
Abstract

Introduction
The Burkholderia cepacia complex (Bcc) is a group of Gram-negative, non-spore-forming bacilli representing at least nine closely related bacterial species, of which Burkholderia cenocepacia and Burkholderia multivorans are the most prevalent in cystic fibrosis (CF). Outcome with Bcc infection can be difficult to predict for an individual CF patient, but generally it has been shown to correlate with a worse prognosis, longer hospital stays and an increased risk of death.1–3 ‘Cepacia syndrome’ is a term used to describe an important subgroup of Bcc-infected patients who develop a rapidly progressive pneumonic process associated with high fevers, positive blood cultures, respiratory failure and high mortality. 4
DECLARATIONS
None declared
None
Not applicable
NJS
Both authors contributed equally
The present case report describes a CF patient who, despite having B. cenocepacia for 13 years, had an excellent state of health with stable disease until he developed a large chest wall B. cenocepacia abscess and - despite aggressive medical and surgical management - deteriorated rapidly with sepsis, multiorgan failure and eventual death.
Case report
A 31-year-old man with CF was admitted complaining of fevers, worsening of his cough and a right-sided anterior chest wall lump’. CF had been diagnosed at 2½years of age after recurrent chest infections. He was homozygous ΔF508 and had a history of pancreatic insufficiency, nasal polyposis and distal intestinal obstruction syndrome. B. cepacia (later confirmed as B. cenocepacia) was first isolated in his sputum at the age of 18 years (prior to that only Staphylococcus aureus was present). At that stage FEV1 was >100% predicted and body mass index (BMI) was 20.5 kg/m2. FEV1 decreased to 80% predicted over the subsequent two years but remained >70% predicted thereafter (BMI >20 kg/m2) until the presenting problem. During this period he was fully active with no exercise limitation and required only one course of intravenous antibiotics.
Two months before the current admission he attended a routine outpatient appointment and gave a vague history of occasional mild fevers but otherwise was well with good lung function (FEV1 2.8L, 70% predicted) so no treatment change was initiated. Nineteen days later he was admitted to hospital with a six-day history of fevers, mild right-sided chest pain, slight increased sputum production and a C-reactive protein (CRP) of 195. He received 14 days of piperacillin-tazobactam and ceftazidime with good symptomatic improvement. One month before the current admission he was admitted again with fevers, a high CRP (189) and now described the chest pain as ‘pleuritic’. Subtle right-sided chest radiograph changes were noted and he received ceftazidime and tobramycin for two weeks.
On day one of the current admission he was pyrexial (38.5°C) and his lung function had deteriorated (FEV1 2.03). A 3×5 cm firm, tender mass was present over the right upper anterior chest wall extending from the clavicle to the nipple. Thoracic computed tomography (CT) revealed extensive right upper lobe consolidation and a heterogeneous mass deep to the pectoralis muscle (Figure 1). An ultrasound scan of the chest wall mass showed no obvious collection and only 2 mL of blood-stained fluid was aspirated with difficulty. Aspirate, blood, sputum and wound swab cultures all grew B. cenocepacia. HIV testing and immunoglobulin levels were normal. Cultures were all sensitive to ceftazidime and tazobactam and intermittently sensitive to minocycline, chloramphenicol, meropenem and temocillin.
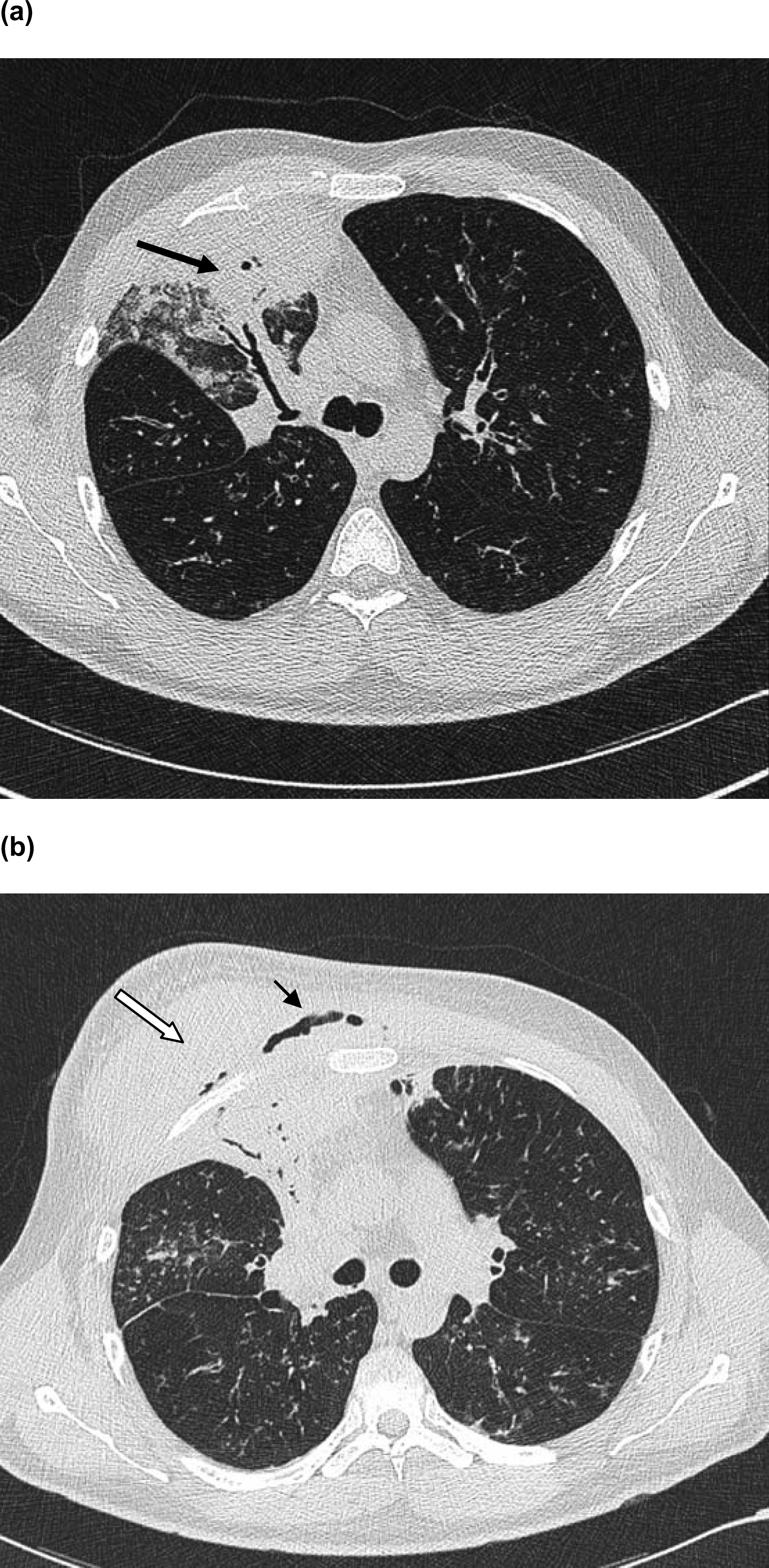
(a)Thoracic computed tomography on day 2 of the third admission demonstrating widespread cylindrical bronchiectasis and extensive right upper lobe consolidation (arrow). (b) By day 29 of the third admission the mass (white arrow), deep to the pectoralis muscle, has significantly increased in size and contains air (small arrow), indicating possible fistula formation.
The mass continued to increase in size over the subsequent three weeks despite treatment with a high-dose combination of the above antibiotics in addition to tobramycin and co-trimoxazole. Furthermore, the patient remained septic with a high temperature, elevated CRP (Figure 2) and leukocytosis. As the mass enlarged, pain over the area intensified, requiring strong opioid analgesia. Surgical drainage was considered, but due to its difficult location and the apparent lack of fluid, surgery was not performed at that stage. Subsequently a true-cut biopsy revealed granulation tissue with inflammatory cells only, confirming abscess formation (the culture grew B. cenocepacia). His condition continued to worsen over the following week despite continuing with high-dose combination antibiotics and a trial of steroids. A repeat CT scan showed air in the subcutaneous deep tissue, indicating the abscess had broken down and suggesting a fistula had formed (Figure 1); open surgical drainage was therefore performed under general anaesthesia. 100 ml of pus was drained and small drains were left in situ.
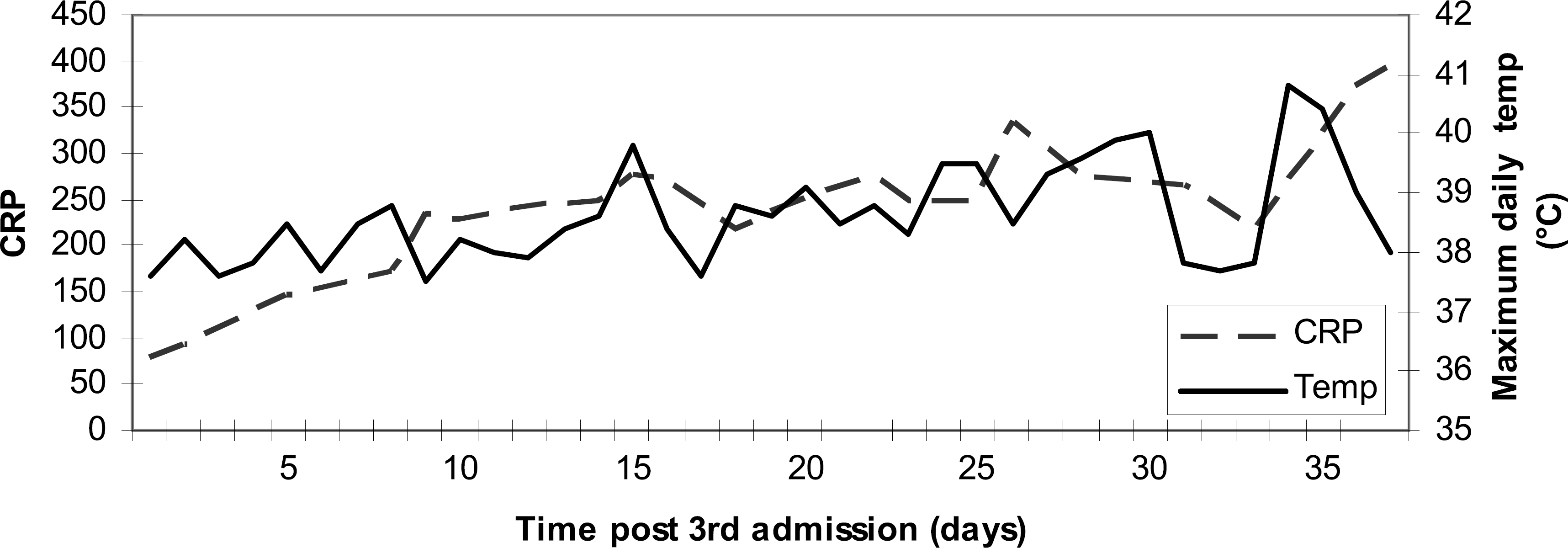
Clinical course, demonstrating the relentless swinging pyrexia and high CRP
Postoperatively, the chest wall mass was considerably reduced in size and the pain was much better. However, the patient remained pyrexial and over the next two days the chest radiograph rapidly deteriorated and acute renal failure developed, requiring haemofiltration. A decision not to escalate treatment (i.e. inotropes / mechanical support) due to his poor prognosis was taken after extensive discussion with the patient's family. Respiratory function continued to deteriorate and he died 24 hours later of sepsis and multiorgan failure.
Postmortem showed an abscess present on the anterior and posterior surface of the right rib cage, involving the sternum and fourth to sixth ribs, extending into the right upper lobe of the lungs (Figure 3). All microbiological cultures grew B. cenocepacia.
Discussion
Bcc, originally called Pseudomonas cepacia, was first identified in the 1940s as a plant pathogen causing onion rot, but it was not until the 1980s that it was first recognized as an important pathogen in CF. 4 It has since been shown to be associated with a deterioration of lung function and increased mortality, although these early observations came before the sub-classification of Bcc into different species.3,5,6 With improved microbiology techniques, the taxonomy has evolved and now includes nine phylogenetically distinguishable species or genomovars. 7 Subsequently, it has been recognized that B. cenocepacia carries a worse prognosis compared with B. multivorans, with shorter survival when matched with P. aeruginosa controls. 8 Cepacia syndrome has been reported with both of these species. 8 The exact pathophysiology of this syndrome is poorly understood and the precise mortality rate is not known, although it is thought to approach 100%. 9
Two clinical features make this case unique. The first was the length of time between the onset of Bcc colonization and the development of his final illness. During those 13 years the patient had been very stable with no physical restriction due to his CF. Cepacia syndrome generally occurs soon after first isolation, although one case report of it occurring nine years after colonization exists. 10 The second, most striking, feature of this case was the development of a chest wall mass, which is an extremely unusual manifestation of the disease. Initially the mass contained limited fluid and, due to its radiological appearances, actinomycosis was considered as part of the differential diagnosis, but B. cenocepacia became the most likely aetiology after it was cultured from all the microbiological specimens (abscess aspirate/biopsy, blood and sputum).
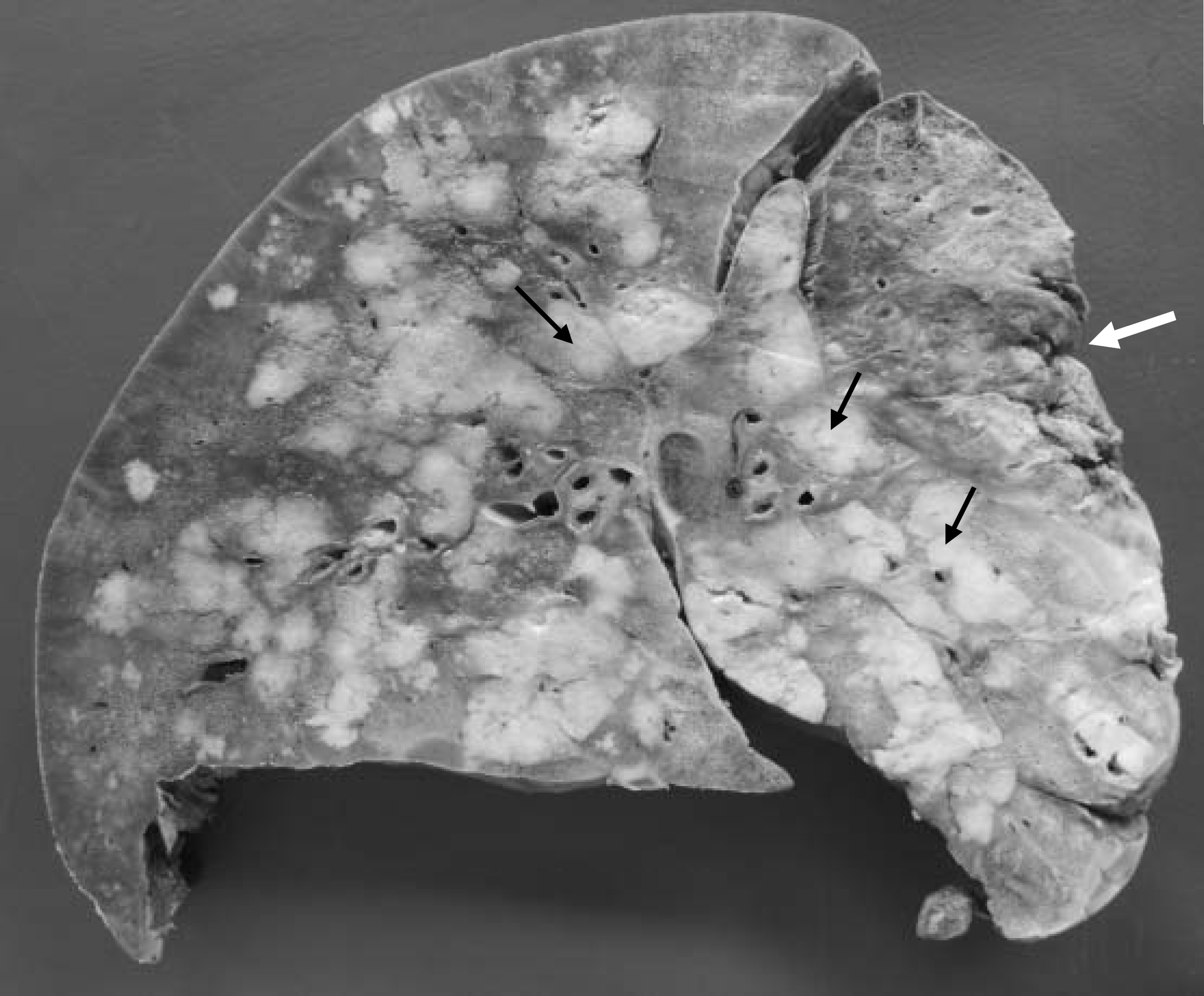
Post-mortem macroscopic appearance demonstrating widespread abscess formation (examples highlighted by black arrows) with destruction of lung tissue and surrounding necrosis in the right upper lobe (white arrow).
Pulmonary microabscess formation is recognized as a potential sequelae to Bcc infection, 4 but large abscess formation is extremely rare. An electronic search using the terms ‘abscess’, ‘cenocepacia”, ‘cepacia’ and ‘Burkholderia cepacia complex’ in PubMed, Embase and Medline (Ovid), covering the period 1950-2007, only yielded one description of such a process in an immunocompetent CF patient. This occurred in a 40-year-old man with cepacia syndrome, mediastinitis and a mediastinal abscess who died despite aggressive antimicrobial treatment and surgical drainage. 11 Other descriptions in CF are limited to the post-transplant period in immunosuppressed patients.12,13 However, abscess formation secondary to Bcc has also been reported in chronic granulomatous disease (CGD) - a condition in which oxidative phagocytosis is disabled. 14 This provides insight into the virulent mechanisms of Bcc; it is highly resistant to nonoxidative phagocytosis, thus leaving CGD patients extremely vulnerable to infection. Consequently, a proposed mechanism for the susceptibility to Bcc infection in CF is an imbalance between oxidative and nonoxidative phagocytosis. 7
Bcc's virulence can also be partly explained by its cellular lipopolysaccharide, which is more endotoxic and induces increased neutrophil burst activity and levels of interleukin 8 compared with P. aeruginosa. 15 Another putative virulence factor includes the production of biofilms. 16 Biofilms are communities of bacteria that are protected from many environmental factors; Bcc biofilms have been shown to be resistant to ceftazidime and ciprofloxacin and are also thought to be protected from various host defence mediators. 17 A structural component of Bcc which interferes with the clearance of secretions, thus increasing its virulence, is the presence of a cable and mesh pilus which bind to tracheobronchial mucin and facilitates adherence to cells. 17
Regardless of these mechanisms of infection, it is not clear why abscess formation occurred in the present case. The underlying integrity of the immune system is the most obvious explanation; however, no immune deficiency was identified, although extensive testing (including of neutrophil function) was not performed. In spite of Bcc being regarded as an opportunistic infection, there are reports of abscess formation in non-CF/non-CGD immunocompetent patients, including a brain abscess secondary to chronic suppurative otitis media 18 and microabscesses in three patients with pneumonia. 19 Other reports of neurological and pulmonary abscesses occurred in non-CF patients with identifiable risk factors (diabetes and an IV drug user).20–22 Although the above examples are rare case reports, they serve to highlight the complexity of Bcc infection and, in particular, our limited understanding of why abscess occurs in certain clinical situations.
Bcc is notoriously difficult to treat as it has broad-spectrum innate antimicrobial resistance, due to several mechanisms. In addition to the bio-film theory, these include a novel antibiotic efflux pump, 23 a trimethoprim-resistant dihydrofolate reductase, decreased permeability of its outer membrane (especially to β-lactams) and inducible chromosomally encoded β-lactamases. 17 Multiple different antibiotic regimens were used in the present case without significant clinical improvement. Corticosteroids, which have been reported to be beneficial in isolated cases in cepacia syndrome, 24 were also ineffective.
Conclusion
The present report describes a patient with CF and B. cenocepacia colonization who developed cepacia syndrome and a large penetrating chest wall abscess. Despite multiple different antibiotic regimens and a trial of steroids, combined with surgical drainage, the patient died of the infection. The case highlights the unpredictability of this pathogen, which has the ability to develop into cepacia syndrome and abscess formation many years after initial colonization. Awareness of these potential complications is crucial, but until more treatment options are developed it will always provide a considerable challenge to those caring for patients with CF.
Footnotes
Acknowledgements
The authors acknowledge and thank Dr Mary Sheppard for her pathology advice and for providing the postmortem illustration.