
Abstract

Introduction
In recent years there has been a convergence of approaches to the treatment of cardiovascular disease with combined cardiology, radiology and surgical multidisciplinary team (MDT) based management. This is particularly true with the advent of transcatheter (transfemoral and transapical) aortic valve replacement 1 as well as the new combined open and endovascular approaches to thoraco‐abdominal aneurysms, 2 including single stage combined coronary artery bypass grafting (CABG) and abdominal aortic endovascular aneurysm repair (EVAR). 3 However, there has also been a more longstanding, and commonly although not exclusively, staged hybrid approach in the form of combining percutaneous coronary intervention (PCI) with surgical coronary revascularization and surgical valve repair or replacement in appropriate patients. 4, 5, 6 As such, it is inevitable new operating enviroments have emerged in the form of so‐called ‘hybrid theatres’ allowing single stage, hybrid endovascular and open intervention for a range of morbidities in children and adults. 7, 8 This manuscript discusses briefly the design and function of a hybrid theatre, including its perceived advantages and disadvantages. By way of example we review our activity in this environment over the first year of opening. We discuss whether this resource is a nicety or necessity in adopting hybrid approaches.
Design and function of the hybrid theatre
As part of the development of a regional thoracic aortic aneurysm service a purpose‐built hybrid theatre was constructed (Philips) and opened in Liverpool in April 2007. A number of detailed descriptions of hybrid theatres exist 8, 9, 10 and we therefore restrict the discussion here to a brief overview. Broken down into its basic structural components, the hybrid theatre is simply an operating theatre with built‐in radiological screening capabilities. In truth, however, the hybrid theatre is more than simply the sum of its parts. The bespoke C‐arm image intensifier is built into the ceiling of the operating room and able to move both longitudinally and rotate around the axis of the patient (Figures 1a and b). As such, the theatre complex is designed with ample space, allowing for dedicated cardiopulmonary bypass equipment as well as the paraphernalia associated with general anaesthesia. Other equipment, including transoesophageal echocardiography, cell salvage, electrocautery and pacing, are easily accommodated. Multiple monitors allow easy access to data at all points around the table. High quality overhead lights allow for good visibility. Consistent with a normal catheter laboratory the theatre is designed with a control/viewing room with dedicated image processing, as well as catheter store room, surgical scrub room and anteroom. Lead aprons are available. Other devices such as contrast injector and defibrillator are stored in theatre. It is not only the close proximity of this multidisciplinary equipment which makes this a unique environment, but the fact that it engenders a collaborative approach to the management of complex disease.
Hybrid approaches to elective cardiovascular disease
The hybrid activity in the theatre is coordinated by two MDT meetings attended regularly by consultant representation from cardiology and radiology, as well as both vascular surgery and cardiac surgery, and intensive care medicine. The specialization of these two groups centres on endovascular approaches to thoraco‐abdominal aortic disease and transfemoral/transapical aortic valve replacement.
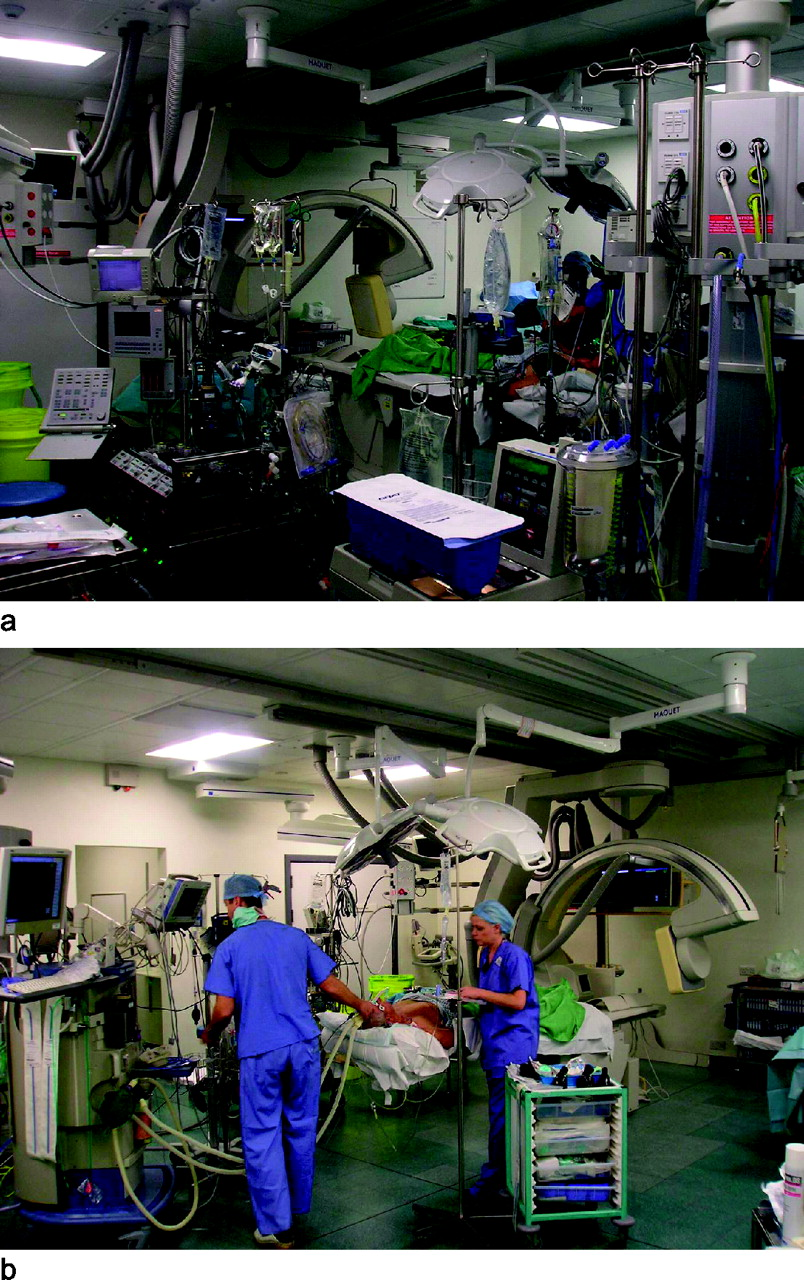
Hybrid theatre showing the theatre table, roof-mounted C‐arm, perfusion, anaesthetic and surgical equipment
Hybrid thoracic endovascular aneurysm repair (TEVAR)/open procedures
Surgical activity 2007–2008
CABG, coronary artery bypass surgery; EVAR, endovascular aneurysm repair; TEVAR, thoracic EVAR; AVR, aortic valve replacement; MVR, mitral valve replacement; TVR, tricuspid valve replacement; AF, atrial fibrillation; VATS, video‐assisted thoracic surgery
Transfemoral and transapical aortic valve replacement
A regular MDT comprising interventional cardiologists, cardiac surgeons and anaesthetists/intensivists discusses possible suitable patients for this approach. To date we have early experience with transfemoral and transpical aortic valve replacement and found the hybrid theatre exceptionally well suited for this activity.
Simultaneous CABG and EVAR
The hybrid theatre has provided a unique opportunity to treat a specific group of patients with combined coronary artery disease and abdominal aortic aneurysm. These are complex patients who normally require two significant staged interventions, the sequence of which exposes them to risk from the untreated morbidity. Coronary artery surgery in the presence of untreated abdominal aortic aneurysm exposes them to risk of rupture, while intervention on the aneurysm in the presence of untreated ischaemic heart disease exposes them to the risk of a perioperative myocardial infarction. Our approach to these patients has been to perform both procedures under a single general anaesthetic. Typically, we perform EVAR on the abdominal aortic aneurysm followed by surgical coronary artery bypassing either on or off pump. We believe this lowers the overall risk for the patient as well as reducing significantly their overall hospital stay and cost. 11
Routine elective cardiological and cardiovascular surgical activity
Medical activity summary 2007–2008
ICD, internal cardiac defibrillator
Emergency work
The advantages of the hybrid theatre are best seen in the setting of our emergency aortic practice. The treatment of Type B aortic dissection has been transformed by our access to this facility. While previously Type B dissections were mainly managed medically in peripheral hospitals, with occasional patients being transferred to our Cardiothoracic Centre for treatment of life‐ threatening complications, we now transfer nearly all patients on diagnosis. Our facility allows for earlier and better endovascular and open intervention on these maladies including fenestration, stenting and extra‐anatomical bypass surgery. The close relationship between cardiac surgeons, vascular surgeons and interventional radiologists allows for a multidisciplinary discussion and treatment of this previously under‐treated condition. In addition, leaking thoracic aneurysm in the elderly population, which previously were consigned to medical management, are often taken on for either endovascular or hybrid endovascular‐open solutions. This is particularly true in the treatment of aortic arch surgery where the calcified diseased arch may be stented with prior extra‐anatomical bypass to the neck vessels. The approach putatively reduces the risk of intervention in this elderly group.
Discussion
Hybrid theatres allow for not only routine surgical and medical interventions, but also combined catheter‐based interventions and open surgery under a single anaesthetic. In this discussion we address the issue of whether these hybrid interventions are beneficial and whether a hybrid theatre is a nicety or a necessity in performing these procedures.
Potential advantages of a hybrid theatre
Hybrid theatres have several perceived advantages including:
Space: The theatre is approximately twice the size of a
normal surgical theatre or catheter laboratory allowing for not only the
vast array of equipment and personnel but also the space required for
deployment of catheter devices, particularly the operating bed which
conventionally does not allow for the work space required to manage catheter
devices;
Bespoke C‐arm screening with on‐line 3D digital
reconstructions: The roof mounted C‐arm allows for convenient,
high quality imaging with online processing vastly superior to portable
systems commonly used in non‐hybrid environments;
Theatre table: The operating table is central to the
environment. As a surgical table it allows for routine surgery as well as
positioning in on‐pump and off‐pump coronary artery surgery. In addition, as
a screening table it allows for catheter‐based procedures;
Dedicated anaesthetic and perfusion capabilities: Dedicated
anaesthetic and perfusion equipment is a key logistical advantage being very
convenient negating the need to seek and transfer equipment as required;
Locality within surgical complex: The arrangement promotes
the multidisciplinary process with a common locality of equipment and
personnel. This allows for efficient use of staff and equipment;
Conversion: Even pure endovascular work requires facility
for conversion.
13
This is particularly true of thoraco‐abdominal stenting,
transfermoral/transapical AVR and combined CABG and EVAR. The facility to
rapidly convert to an open procedure without compromising the patient is
effectively dictated by ethics insomuch as a newly‐adopted procedure should
not expose the patient to any added risk and should be at least as
efficacious as the routine approach. This is easily achieved in the hybrid
environment.
There are also potentially large financial benefits of performing hybrid procedures, which would otherwise require two separate hospital admissions and longer overall hospital stay for patients. Following on from this one may expect higher patient satisfaction. The extent to which these benefits are a reality requires further clarification through the use of well‐conducted comparative studies. Although intuitive, there has been no formal financial analysis published to demonstrate the efficiency of the theatre to date.
Potential disadvantages of a hybrid
The main disadvantage of establishing a hybrid theatre is cost. However, an easy
business plan based on the future marketplace can be proposed. Any centre of
excellence will be expected to provide this range of services in the coming years.
Catheter‐based interventions, with or without hybrid open adjuncts, are the future of
cardiovascular treatments. These should be embraced in a multidisciplinary spirit by
both surgeons and physicians. More specific putative disadvantages might include:
Infection risk: The size of the hybrid theatre and the
nature of the interventions which require a higher number of personnel might
result in a theoretically higher infective risk although this has not been
seen in our outcomes and no data exist in the literature;
Prolonged general anaesthetic: Although general anaesthetic
times are long, there is an obvious balance of risks comparing several
anaesthetics with multiple procedures over a longer period of time. Again
there is a lack of specific data on this putative benefit in the literature.
An additional factor that must be considered is the radiation exposure
associated with prolonged procedures particularly when deploying branched
and fenestrated grafts.
The Liverpool‐specific experience
We do not claim anything special about the physical aspects of the hybrid theatre in Liverpool, although we would like to suggest that our management of it has created a unique outcome. We have adopted a thoroughly collaborative approach embracing all specialties. By discussing hybrid activity in MDTs and ensuring multidisciplinary presence at all procedures we have adopted an attitude of inclusivity. In this way we have avoided any territorial conflict between specialties. We believe patients have benefited from this open collaborative approach by increasing their options with truly innovative hybrid approaches to care. Previously many of these patients may have been denied any intervention.
The future
Hybrid theatres are becoming increasingly complex allowing increasingly complex hybrid approaches. Some centres have introduced robotic technology allowing inclusion of minimally invasive open procedures. 4 In addition, one centre has introduced magnetic resonance imaging into the hybrid environment for complex neurosurgical intervention. 14 Inevitably, endovascular approaches to the mitral valve 15 and congenital heart disease 16 will further the utility of these environments. Single stage combined CABG and carotid artery stenting is another area of interest as well as complex branched and fenestrated graft stenting.
Nicety or necessity?
In order to answer this question we define necessity in the context of a hybrid theatre as a particular procedure which cannot physically be done except in this environment. Nicety we suggest the procedure could be done out of the hybrid environment but with inconvenience and possibly risk. In all honesty, there are few, if any, of these procedures which could not ultimately be performed in a normal theatre or catheter laboratory, albeit with a great deal of extra time, inconvenience, effort and perhaps risk to the patient. Certainly the hybrid theatre allows hybrid solutions to be executed conveniently, safely and timely making it a practicality issue. However, we believe more than that, arranged as we have, it is not the physical environment which is the key but the interdisciplinary collaborative aspects it engenders which are the true advantages of the hybrid theatre. We believe that in practical terms the hybrid theatre is a nicety, however as a focus engendering a spirit of collaboration with novel solutions to complex disease, it represents a necessity. It may also be argued that on the basis of patient safety, this suite is a necessity in performing complex hybrid procedures. As stated, the outcome is more than the sum of its parts. A proviso must always be that the management process adopted should be best care for the patient rather than the application of technology for its sake.
Conclusions
The improved collaboration between healthcare professionals, which is what the hybrid theatre represents, is only likely to be of benefit to patients. Not only through the perceived advantages outlined above but also through the sharing of knowledge and clinical expertise that close collaborative partnerships entail. Hybrid theatres are a necessity in engendering this approach in a convenient way for the clinicians and in a safe way for the patients. The hybrid theatre represents a new standard of care.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
In the spirit of the content of the paper, we acknowledge the contributions of many other personnel from a multitude ofspecialties. But for a journal limit on authorship, we would include them all