
Abstract
Introduction
Interventional radiology is defined by the Society of Interventional Radiology as ‘the delivery of minimally invasive, targeted treatments, performed using imaging for guidance’. Although the principles of angiography for diagnosis have existed since the 1920s, and today remain a well-established modality for the diagnosis of many common conditions, it was not until the 1960s that the American Charles Dotter, and other pioneers, extended these techniques from diagnosis to treatment. 1 Their foresight, together with ever-increasing technological capability, allowed the use of transluminal angioplasty for the treatment of peripheral vascular disease and led Dotter to say, in 1964, that ‘it should be evident that the vascular catheter can be more than a tool for passive means for diagnostic observations: used with imagination it can become an important surgical instrument’.2,3 Thus, interventional radiology as a specialty was born. Work on the cerebral vasculature began in the 1970s, largely for neurosurgical conditions. It is perhaps not surprising that the initial, and still best known, uses of interventional radiology were for the highly accessible vascular system, and for the type of non-vascular conditions that offered poor surgical access, such as in neurosurgery. More recently, interventional radiology techniques have been applied to head and neck cancer patients, initially with the use of detachable balloon occlusion in patients with laryngeal cancer and impending carotid artery rupture. From this, the range of applications of interventional radiology in the extra-cranial head and neck has continued to evolve and expand. These applications include line placement, foreign body removal, placement of feeding tubes (primary gastrostomy, gastrojejunostomy or jejunostomy tubes), and oesophageal or bronchial dilatation and stenting. The main focus of this review is on the vascular applications of interventional radiology in the head and neck, which can be divided into three main categories: management of acute haemorrhage (e.g. epistaxis, carotid blowout); management of vascular lesions (e.g. tumours, arterio-venous malformations); and venous sampling.
DECLARATIONS
None declared
None
Not applicable
SB
All authors contributed equally
Management of acute haemorrhage
Epistaxis
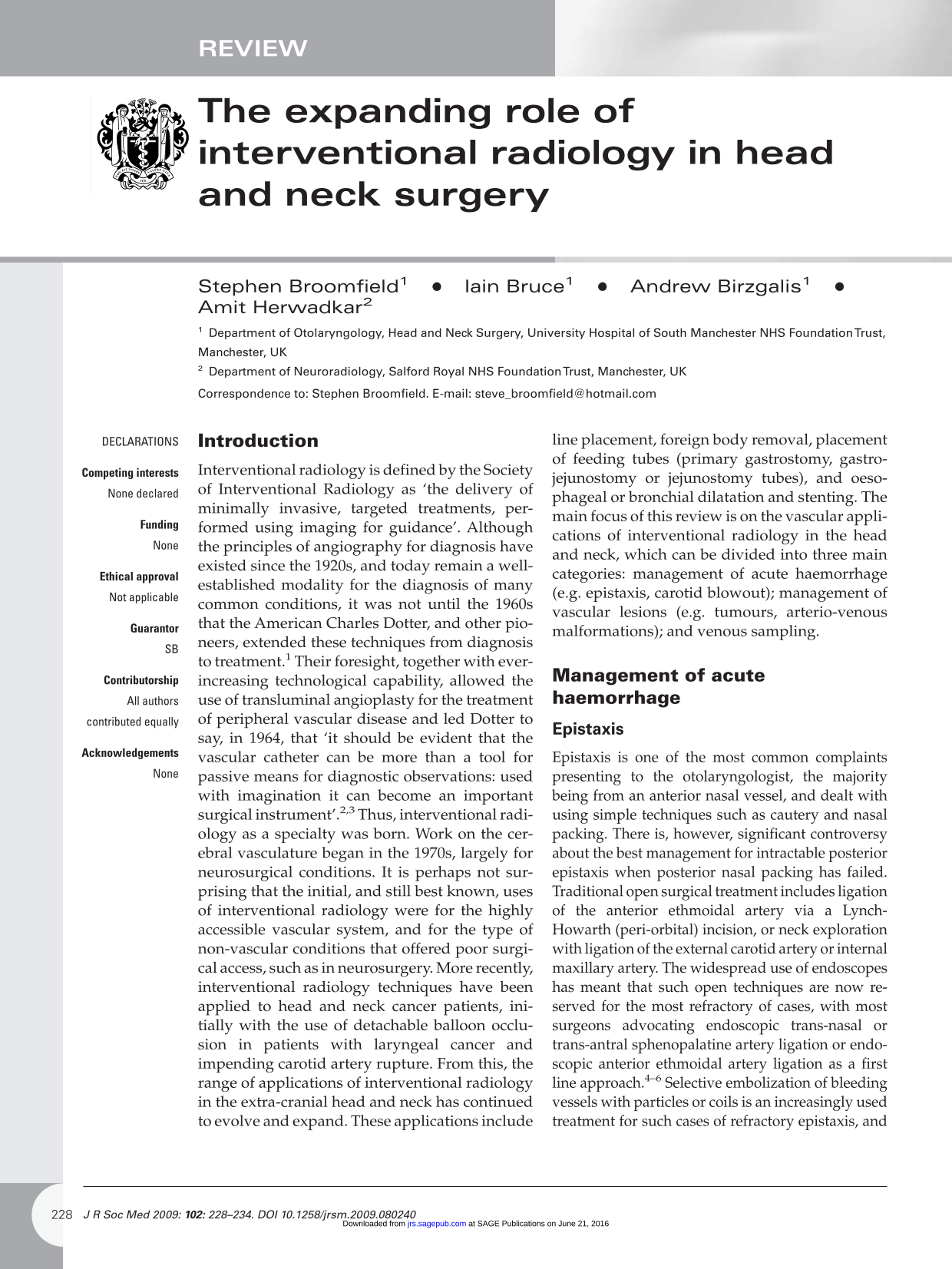
Epistaxis is one of the most common complaints presenting to the otolaryngologist, the majority being from an anterior nasal vessel, and dealt with using simple techniques such as cautery and nasal packing. There is, however, significant controversy about the best management for intractable posterior epistaxis when posterior nasal packing has failed. Traditional open surgical treatment includes ligation of the anterior ethmoidal artery via a Lynch-Howarth (peri-orbital) incision, or neck exploration with ligation of the external carotid artery or internal maxillary artery. The widespread use of endoscopes has meant that such open techniques are now reserved for the most refractory of cases, with most surgeons advocating endoscopic trans-nasal or trans-antral sphenopalatine artery ligation or endoscopic anterior ethmoidal artery ligation as a first line approach.4–6 Selective embolization of bleeding vessels with particles or coils is an increasingly used treatment for such cases of refractory epistaxis, and has been shown by many to be safe and effective7–12 Figure 1 shows how bleeding was managed using embolization in a patient with intractable epistaxis who was not considered fit for general anaesthesia.
(a) Digital subtraction angiogram showing nasal vasculature with bleeding point (black arrow) and catheter (white arrow); (b) after selective embolization there is no blood flow to the bleeding point (black arrow). Blood flow to the anterior part of the nose has been preserved (white arrow)
At present, there is little consensus as to which treatment modality is preferable or most cost effective, as both surgery and embolization carry similarly acceptable complication rates. Each patient is therefore managed on an individual basis, taking into account the experience of the surgeon, the fitness of the patient for general anaesthesia and the availability of interventional radiology services.
Carotid blowout
Carotid blowout can be defined as ‘bleeding from the carotid artery or its branches’. The modern definition of carotid blowout describes a distinct syndrome that includes threatened (where there is radiological or clinical evidence to suspect future haemorrhage, such as an exposed carotid artery) and imminent (where there has been minor bleeding that has settled or been controlled) bleeding as well as acute carotid haemorrhage. 13 Carotid blowout is a well-known and much feared complication of advanced head and neck malignancy, whether treated surgically or with radiotherapy, and occurs in up to 3-4% of patients following neck dissection. 14 Surgical intervention for such patients, who often pose a high anaesthetic risk due to significant co-morbidity, is technically difficult, and it is often impossible to identify the exact source of bleeding due to tumour bulk, ongoing infection or soft tissue fibrosis following prior surgery or radiotherapy; surgery for carotid blowout is known to carry up to 40% overall mortality, with a 60% incidence of neurological complications.13–15 For this reason, patients experiencing acute carotid blowout have traditionally been managed with end-of-life comfort measures.
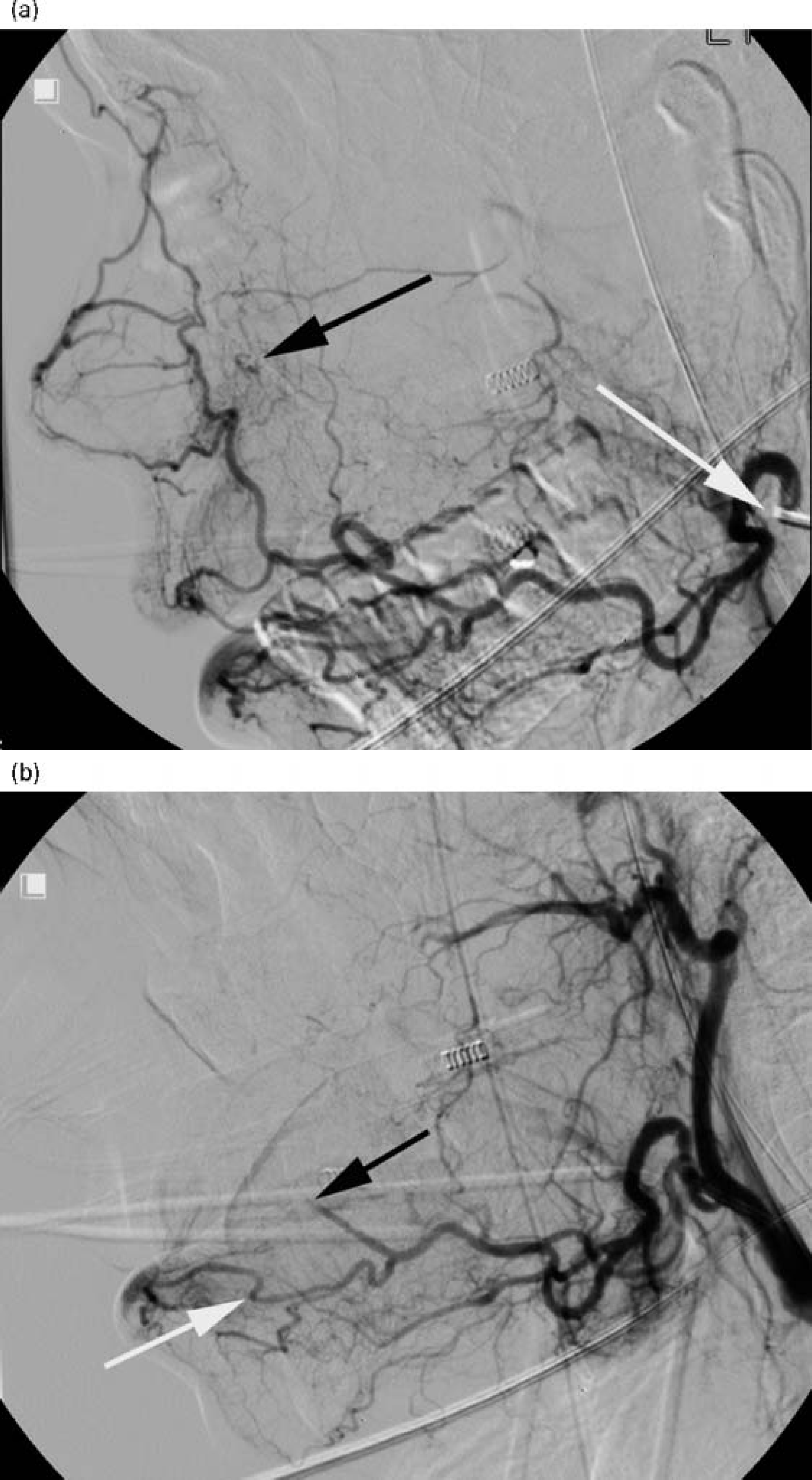
Endovascular treatment is now considered by some to be the gold standard for this group of patients. There are three main options available to the interventional radiologist. The first is permanent balloon occlusion (PBO), in which a detachable balloon is placed in the common carotid artery, preventing blood flow into the bleeding vessel. 13 In order to predict which patients are at risk from cerebral ischaemia, most advocates of this technique perform a temporary balloon occlusion test prior to PBO (Figure 2), although there is a recognized incidence of delayed cerebral ischaemia of up to 20%. 16 The second interventional technique available is selective embolization, using a variety of materials to occlude bleeding vessels, leaving the main carotid trunks intact. 17 The third option is placement of an endovascular stent, which also allows continued cerebral blood flow, and may be used alone or in combination with embolization.13–18–20 Successful treatment of patients with carotid blowout has led to the emergence of a new group of patients who present with recurrent haemorrhage or with delayed complications of endovascular stents.21,22 Whether a new presentation or a recurrence, it remains important for the head and neck surgeon to work closely with the interventional radiologist, as a part of the multidisciplinary team, and where possible with the patient, in order to decide when such treatment is appropriate and will lead to a continued quality of life for the patient.
(a)Temporary balloon occlusion test. The inflated balloon is seen in the left common carotid artery of a patient with uncontrolled haemorrhage secondary to malignant erosion of the carotid artery; (b) lateral view of the same patient after coil embolization; (c) this patient required permanent balloon occlusion to fully control the haemorrhage
Management of vascular lesions
Tumour embolization
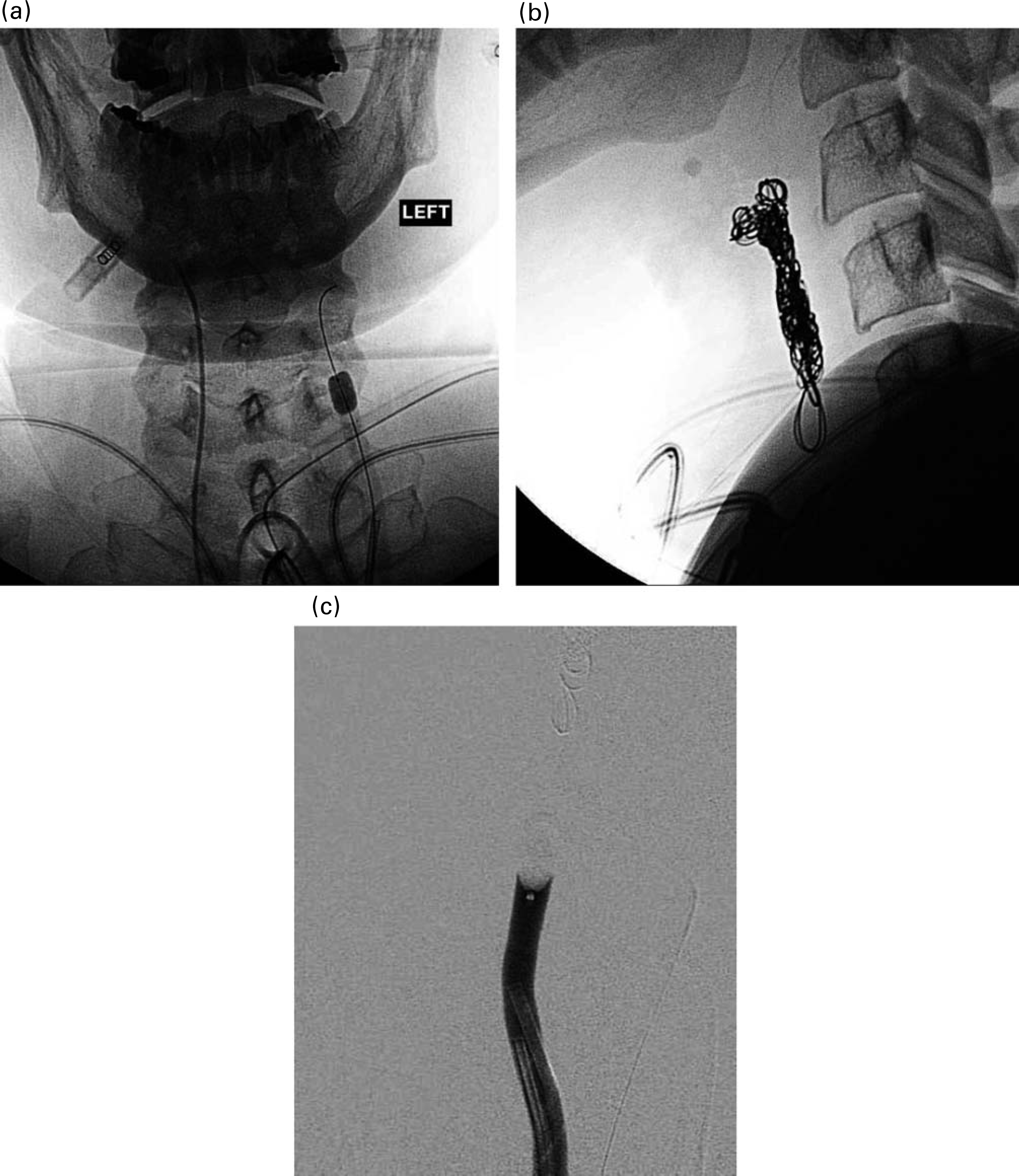
Embolization has been used in the treatment of a wide variety of head and neck vascular tumours, including congenital haemangiomas. The aim in most cases is to devascularize the tumour prior to surgical excision, although in patients unfit for anaesthetic, embolization may be used as a palliative measure. The commonest use of embolization is in the management of juvenile nasal angiofibroma (JNA), a rare, highly vascular benign tumour found in adolescent males. This lesion commonly originates in the pterygo-palatine fossa, and then expands aggressively through the sphenopalatine foramen into the nasopharynx and nasal cavities followed by the sinuses and orbit, finally extending intracranially Traditional surgical treatment has comprised an open approach using lateral rhinotomy or mid-facial degloving techniques. More recently, an endoscopic transnasal approach has been successfully described as safe and effective for all but the largest tumours. 23 Embolization devascularizes the tumour, minimizing blood loss during surgery and making an endoscopic approach more feasible, and for these reasons is now a well accepted part of the treatment of JNA. 24 Figure 3 shows how effective embolization can be in devascularizing JNA. For larger tumours, particularly those showing deep invasion of the sphenoid, there is evidence that a more radical surgical approach is preferable. In these cases, preoperative embolization may make complete tumour excision more difficult, and is not recommended. 25 Preoperative imaging with CT and MRI is therefore essential in planning the treatment for each case of JNA.

(a) DSA of juvenile nasal angiofibroma (JNA) showing microcatheter (black arrow) and tumour blush (white arrow); (b) after embolization there is minimal vascularity of the JNA
Embolization is also used in the treatment of paragangliomas, which are tumours arising from paraganglionic chemoreceptor cells. The commonest examples are glomus tympanicum, glomus jugulare and carotid body tumours. These tumours, which take their blood supply from the ascending pharyngeal artery, may be multicentric, and their ability to spread locally and small malignant potential are well described. Aggressive treatment is therefore recommended, and although surgery remains the mainstay of treatment, preoperative embolization has led to improved resecta-bility and reduced morbidity (Figure 4).26,27
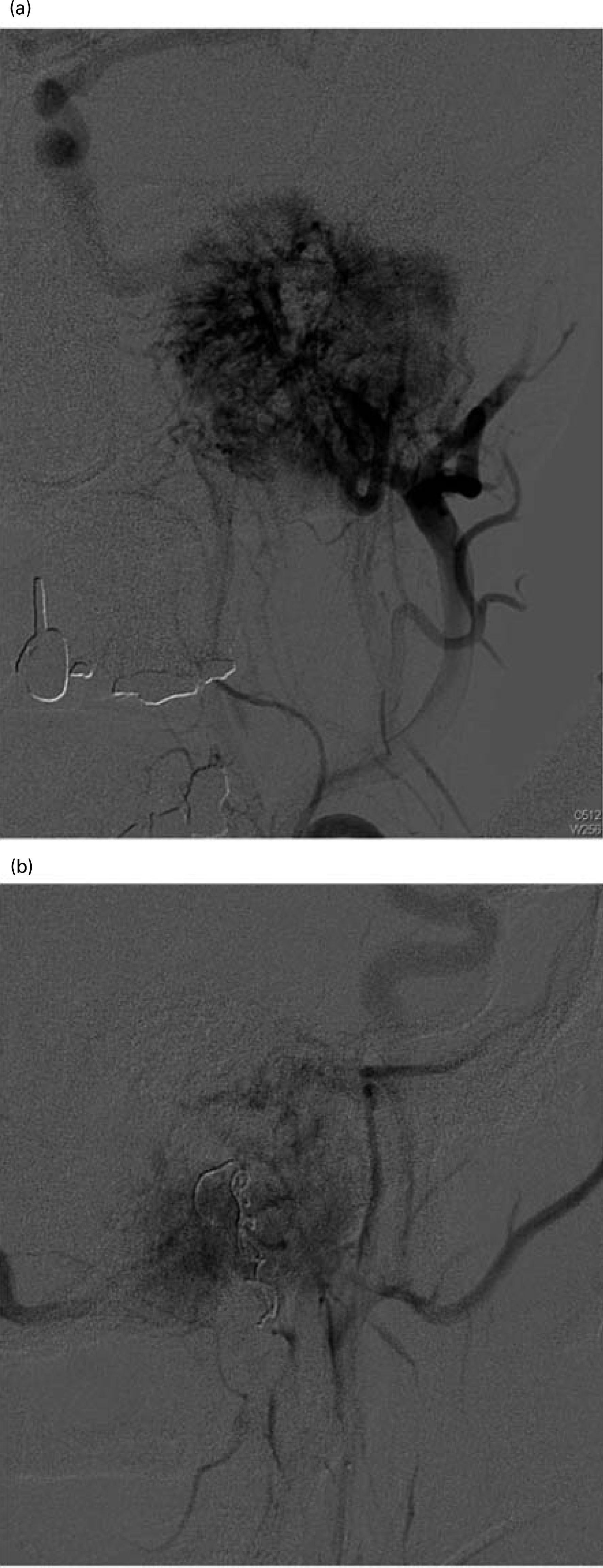
(a)Tumour blush of a large glomus tumour before embolization; (b) after embolization of the ascending pharyngeal artery with coils and particles the vascularity is reduced
Arterio-venous fistulas
These abnormal vascular connections can be congenital, spontaneous or traumatic. Treatment of congenital lesions is a challenge, as these have multiple, diffuse anastamoses with the surrounding vasculature. 28 Traumatic lesions can also be difficult to treat, in part due to the urgency of treatment required in order to prevent life-threatening haemorrhage, neurological deficit or visual complications. These lesions, such as the carotid to cavernous sinus fistula occurring after head injury, are also often inaccessible surgically. The principle of treatment of arterio-venous fistulas is preservation of the normal vasculature where possible, while ensuring that both the distal and proximal vessels of the fistula are occluded. Various treatment modalities have been described, including embolization with detachable balloons, particles or sclerosants, using both arterial and venous approaches, as well as placement of endovascular stents.28,30 Proper planning of treatment is the key to success, and again requires close cooperation between the interventional radiologist and the head and neck surgeon.
Venous sampling
In recent years, a minimal access approach to parathyroidectomy for the treatment of primary hyperparathyroidism has evolved, making preoperative localization of the abnormal parathyroid gland increasingly important. The usual techniques employed for this include combinations of sestamibi, ultrasound, computerized tomography (CT) and magnetic resonance (MR) scans. When necessary, usually if the above techniques have not convincingly localized the affected gland, or in re-operative cases, a further technique available is that of intraoperative selective venous sampling. In this technique, the veins draining the parathyroid glands can be catheterized and blood sampled for parathyroid hormone. Elevated levels identify the abnormal gland and can be seen to return to normal after surgery. This technique, though invasive, has a high sensitivity and accurately predicts patients who have been successfully cured. 31
Complications of interventional radiology
It is well recognized that interventional radiology procedures carry a risk of complications higher than that of angiography alone. Immediate complications include arterial puncture site haematoma, embolic or ischemic neurological deficits including visual disturbance, and, rarely, arterial rupture or contrast allergy. Later complications include delayed ischaemia which may present with neurological sequelae, including cranial nerve deficit, as well as pain and skin necrosis or paraes-thesia.32,33 Technological advances in the size and design of microcatheters has reduced the trauma and interruption to normal vascular flow that can be associated with interventional vascular procedures. In addition, access to much smaller vessels is now possible, allowing for highly selective vascular treatments, and reducing the incidence and severity of many of the possible complications. Infections may occur, those occurring around endovascular stents being particularly difficult to manage. 34 It must be remembered that, in many cases, similar complications can occur following surgical treatment. The treating radiologists and surgeons must therefore include the consideration of these risks in their decision-making process.
The future
Many of the most exciting advances in interventional radiology are in the treatment of malignant diseases. These applications include intra-arterial chemotherapy, radiofrequency ablation of tumours and catheter-directed gene therapy 35
There is currently much research into the role of endovascular carotid artery stenting in the treatment of carotid vascular disease, with comparisons to surgical carotid endarterectomy 36 This is a controversial area, and results of further studies are awaited.
It is certain that with the continual evolution of imaging technology, improved design of micro-catheters allowing increasingly selective vascular access, and the increasing availability of interventional radiology services, their use will expand. 37 As the specialty grows, it will be possible to safely offer more procedures on an outpatient basis. 38 This will require increasing cooperation between specialties, and in the future some authors predict direct referrals to interventional radiology from general practitioners. 39
Conclusion
The role of interventional radiology in the treatment of head and neck conditions is increasing, but remains controversial. In some cases, such as the treatment of the carotid blowout syndrome, endovascular treatments have been shown to be superior to surgical treatment, and are rapidly becoming the gold standard for cases where intervention is appropriate. In most cases, as in the preoperative embolization of tumours or in parathyroid venous sampling, interventional techniques and surgery can be used as complementary therapies. In some conditions, such as in the management of epistaxis, the exact role of endovascular therapies is still debated.
Head and neck surgery trainees must continue to be taught the necessary techniques to deal effectively with all of these conditions, but must also understand the role of interventional radiology in order to be able to offer the highest possible quality of care to their patients.
Footnotes
Acknowledgements
None