
Abstract
‘A main cause of philosophical disease – a one‐sided diet: one nourishes one's thinking with only one kind of example.’ Ludwig Wittgenstein
Introduction: when non‐RCT evidence is sufficient to conclude that the intervention caused the outcome
High quality randomized controlled trials (RCTs) (concealed allocation, relevant groups blinded and sufficiently powered, etc.) will usually provide sufficient evidence to establish that a particular treatment caused an outcome. Yet sufficiently well‐conducted RCTs are rare. 1 Trials can be under‐powered, 2 or unsuccessfully blinded, 3, 4 and often suffer from many undetected biases. The results of most RCTs are therefore often insufficient to establish causation. At the same time, RCTs are often not required to establish causation. 5 Treatments including the Heimlich manoeuvre, cardiac defibrillation and parachutes to prevent death 6 have never been tested in RCTs, yet their effectiveness is surely strongly supported by evidence.
Evidence‐grading systems that place randomized trials at the top of a hierarchy 7, 8, 9, 10, 11, 12, 13 will deliver misleading conclusions in cases where RCTs are insufficient or unnecessary. According to these hierarchies, trails of homeopathy – often generating positive results and generally of higher quality than RCTs of conventional treatments 14 – will be considered to provide strong evidence, whereas the evidence base for the Heimlich manoeuvre to unblock airways and parachutes to prevent death will be judged as less strongly supported by evidence.
Sir Austin Bradford Hill, in a widely‐cited ‘pre‐EBM’ system for appraising evidence, suggested that several relevant factors must be considered before concluding causation. We investigated and revised the Bradford Hill ‘guidelines for causation’, in order to refine our intuitions about whether to believe that intervention is effective. Our intention is not to debunk previous attempts to grade evidence, but rather to contribute to their natural evolution and development.
Revising Bradford Hill's guidelines
Bradford Hill's original guidelines and proposed revisions
Direct evidence from studies (randomized or non‐randomized) that a probabilistic association between intervention and outcome is causal and not spurious;
Mechanistic evidence for the alleged causal process that connects the intervention and the outcome;
Parallel evidence that supports the causal hypothesis suggested in a study, with related studies that have similar results.
A previous attempt to impose a structure on the guidelines 15 may have oversimplified, claiming, for example, that ‘analogy’ (our ‘similarity’) is a ‘mechanistic’ consideration (which, as shallbecome clear below, is a category error).
We use the term ‘guidelines’ over the more common ‘criteria’ 16, 17, 18, 19, 20, 21 because Bradford Hill did not regard any of the guidelines as necessary or sufficient for establishing causation 11 : ‘… none of these viewpoints can bring indisptuable evidence for or against a cause‐and‐effect hypothesis and equally none can be required as a sine qua non’. 22 To cite his example, ‘It will be helpful if the causation we suspect is biologically plausible, though this is a feature we cannot demand. What is biologically plausible depends on the biological knowledge of the day.’ 22 Bradford Hill gave similar warnings about all the other guidelines (except, as we shall see, ‘temporality’). Rather than ‘criteria’, they are best viewed as factors to be considered when assessing whether there is evidence for causation, or ‘guidelines’ for short.
Aware of detailed descriptions of the original guidelines, 15,, 23, 24 we shall limit ourselves to describing our re‐structured and revised version (Table 1). We shall then apply the Revised Bradford Hill Guidelines to real examples of likely causation despite lack of support from RCTs.
Direct evidence
The first three of the revised guidelines help assess whether ‘direct’ evidence of a probabilistic association between two factors is causal rather than spurious.
Size of effect not attributable to plausible confounding
Plausible confounders are factors which are not directly related to the experimental intervention, are unequally distributed between treatment and control groups, and are likely to determine the outcome. For instance, we might observe that depressed people who exercise recover more quickly. Is the association between exercise and more expedient recovery from depressive symptoms causal? We cannot answer this question without ruling out potential confounders. Those who take regular exercise might also (on average) get more sun, eat healthier foods or they might simply believe more strongly that their depression will go away. These other factors, rather than exercise, might cause their speedier recovery.
Different ailments and studies are at risk from different confounders, so the judgement of whether plausible confounders have been ruled out will depend on careful examination of each case. For ailments that are responsive to expectations (such as depression and pain) the confounding effects of expectations will have to be ruled out, which can be achieved by blinding the patients and caregivers. When the assessment of outcomes is prone to influence from observer bias (such as blood pressure), potential confounding by variable measurements has to be ruled out, perhaps by standardizing the measurement procedure and by blinding the investigators in charge of collecting the data and evaluating the outcomes.
Yet sometimes the strength of the association (the size of the effect) will be greater than the combined effect of plausible confounders. In these cases, although plausible confounders have not been ruled by the design of the study, the large observed effect has swamped the combined effects of any plausible confounders. For example, the observed effects of general anaesthesia are unlikely to be accountable by selection bias, placebo effects or reporting bias. Thus, the failure to test the effects of general anaesthetics in double‐blind, placebo controlled trials should not count against our beliefs that they cause reversible loss of consciousness.
Since one should compare the strength of association (size of effect) with the potential degree of bias, we have combined these into a single comparative guideline to emphasize this intrinsic comparison: is plausible confounding less than the size of effect?
A note of caution about strong relative effects (but small absolute effects) must be issued. Although ‘weak’ causes may be as real as ‘strong’ causes, it takes fewer (or ‘weaker’) confounders to account for a small absolute effect than for a large absolute effect. We therefore must be more careful when inferring from a strong relative (but small absolute) effect that an association is causal. At the same time, in many cases strong relative effects can provide strong support for the causal hypothesis. For instance, although the increased risk for lung cancer in smokers Bradford Hill cited was extremely low (0.07 per 1000 for non‐smokers, 0.57 for smokers), the death rate for lung cancer in cigarette smokers was over 9 times the rate for non‐smokers and thus provided good evidence for causation. 22
Our omission of the ‘experiment’ guideline should not be interpreted as a sign that any observational study will do. Observational studies must demonstrate larger effects than randomized trials since they are at risk from selection bias (because the allocation to treatment groups is neither randomized nor concealed) and performance bias (because the participants and caregivers are not blinded). Whether the effect size in a particular observational study is sufficiently large to rule out the combined effects of selection and performance bias will vary from case to case. If investigators conducting an observational study have been vigilant in attempts to reduce selection bias (through careful selection of the control groups and post hoc adjustments), and the outcome is objective, the observational study might not have to demonstrate a dramatic effect in order to support causation. 25, 26, 27 In most other cases, however, the effect in an observational study will have to be dramatic in order to be confident that plausible confounders have been ruled out. 5
In fact, our guideline can be more stringent than current EBM standards of evidence. According to hierarchies of evidence, RCTs with a low risk of bias often provide sufficient evidence to support causation. We require that, in addition to being at low risk, the effect size outweighs the combined effects of any residual bias. For example, although most systematic reviews of high quality RCTs of SSRIs suggest that these drugs enjoy a statistically significant benefit over ‘placebo’, 28, 29 the absolute benefit is modest – a recent study suggests it is 6% (2–9%). 30 Yet one often overlooked source of confounding in these studies is the identifiable side‐effects of the drug. If patients identify the drugs because of the side‐effects (and independently of their effects on depression), then their expectations regarding recovery might be higher than if they knew they were taking a ‘mere’ placebo. To rule out the possible confounding effect of expectations, ‘active placebos’, which imitate the side‐effects of SSRIs need to be employed. A systematic review of antidepressants versus ‘active’ placebos found that the drug less placebo difference was substantially reduced. 31 Besides confounding expectations, systematic reviews of SSRIs (like most systematic reviews) are likely to be confounded to some degree by publication bias, 32, 33 funding source bias 34 and data mining in the original studies. 35 A careful calculation of the combined effects of these plausible confounders must be made before claiming that the systematic reviews of SSRIs support the claim that the drugs cause the reduction in depressive symptoms. Such calculations have not (to our knowledge) been made, so this guideline, unlike current hierarchies, does not necessarily support the existence of (non‐placebo) effects of SSRIs.
Appropriate temporal and spatial proximity (encompassing and extending Bradford Hill's ‘Temporality’)
‘Does a particular diet lead to disease or do the early stages of the disease lead to particular dietetic habits?’ 22 The temporal part of this guideline is necessary: causes precede their effects and is therefore a true criterion. However, we should also ask: is the time interval between cause and effect consistent with the supposed mechanism? In general, the shorter the temporal and spatial interval, the less room for confounders (especially spontaneous remission) to interfere. It is equally important, for the time interval between administration of the treatment and cure to agree with the supposed mechanism of the treatment.
In some cases the spatial proximity between the site of administration and the outcome (see the oral ulceration example below) may support causality – for example, thrombophlebitis at the site of injection of a cytotoxic drug. Again, the outcome need not be close to where the intervention was administered in order for the relationship to be causal, but spatial proximity generally leaves less room for confounders to interfere.
Dose responsiveness (Bradford Hill's ‘Biological gradient’)
Does the outcome change when the intensity of the intervention is altered (at least if the purported mechanism predicts such a relationship)? While the presence of a dose‐response relationship does not always support causality (this guideline will not be applicable for ‘all or none’ causes), its absence when expected would lead us to doubt causality. Strongest ‘dose‐response’ evidence comes when the process is reversible. For example, the risk of lung cancer is increased in smokers but is also reduced by a half in those who stop smoking at the age of 50 years and almost completely abolished in those who stop at the age of 30. 36
Mechanistic evidence
Direct evidence does not always tell us how the intervention caused the outcome and this makes the result difficult to generalize. 37 What happens in between the intervention and the outcome is, as far as this category is concerned, a ‘black box’ (Figure 1). For example, Doll and Hill's famous study of the relation between the number of cigarettes smoked and the incidence of lung cancer 38 did not refer in any way to what happens between inhalation of cigarette smoke and the development of tumours in the lung. This brings us to the second category of guidelines.
Direct evidence of probabilistic dependence of outcome on intervention +
evidence for the causal process*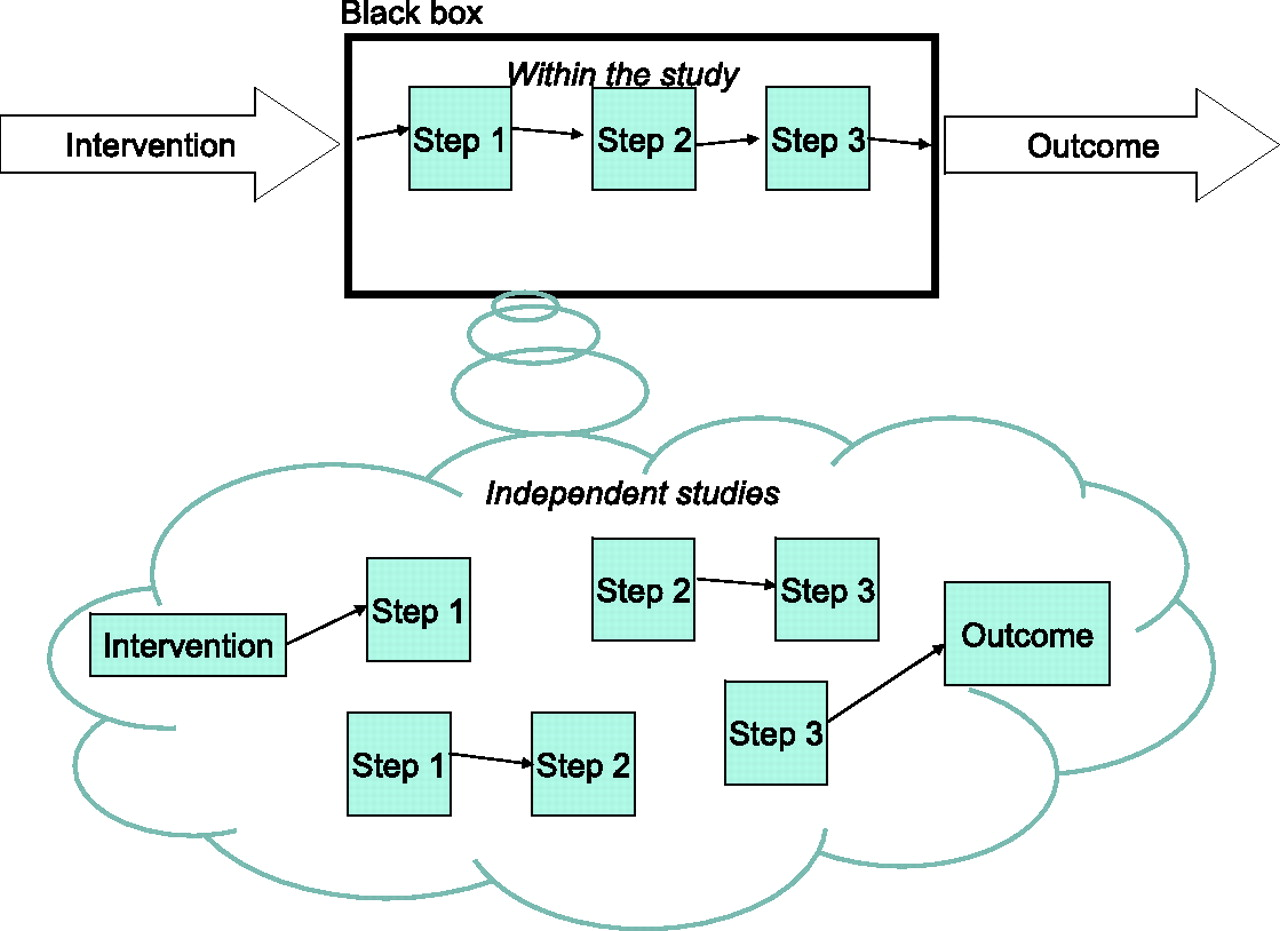
Although we believe that mechanistic evidence can provide evidential support for a causal hypothesis, two warnings are in order. Firstly, there is a difference between merely positing a mechanism (one can find a theory to explain almost anything) and providing sound evidence that there is a causal chain linking the intervention and the outcome. Secondly, appeal to mechanistic evidence has often justified the widespread use of treatments that turned out to be harmful. 40, 41, 42, 43, 44, 45, 46 Likewise, the absence of a plausible mechanism has often been used as a justification to ignore useful therapies such as antisepsis 47 and peptic ulceration. 48 With this in mind, although we believe that mechanistic evidence cannot be ignored, we acknowledge that mechanistic evidence should always play a subsidiary confirmatory role vis-à-vis direct evidence.
Plausible mechanism
Is there evidence supporting the causal chain linking the intervention and the outcome? For example, trials testing the effect of ACE inhibitors on reduction in stroke mortality might include evidence that ACE inhibitors reduce blood pressure, that reduced blood pressure reduces the risk of stroke, and that the reduced incidence of stroke reduces mortality. Of course, each ‘step’ in the causal process is a new ‘black box’. For example, the link between ACE inhibitors and blood pressure can be further decomposed into a series of steps, until (in a reductionist model) we bottom out at the molecular level. Bradford Hill, no doubt as an oversight, implied that plausibility was limited to ‘biological plausibility’. Mechanisms of action can also be mechanical (as in the Mother's Kiss example below) or chemical (as in the oral ulceration example below).
We can envisage three ‘levels’ of evidential support from mechanistic evidence. Firstly, the direct study can also include studies of the causal links between the intervention and the outcome (Figure 1, top half). A second level of mechanistic evidence is when the purported mechanism of action has been demonstrated in other, independent studies (Figure 1, bottom half). For example, separate studies could establish a probable link between ACE inhibition and lower blood pressure. Obviously, having evidence for a part of the mechanism is not as strong as evidence for all the links in the causal chain.
The second level of mechanistic evidence is closest to Bradford Hill's ‘Coherence’, and we have kept this guideline separate.
Coherence
Does the causal hypothesis cohere with what is currently known, or is it contradicted by current knowledge? This is best explained by what happens when the evidence does not cohere. For example, the causal process by which a homeopathic remedy is purportedly effective (other than by ‘placebo’ effects) is not currently explicable by mainstream science. Given the numerous examples where treatments that seemed to cohere with current science that turned out to be harmful, 40, 41, 42, 43, 44, 45, 46 and where treatments that seemed not to cohere with current science that turned out to be helpful, 47, 48 this guideline must be applied with care.
Parallel evidence
There are rarely cases where there is only a single piece of evidence for a causal claim. When assessing whether an association is causal it is obviously necessary to consider all the relevant studies – this is the powerful idea underlying the importance of systematic reviews.
Replicability (Bradford Hill's ‘Consistency’)
A study can be replicated, which means that the same intervention is tested on a similar population, using the same outcome measure. In order to count as a replication, all the elements of the study must be kept constant as far as possible. Replicability is a central tenet of scientific method: if the experiment can be repeated and provides the same results, the chances that the original results arose due to confounding is reduced. If an experiment is not replicable, either something is wrong with the attempt to replicate it or the initial experiment must be questioned.
Similarity (of the study to other studies)
No two studies are absolutely identical, so similarities form a spectrum ( Types of similarities (the axis of ‘similarity of circumstances’ is
omitted for simplicity)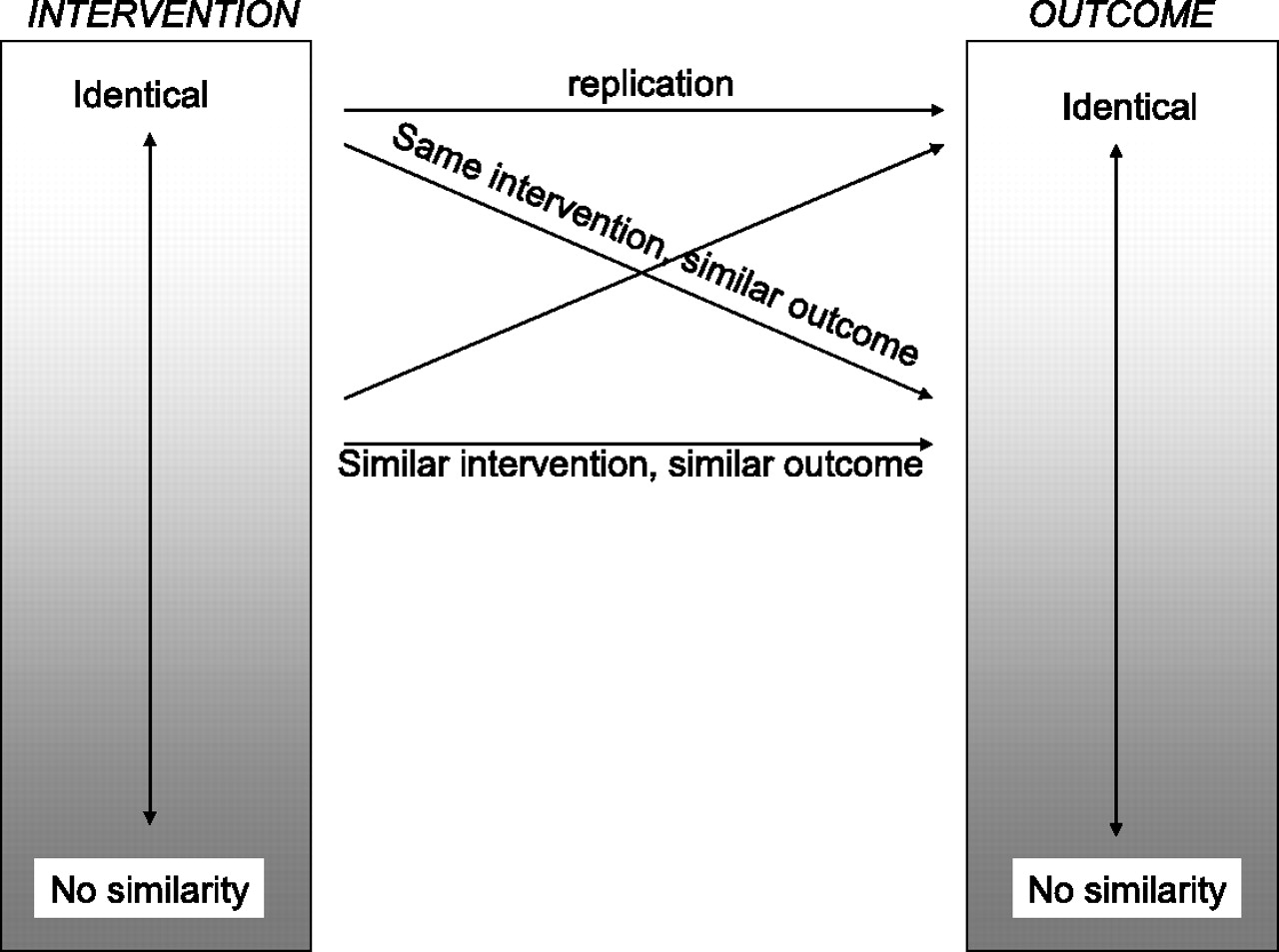
Omitted guidelines
Besides experiment, which was absorbed in our first revised guideline, we also omitted specificity. Diseases usually have multiple causes and multiple effects, while most interventions also have multiple effects. In fact, Bradford Hill did not support this guideline with adequate examples, and in his description of multiple regression he admits that most diseases have multiple causes and that most causes have multiple effects. 22 For example, the fact that smoking increases the risk of lung cancer in no way repudiates evidence that smoking causes other diseases. Similarly, the fact that Prozac might have a positive effect on depression does not reduce the force of the claim that it also cures premature ejaculation.
Tests of whether the Revised Bradford Hill guidelines deliver the verdict of strong evidence for causation, even if RCTs have not been conducted
A strict application of the EBM evidence hierarchy would deliver the verdict that the following treatments are supported by relatively poor evidence since they have not been tested in randomized trials. After describing the examples, we shall evaluate whether the Revised Bradford Hill guidelines deliver a more reasonable verdict.
The Mother's Kiss
Glasziou et al.
5
cite the following example:
A child presented with a plastic bead lodged high in one nostril. The
doctor asked for forceps, but the nurse suggested trying the mother's kiss
technique – occluding the unblocked nostril while the mother blows into the
child's mouth. The bead was thus easily dislodged and retrieved.
5
Most would agree that a single case (or at most a series of a few cases) would suffice to support claims that the mother's kiss caused the bead to dislodge.
Oral ulceration due to topical aspirin
Aronson and Hauben
49
have described several categories of adverse events related to drug
administration that seem to require little more than anecdotal evidence to provide
sufficiently strong evidence that the events are caused by adverse drug reactions.
One of the categories is ‘specific anatomical location or pattern of injury’, in
which:
… the location or pattern of injury is sufficiently specific to
attribute the effect to the drug without the need for implicit judgment or
formal investigation. The mechanism of injury can be related to
physicochemical or pharmacological properties of the drug. Examples include
extravasation reactions to cytostatic drugs and oral ulceration due to
topical aspirin.
49
Here, anecdotal observations provide strong evidence that a particular drug caused an adverse event.
Applying the Revised Bradford Hill guidelines
Conclusions: suggesting ways to revise current hierarchies of evidence
The original Bradford Hill Guidelines can be simplified (some of the guidelines can be
omitted while others can be combined or modified) and organized into three categories:
direct, mechanistic and parallel
evidence. In their revised form they suggest two ways that can inform revisions to
current hierarchies of evidence. Firstly, it is more important for ‘direct’ evidence to
demonstrate that the effect size is greater than the combined influence of plausible
confounders, than it is for the study to be experimental. This view is compatible with
the spirit of EBM hierarchies: the motivation for placing RCTs at the pinnacle of
evidence hierarchies is that they generally rule out more confounders than other study
types. If an observational study reveals an effect large enough to swamp the effects of
any additional confounding then other study designs must be regarded as on a par with
RCTs. Likewise, RCTs must demonstrate effect sizes sufficiently large to rule out the
combined effect of any inevitable bias. Secondly, the revised guidelines illustrate how
different types of evidence can complement one another How different types of evidence support the causal hypothesis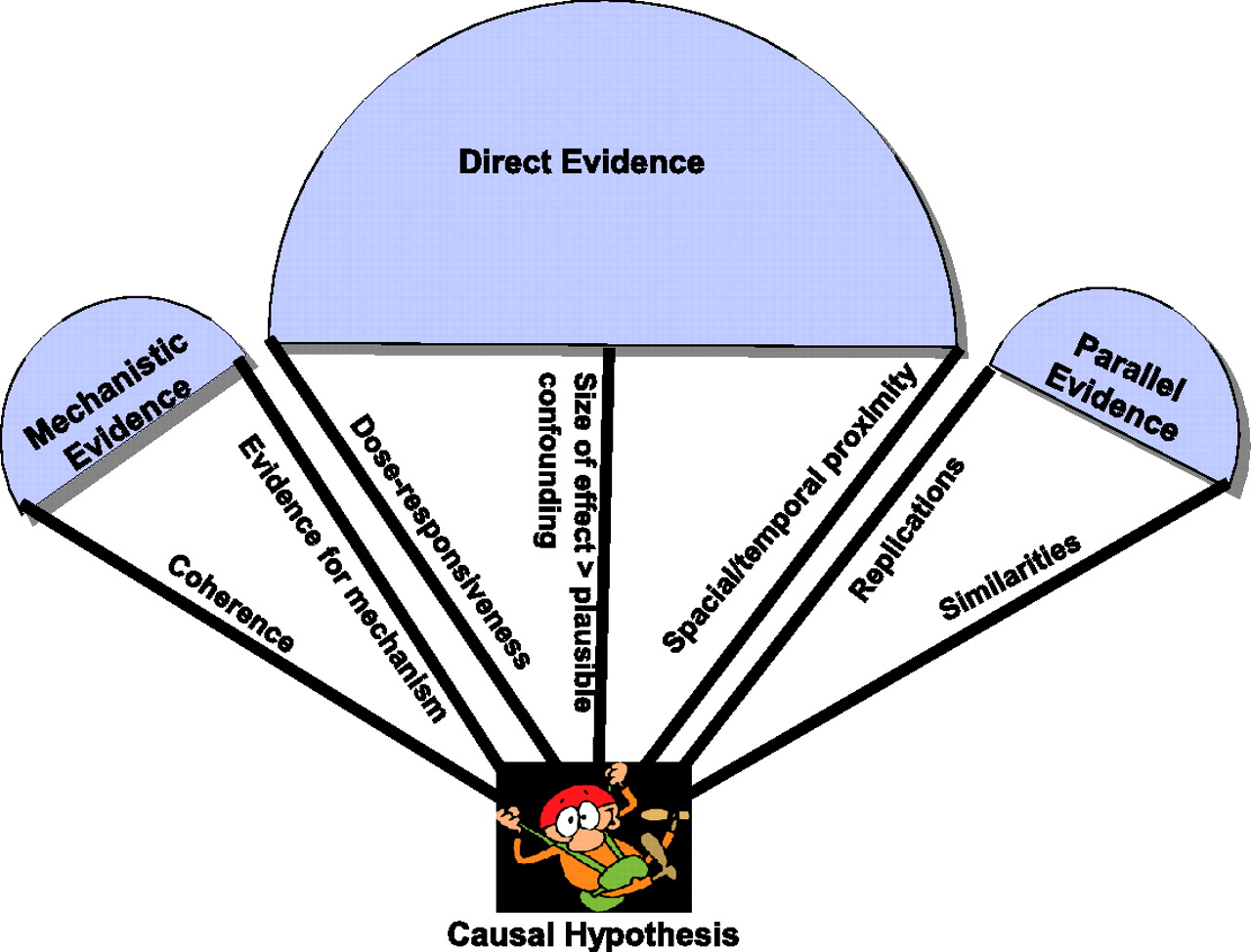
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
We are grateful to Nancy Cartwright for providing useful insights during conversations with the authors. Members of the GRADE working group, especially Roman Jaeschke and Joseph Watine, provided useful feedback. Murray Enking read an earlier draft and suggested the example of folic acid to prevent neural tube defects