
Abstract

Case report
A 40-year-old male plasterer presented to hospital with swollen arms. On direct questioning he reported a 3-kg weight loss over the last 6 months despite a normal appetite; he had no bowel symptoms and no night sweats. There was no significant past medical history. On examination he appeared cachectic and had bilaterally swollen arms, gynacomastia and axillary lympadenopathy. The remainder of the examination was unremarkable. Blood tests revealed an iron-deficiency anaemia and raised inflammatory markers (haemoglobin 10.0 g/dL, mean corpuscular volume [MCV] 67 fl, erythrocyte sedimentation rate 106 mm/hour, C-reactive protein 91 mg/L). A CT scan of the chest, abdomen and pelvis revealed bilateral arm DVTs, axillary and abdominal lympadeonopathy, which was thought to be reactive. The patient was started on Warfarin and iron tablets, and discharged from hospital.
He was reviewed two weeks later in the gastroenterology outpatient clinic to further investigate the cause of his iron-deficiency anaemia. A gastroscopy and colonoscopy were arranged and revealed a grossly normal oesophagus, stomach, duodenum and colon. The CLO-test was positive and he was started on a course of helicobacter pylori eradication therapy. Biopsies taken from the duodenum, showed normal villi with non-caseating granulomata, providing a differential diagnosis of Crohn's disease, TB and sarcoidosis. The patient had been vaccinated against TB as a child and had a BCG scar on his left arm. A serum ACE, ELISpot-Plus and TB sputum culture were taken and were all found to be negative. Coeliac serology was also negative.
When next seen in the gastroenterology outpatient department he had lost a further 6 kgs in weight and was visibly cachectic despite a normal diet and appetite. Cardiovascular examination was normal, no murmurs were heard and the JVP was not raised, respiratory and abdominal examinations were unremarkable but axillary lympadeopathy persisted. Blood tests revealed his iron deficiency anaemia had progressed, his haemoglobin was now 7.7, MCV 67 and iron level 2. ECG was normal. He was admitted to hospital from clinic for further investigation. A repeat abdominothoracic CT scan showed axillary lympadenopathy, thickening of the pericardium with areas of calcification ( Pericardial calcification in Whipple's disease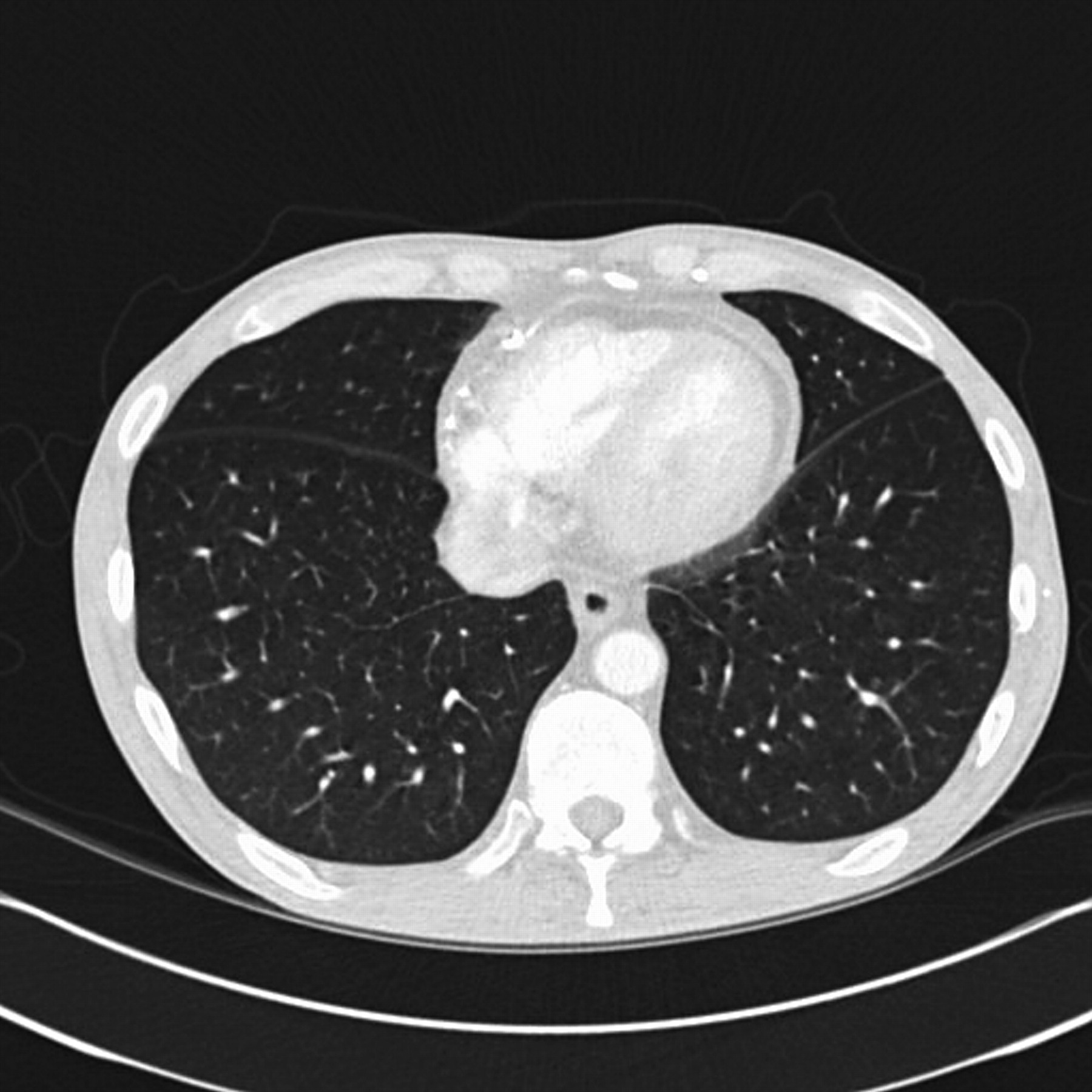
Discussion
Whipple's disease was first described by George Whipple in 1907. It is a rare disease caused by the bacillus Tropheryma Whipplii. Patients classically present with migratory arthralgias, weight loss, malabsorption, diarrhoea, lympadenopathy and abdominal pain but the disease may affect any part of the body.
Whipple's disease can affect the heart in multiple ways, most commonly causing a pericarditis, but there are also reports of myocarditis, valvular endocarditis and coronary arteritis. The prevalence of cardiac involvement in Whipple's disease is unknown but one series of 19 patients reported that 58% had clinical cardiac findings and 79% had gross cardiac lesions at postmortem. Histological changes in the heart are identical to those seen in biopsies of the gut and electron microscopy has demonstrated the presence of the rod-shaped bacteria within the heart tissue. 1 Pathologically the bacteria cause a chronic inflammatory reaction, which results in fibrosis which may affect any of the layers of the heart. 2
In this case pericardical calcification was noted on the CT scan two years after initial presentation to hospital and just prior to formal diagnosis and commencement of antibiotic therapy. These findings are consistent with other reports which have noted that although there does not seem to be a clear relationship between cardiac involvement and the severity of the systemic disease, in most cases Whipple's disease has been present and untreated for number of years.
Unusually this patient was completely asymptomatic from his pericarditis, with a normal cardiovascular examination and ECG. Cardiac involvement in Whipple's disease is a rare finding in life but a relatively common postmortem finding. Death from cardiac Whipple's disease is a result of heart failure secondary to constrictive pericarditis or myocarditis or is a result of arrhythmias due to fibrosis of the conduction pathways. 3 This case report demonstrates that computer tomographic imaging can be useful in detecting early pericardial calcification in Whipple's disease prior to the patient being symptomatic. Due to the significant mortality of cardiac Whipple's disease we should, as clinicians, remain vigilant for any signs of cardiac involvement, so additional treatment or monitoring can be instigated early in the disease course.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
None