
Abstract
Summary
Objective
To assess the contemporary caseload of NHS plastic surgeons.
Design
Descriptive study.
Setting
Scotland.
Methods
Analysis of routinely collected NHS hospital activity data relating to the financial year 2005–2006.
Main outcome measures
Number of inpatient/day-case episodes and bed-days by principal diagnosis and main operative procedure.
Results
During the study period, 12,844 inpatient and 9439 day-case episodes were recorded in 19,166 patients, accounting for 36,300 bed-days. There were more female patients, especially among middle-age groups. Socioeconomic deprivation was more common than expected (P < 0.0001), especially among younger age groups and male patients. In terms of episodes, the most common categories of diagnosis were neoplasms (28.4%) and injuries, including burns (22.4%). However, injuries accounted for a higher proportion of bed-days (37.3%) than neoplasms (23.8%). Only approximately half of all surgical procedures were assigned to the skin chapter of the OPCS-4 classification.
Conclusions
Despite some limitations, this study provides an insight into the current caseload of NHS plastic surgeons working in Scotland. The data suggest that cosmetic surgery for purely aesthetic reasons represents a relatively small part of NHS plastic surgery activity in Scotland, and that the majority of caseload is in reconstructive plastic surgery.
Introduction
In January 2007, the BMJ published a personal view entitled ‘We don't need another 400 plastic surgeons’. 1 Perhaps stung by the suggestion that plastic surgery trainees might all simply want to be cosmetic surgeons, the article provoked 72 rapid responses within less than three months, mainly from the plastic surgery community. 2 Many correspondents expressed their frustration about the public image of plastic surgeons, based on misconceptions of their role, although this is by no means a new phenomenon. 3, 4, 5, 6 With notable exceptions, very few correspondents supported their arguments with data.
Age and sex distribution of inpatients and day-cases, 2005–2006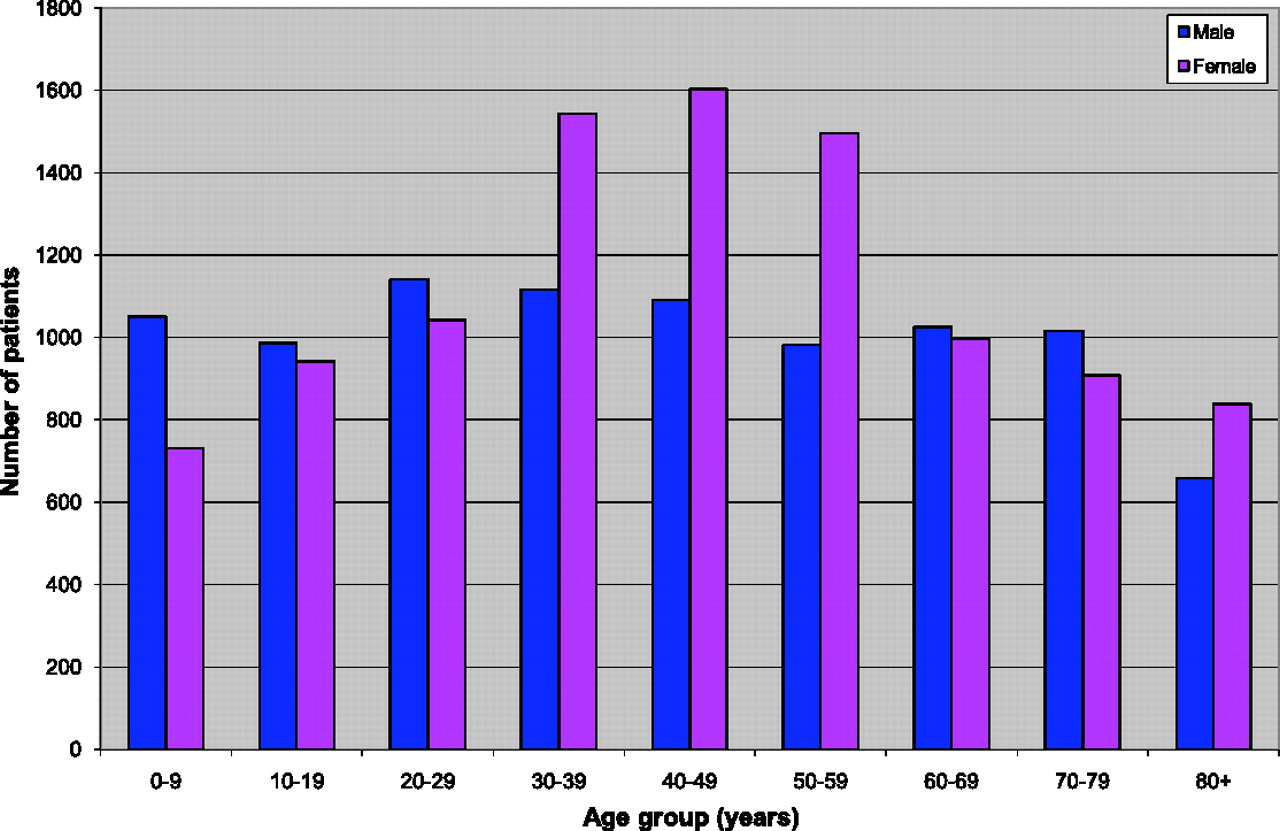
By analysing routinely collected NHS hospital activity data, the aim of the present study was to provide information about the contemporary caseload of NHS plastic surgeons in one part of the UK.
Methods
Anonymized inpatient and day‐case hospital episode data for the plastic surgery
specialty and the financial year April 2005–March 2006 were obtained from the
Information Services Division of NHS National Services Scotland. There are four main
plastic surgery units in Scotland. The data were analysed by principal diagnosis and
main operative procedure. Although essentially administrative data, re‐abstraction
exercises have shown that the coding of the principal diagnosis and main operative
procedure are approximately 90% reliable at the level of three digit ICD-10
8
and OPCS-4
9
categories.
10
The impact of socioeconomic position was Plastic surgery inpatient and day-case episodes by main diagnostic category,
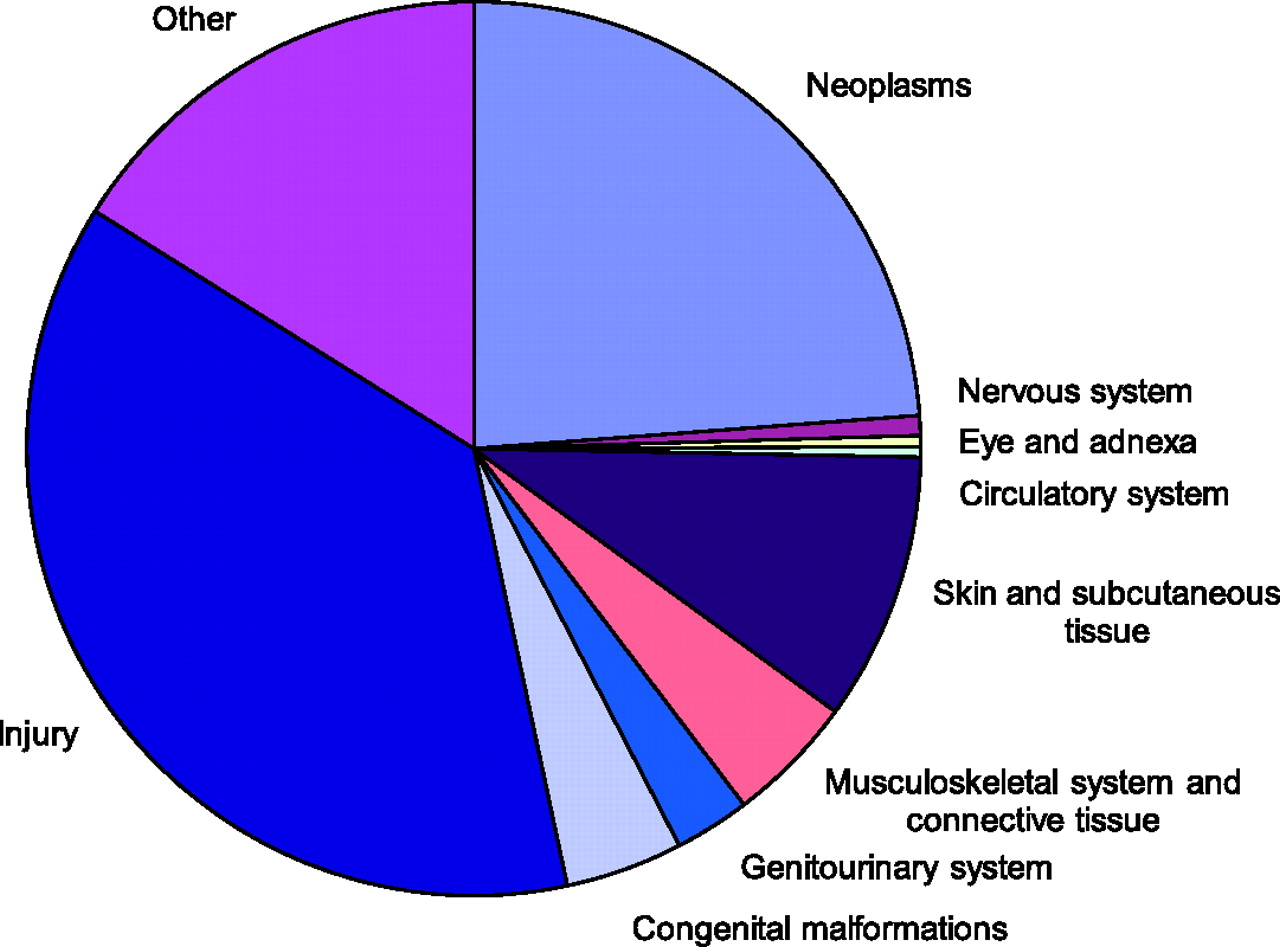
Scotland, financial year 2005–2006 Plastic surgery inpatient bed-days by main diagnostic category, Scotland,
financial year 2005–2006 Plastic surgery inpatient and day‐case episodes by principal diagnosis,
Scotland, financial year 2005–2006
*
Note that only selected subcategories of the main diagnostic categories
(italics) are shown. Only the sums of the main diagnostic categories
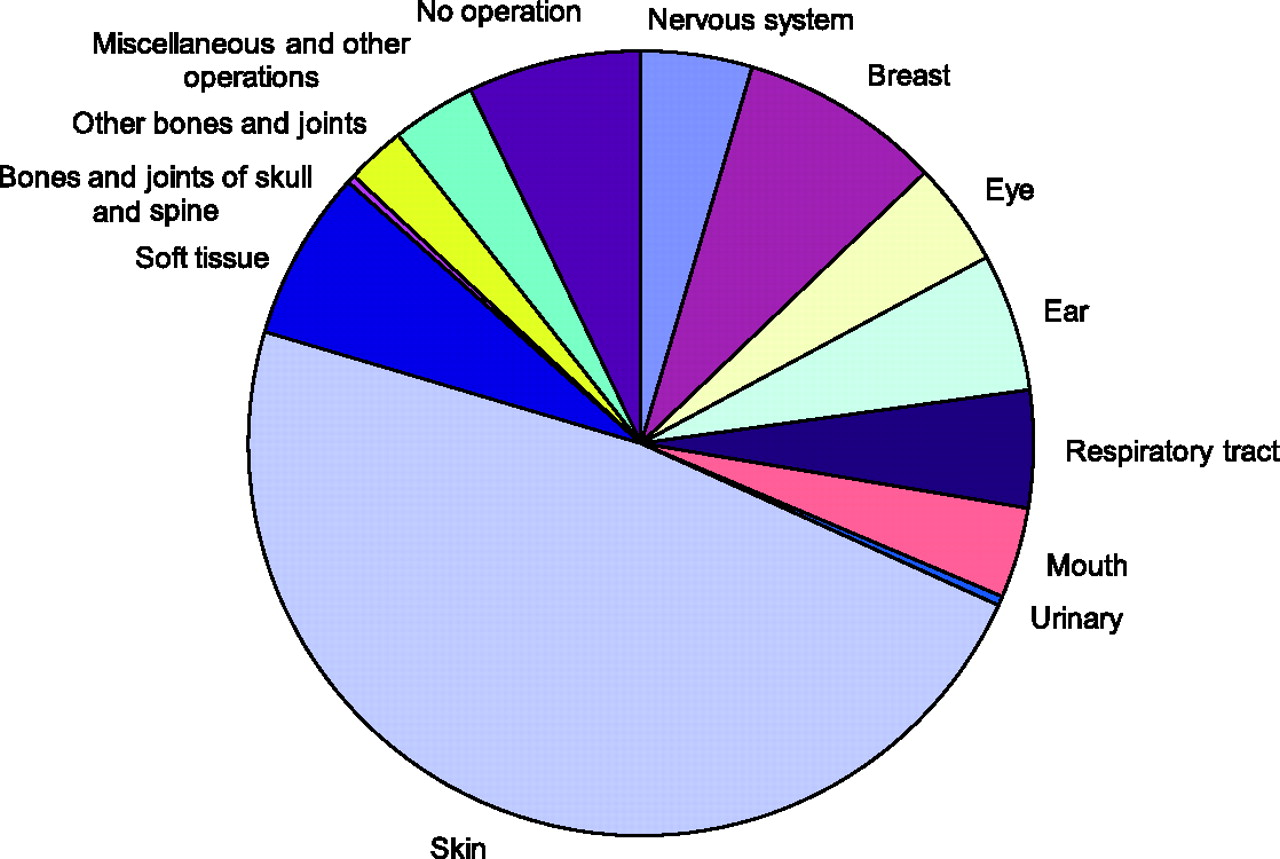
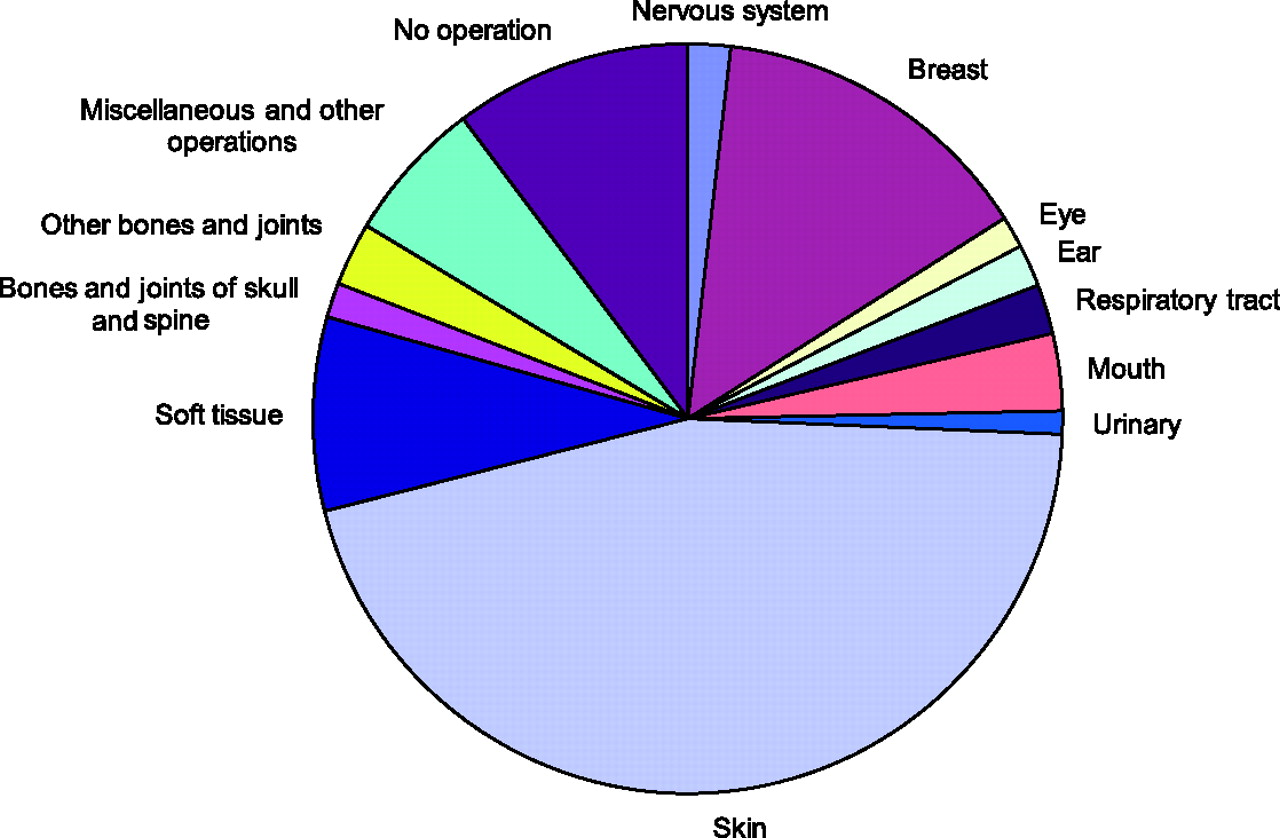
correspond to the column totals Plastic surgery inpatient and day-case episodes by main operation category,
Scotland, financial year 2005–2006 Plastic surgery inpatient bed-days by main operation category, Scotland,
financial year 2005–2006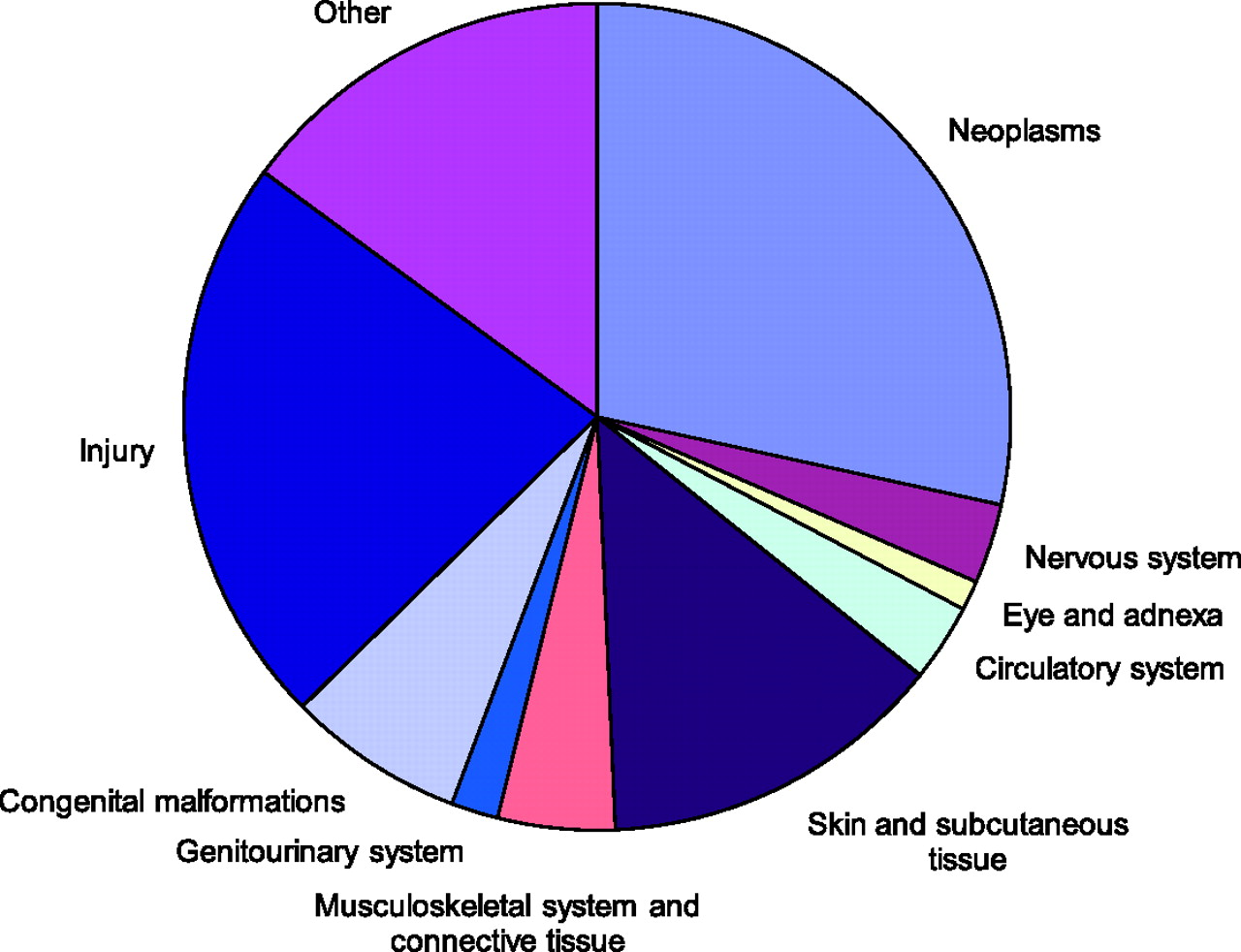
Results
During the financial year April 2005–March 2006, 12,844 inpatient and 9439 day‐case episodes were recorded in 19,166 patients, accounting for 36,300 bed-days. Overall, there were more female (10,098) than male (9068) patients, especially among the middle‐age groups, although men predominated at the ages under 30 and 60–79 years (Figure 1). A higher than expected percentage of patients (25.3%) were assigned to the most deprived quintile of the Scottish Index of Multiple Deprivation based on their postcodes of residence (Chi‐squared = 373.2, P < 0.0001). Socioeconomic deprivation was more commonly observed among younger age groups and male patients.
The distribution of inpatient or day‐case episodes and bed‐days by main category of principal diagnosis is shown in Figures 2a and 2b, and in Table 1 with selected, more specific diagnoses listed under each main category. In terms of episodes, the most common categories of diagnosis recorded were ‘Neoplasms’ (28.4%) and ‘Injury, poisoning and certain other consequences of external causes’ (22.4%). However, ‘Injury, poisoning and certain other consequences of external causes’ accounted for a higher proportion of bed‐days (37.3%) than ‘Neoplasms’ (23.8%).
Plastic surgery inpatient and day‐case episodes by main operation, Scotland, financial year 2005–2006 *
Note that only selected subcategories of the main operation categories (italics) are shown. Only the sums of the main operation categories correspond to the column totals
Discussion
We have used national data, collected routinely, to describe the caseload of NHS plastic surgeons in Scotland. It has been observed that case numbers alone may give a totally misleading impression of the amount and type of work carried out by plastic surgeons. 12 However, for the sake of simplicity, we chose to analyse only the principal diagnosis and the main operative procedure of inpatient or day‐case episodes. Inevitably, this underestimates the complexity of the workload because many patients have multiple diagnoses and multiple procedures performed. Furthermore, we did not analyse outpatient data because these do not record all return visits, they do not usually record diagnosis, and the recording of operative procedures is believed to be incomplete. According to existing published statistics, 26,480 new plastic surgery outpatients were seen during the financial year April 2005–March 2006. 13
Despite the limitations of our analysis, we believe that our results provide a reasonable insight into the current pattern of work of NHS consultant plastic surgeons in Scotland who, according to national manpower census statistics, numbered 26 at 30 September 2005, approximately halfway through our study period. 13 It is possible to classify many of the diagnoses and procedures listed in Tables 1 and 2 according to whether they relate primarily to reconstructive surgery or to aesthetic surgery. Based on this, the data suggest that the majority of caseload is in reconstructive plastic surgery, and that cosmetic surgery for purely aesthetic reasons represents a relatively small part of NHS plastic surgery activity in Scotland. Even for the latter cases, clinical coders may not have been aware of other factors underpinning the decision to operate, such as psychological morbidity. In future, the advent of clinical information systems may permit a more clinically meaningful classification and analysis of plastic surgery activity.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
The authors are grateful to Tracey Rapson of the Information Services Division, NHS National Services Scotland for supplying the data for this study