
Abstract
Introduction
Eosinophilic oesophagitis is a modern diagnosis, emerging as an important clinical condition, of which, generalists should be aware (and specialists should be wary).
DECLARATIONS
None declared
None
The patient consented to publication
NB
NB wrote the paper, ML critiqued the paper and YC provided the histological report and images
Case report
A 36-year-old Caucasian woman was admitted to hospital after she had eaten a chicken dish and felt that food had stuck in the lower part of her gullet. On further questioning, she mentioned that she had experienced transient dysphagia in the past, including an episode after taking some tablets, which eventually resolved spontaneously. She had no significant past medical history and took no regular medication. Clinical examination, haematological and biochemical parameters were within normal range. An upper gastrointestinal endoscopy was arranged and confirmed the presence of a piece of chicken in the lower oesophagus causing a food bolus obstruction (Figure 1).

Food bolus in oesophagus
The food matter was partially broken up with endoscopic biopsy forceps and then the bolus was gently delivered into the stomach using the ‘push’ technique, which is a safe method for oesophageal bolus removal. 1 The endoscopic procedure was uncomplicated, revealing no oesophageal stricture and a normal stomach and duodenum. There was no endoscopic evidence of reflux oesophagitis.
On withdrawal of the endoscope, macroscopic appearances of eosinophilic oesophagitis (EO) were seen in the mid oesophagus, which include circular rings and linear furrows (Figure 2).

Mid-oesophagus demonstrating circular rings and linear furrows
In light of the compatible symptoms, mid-oesophageal biopsies were taken to examine for microscopic evidence of EO.
She complained of chest pain soon after the procedure and this progressed over a number of hours. She became unwell and was noted to have severe epigastric pain and evidence of surgical emphysema around the neck. Chest X-ray and CT scan confirmed evidence of pneumomediastinum secondary to oesophageal perforation. She was transferred to a tertiary unit for mediastinoscopy and repair of the oesophageal perforation which was successful, culminating in the patient's discharge home.
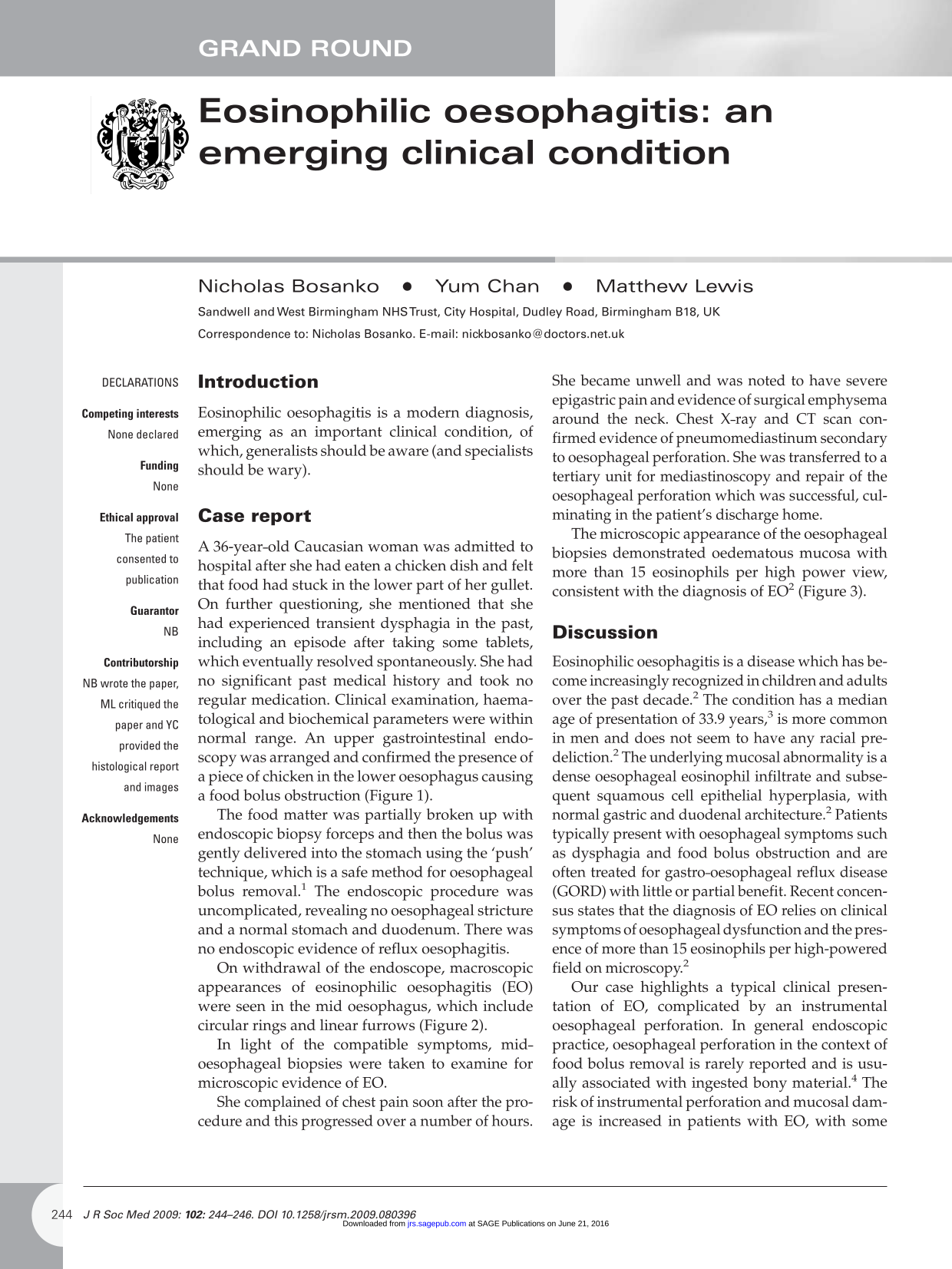
The microscopic appearance of the oesophageal biopsies demonstrated oedematous mucosa with more than 15 eosinophils per high power view, consistent with the diagnosis of EO 2 (Figure 3).
Oesophageal biopsy after haematoxylin and eosin stain showing eosinophils (arrows and circle)
Discussion
Eosinophilic oesophagitis is a disease which has become increasingly recognized in children and adults over the past decade. 2 The condition has a median age of presentation of 33.9 years, 3 is more common in men and does not seem to have any racial pre-deliction. 2 The underlying mucosal abnormality is a dense oesophageal eosinophil infiltrate and subsequent squamous cell epithelial hyperplasia, with normal gastric and duodenal architecture. 2 Patients typically present with oesophageal symptoms such as dysphagia and food bolus obstruction and are often treated for gastro-oesophageal reflux disease (CORD) with little or partial benefit. Recent concensus states that the diagnosis of EO relies on clinical symptoms of oesophageal dysfunction and the presence of more than 15 eosinophils per high-powered field on microscopy. 2
Our case highlights a typical clinical presentation of EO, complicated by an instrumental oesophageal perforation. In general endoscopic practice, oesophageal perforation in the context of food bolus removal is rarely reported and is usually associated with ingested bony material.” The risk of instrumental perforation and mucosal damage is increased in patients with EO, with some patients suffering oesophageal perforation following the simple passage of the endoscope or after routine biopsies. 5 In one series, 31% of EO patients suffered endoscopic complications of oesophageal laceration and rupture (8.3%). 3 Endoscopic evidence of mucosal fragility or oedema has been identified in 59% of patients with EO. 6
There is often overlap between the symptoms and clinical findings related to EO and GORD. In order to secure the diagnosis, it is recommended that patients fulfilling the symptomatic and histological criteria are also demonstrated to have lack of responsiveness to high-dose proton pump inhibition and normal pH monitoring of the distal oesophagus. 2 It is worth noting that oesophageal manometric abnormalities are common, with up to 60.6% of patients with EO displaying evidence of spastic or hypocontractile oesophagus. 7
The prevalence of EO has been found to be as high as 43 per 100,000 in one paediatric series. 8 There is also evidence that the prevalence is rising from 2 per 100,000 to 30 per 100,000 in one adult study over 18 years. 8 It is likely that this is an underestimate as many people with low grade symptoms may not have presented to their doctor, nor been referred for endoscopic and histological evaluation. In studies which have evaluated the presence of EO in patients with who present with food bolus obstruction, around 50% of patients have been found to have the condition. 8
Allergic responses have been strongly implicated in the aetiology of EO based on several lines of evidence. EO is frequently associated with the co-existence of atopic conditions 2 and, as would be expected, there is usually acute resolution of eosinophilic inflammation with the use of systemic corticosteroids. Swallowed corticosteroid, delivered orally via an inhaler device, has also been demonstrated to improve symptoms, but the benefits may be limited by the development of candidiasis. 2 Positive symptomatic benefit has also been demonstrated by the use of leukotrine receptor antagonists, dietary restrictions 9 and immunomodulatory therapy 10
Conclusion
We report a significant endoscopic complication occurring in a patient with evidence of an underlying oesophageal inflammatory disorder which is becoming more widely recognized. EO considered as a possible diagnosis in children and adults with GORD symptoms which are poorly responsive to acid suppression and in patients with intermittent dysphagia or food bolus obstructions. There is often a delay in diagnosis, estimated at mean of 54 months 2 and patients with compatible symptoms should be referred for endoscopic evaluation and oesophageal biopsies, even if the macroscopic appearance of the oesophagus is normal. We wish to highlight the fact that oesophageal fragility in EO leads to an increased risk of perforation following relatively minor instrumentation, hence a need for endoscopists to be cautious. There has been a huge rise in the numbers of published articles regarding EO in recent times. A PubMed should be search for ‘eosinophilic oesophagitis’ revealed 403 references, of which 310 have been published in the last five years. This suggests that our knowledge about the aetiology and treatment of this condition will continue to develop.
Footnotes
Acknowledgements
None