over-diagnosis, the more efficient
screening is perceived to be.
16
It should be clear to anyone who looks at the data that screening leads to a
substantial and persistent increase in breast cancer incidence, and that the additional
breast cancer cases in the screened age group has not been compensated by a decline in
incidence when the women pass the age limit for invitation ( Breast cancer incidence per 100,000 women in the UK. Horizontal dotted lines
are linear regressions projecting the pre-screening trends using 1975–1987.
This is to allow comparisons of observed and expected incidence rates in the
age groups that could be affected by screening mammography (from 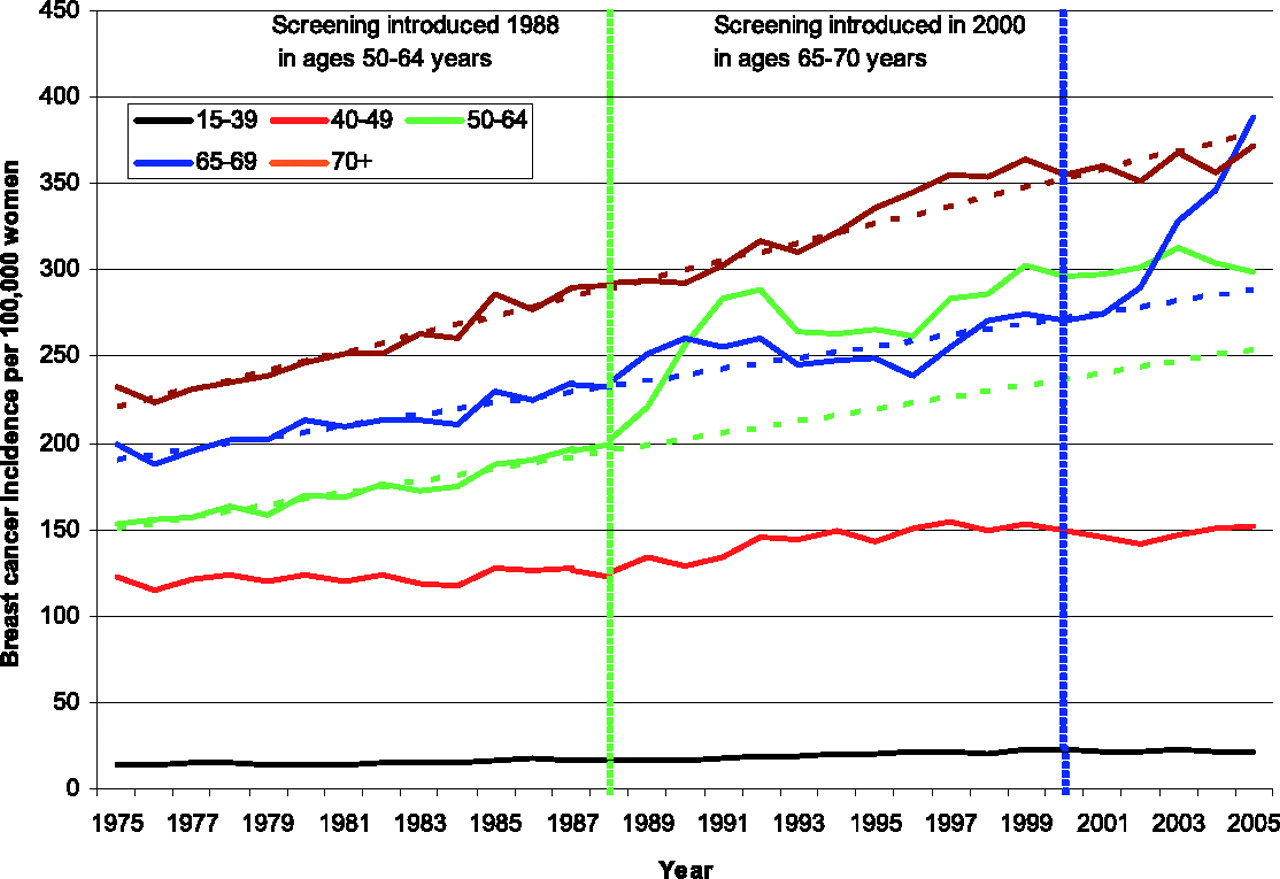
False positives
The second major harm of cancer screening is false-positive findings, but the text of the Review does not mention or quantify false-positive recalls. 1 It notes in a table that there were 83,728 recalls in 2007, 1 but these include both true and false positives. The Review also notes in a table that 14,753 breast cancers were detected in 2007, but does not mention that this means that about 70,000 women experienced a false-positive recall. It has been estimated that about 20% of those invited will have experienced a false-positive recall at some point after 20 years of screening 17 but the report downplays the risk of being recalled as 8.6% for first-time attendees and 3.6% in subsequent rounds. Being recalled raises a suspicion of a potentially life-threatening disease and has serious short- and long-term psychological consequences. 18 An annual review of a screening programme should describe in detail a serious harm that affects one in five invited women in 20 years.
Biopsies and mastectomies
Biopsies can be either surgical excisions or needle biopsies. The Annual Review is not specific about this, but another NHS report notes that about 40% of those recalled in the UK will undergo cytology and/or needle biopsy and that 3% are referred for surgical excision. 4 Surgical excisions remove the whole lesion from the breast. They are called ‘benign biopsies’ in the Review, are specified as surgical biopsies that turned out to ‘be clear’ in Table 7 of the Review, and are quantified in Table 1 to have affected 1676 healthy women in 2007. 1 We believe that, although a lesion proves to be benign for the pathologist, it is not benign for the woman who undergoes a surgical excision on a false suspicion of cancer. Furthermore, this harm is downplayed as affecting 0.1% of those screened per year. The risk should have been related to 10 screening rounds, in order to make it comparable with the beneficial effect. For comparison, we have calculated that the exaggerated mortality benefit mentioned in the Annual Review also amounts to 0.1% of those screened, but in this case over 10 years, 5 and the small absolute risk reduction is not mentioned in the Review. The number of needle biopsies is not presented either but is much larger, 17 affecting about 40% of the 70,000 false-positive recalls, or 28,000 (70,000 × 40%) unnecessary needle biopsies per year. 4
It is far worse than ‘benign biopsies’ to lose a whole breast because of overdiagnosis. Screening leads to 20% more mastectomies than there would have been in the absence of screening, 7 and 29% of carcinoma in situ cases are treated by mastectomy, 1 although less than half of them would ever have developed into invasive cancer. 19 The report presents no data on the absolute number of mastectomies although this number increased by 36% for invasive cancer and by 422% for carcinoma in situ from 1990 to 2001 in the UK. 20
Misleading survival statistics
A quote from Professor in Statistics, Stephen Duffy, is highlighted in the review: ‘The 10-year fatality of screen-detected tumours is 50% lower than that of symptomatic tumours’. 1 This headline comes with no caveats. But using a 10-year fatality rate is seriously misleading. This is well-known 16, 19, 21, 22 and was recognized already in the Forrest report in 1986 that paved the way for screening in the UK. 9 It has also been described by Consultant in Public Health for the National Screening Programmes, Angela Raffle, and the former Director of the National Screening Commitee, Muir Gray:
‘The kind of people who come for screening, and the kind of disease that is easy to find with screening, add up to a highly selected group with regard to both the overall health and longevity of the individuals and to the benign natural course of the uncovered pathology. The combined effect is a very favourable prognosis. Outcomes in screened people will therefore be very good, whether or not screening makes a difference.’ 16
Screening primarily detects slow-growing cancers (length bias), and overdiagnosed cancers have an excellent prognosis. Survival of women with screen-detected cancers is therefore very good, e.g. 97% in the Malmö screening trial after 10 years. 23 The Annual Review from the NHS Breast Cancer Screening Programme is edited by its director, Professor Julietta Patnick. 1 It is embarrassing if Duffy and Patnick, in their positions as professors working with screening, are not aware of this fundamental bias, and even worse if they are aware of it but mislead their readers by being quiet about it.
Looking into the crystal ball
The opening statement in the Introduction reads: ‘In this year's annual review we look back at how the programme has evolved over time, and look forward to the future developments that will deliver even greater benefits to thousands of women in the years to come’. 1 This is marketing speak and says nothing about the thousands of women that will be harmed. Furthermore, the statement is unduly optimistic. It has often been argued that because of substantial improvements in therapy, the effect of screening is probably less today than when the trials were performed. If this continues, we will see fewer benefits in future, not more. Furthermore, increased sensitivity and detection rates will be expected to lead to more overdiagnosis and the balance between benefits and harms will likely also become less favourable by the extension of the NHS BSP to include women aged 47–73 years, announced in the Annual Review. 1
Digital mammography is described as ‘the latest technology and the best for detecting abnormalities in the breast tissue of premenopausal women’. 1 However, there are no randomized trials evaluating digital mammography in a screening setting and premenopausal women often have benign breast abnormalities. Few premenopausal women are invited to screening, and the available evidence indicates that digital and film mammography perform similarly in women aged over 50 years in a screening setting. 24 Even if digital mammography were better at detecting small lesions, this does not necessarily translate into improved outcomes, and it could lead to more false positives, more biopsies and more overdiagnosis. We are told that ‘100m [£] will be invested in digital mammography equipment in 2008’. This is an impressive investment when so little is known about the cost-benefit balance.
What happened with informed consent?
Throughout the Review, there are clear indications of a ‘right’ and a ‘wrong’ choice about attending. For example, ‘The aim is to increase the level of invitation acceptance in target populations, by continuing to support women to make the right choice for them’. This explicit aim goes directly against a decision in the National Screening Committee that ‘the purpose of information about screening is to allow individuals to make an informed choice about whether to participate’, 25 and it seems that there really is not any choice, as the ‘right’ choice clearly is to get screened. This paternalistic approach clashes with today's emphasis on autonomy in healthcare and the requirement for full disclosure of the potential harms. 26
Professor Julietta Patnick writes that: ‘Despite the successes of the last year, we have however seen the acceptance of screening invitations across the general screening population decrease slightly (by 1.1%). The fall is seen in all target age groups but the drop in acceptance of the first invitation is particularly worrying, as the evidence shows women who accept the first invitation are most likely to be regular attendees.’ 1 It is problematic that the director of the programme describes declining attendance as ‘worrying’. The programme has important harms and it is not clear that the benefits outweigh them. The recent development may therefore simply indicate that more women are making informed choices because of the public debate.
It is stated in the Review that the NHS should provide material that allows the decision to be ‘based on balanced factual information’. 1 The Review itself and the information leaflet that is provided to women invited to screening in the UK by the NHS BSP document a huge discrepancy between this principle and actual practice. The information leaflet does not mention overdiagnosis at all and it directly encourages participation. 27
Selling screening
Sheraton Hotels and many other enterprises operate with the term ‘preferred customer’. If you are loyal and do what is expected of you, you are a preferred customer. This is an effective sales strategy, as few would wish to be a non-preferred customer, and the Annual Report has not resisted the temptation. It features an interview with a woman named Dorothy Adams. In advertising, drawing forward a loyal individual who is a satisfied customer is an effective sales strategy.
Dorothy says: ‘I know how important it is to have regular checks and to make sure you accept your invitations or make your appointment’. 1 This happy and faithful customer has even continued to request screening beyond the invited age range (and beyond what is supported by evidence). It is described how ‘Women like Dorothy … have attended without fail for decades’. 1 Clearly, not accepting the invitation is a failure. This is underlined by the omission of Dorothy's surname, which conveys a sense of familiarity and a sense of belonging to the regular customers' executive club.
We are also told that: ‘Dorothy Adams was the first person ever to attend the North Staffordshire Breast Screening service 20 years ago. Since then she has never missed an appointment, seeing it as an important part of her wellbeing and a valuable health entitlement. Now a grandmother, Dorothy is passing on her knowledge and experience to her daughter and granddaughter to help them make decisions about screening when the time comes.’ 1 There can be little doubt about what the ‘right’ decision will be for Dorothy's offspring. Paternalism prevails in the NHS BSP, rather than respect for autonomous free choice, informed consent, and provision of honest and balanced information.
Unlike Sheraton Hotels, where the Directors can be held personally accountable for shortcomings and omissions in their Annual Report to tax authorities and shareholders, it is unclear who is accountable for an Annual Review of a public health programme where the costs are much greater than just monetary.
The Annual Review provides support to our suggestion 27 that those who are responsible for a screening programme should not be the same as those who provide information material about the programme or review whether or not the programme has been a success.
Conclusions
We arrive at a different conclusion than those who wrote the Annual Report. There is no convincing evidence that it has saved lives. In fact, the effect of 20 years of screening in the UK is not visible in the mortality statistics. In contrast, there is solid evidence of serious and common harms, and the screening programme is very costly. Does this not mean that it is time for an impartial review of the justification for mammography screening?
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
None