
Abstract
Summary
A 35-year-old woman collapsed 18 hours after undergoing abdominal wall liposuction. Abdominal CT scan revealed a punctured spleen. She underwent an emergency splenectomy and made an uneventful recovery.
Case report
A 35-year-old woman presented to plastic surgeons with increased adiposity in the lower trunk and upper thigh. She did not have any significant past medical or surgical history and was not taking any regular medications. Her preoperative haemoglobin level was 11.2 g/dL. She underwent abdominal wall and upper thigh tumescent liposuction through suprapubic and lateral abdominal wall stab incisions under general anaesthetic. She made an uneventful initial recovery from the anaesthetic and slept pain-free throughout the first night. Sixteen hours hours after surgery she complained of acute onset of severe generalized abdominal pain and abdominal distension and collapsed. On examination she had marked pallor and class II hypovolaemic shock. She responded to initial fluid resuscitation.
She was transferred to an acute general surgery hospital. On admission she was noted to have marked pallor, severe hypovolaemic shock (class III) and a tense distended abdomen. The general surgery and anaesthetic team were paged as an emergency within five minutes of the patient arriving. She had superficial abdominal bruising at the site of liposuction and mild diffuse abdominal tenderness. There was no abdominal guarding or signs of peritonism present. The bowel sounds were reduced and digital rectal examination was normal. Her blood results revealed haemoglobin level of 3.6 g/dL. She made a moderate recovery to aggressive fluid resuscitation. She was urgently transfused six units of whole blood, type specific blood was given within 15 minutes, followed by cross-matched blood within one hour. After initial resuscitation her blood pressure was stable at 110/60. Her repeat haemoglobin level was 10.6 g/dL. She continued to have persistent tachycardia, with a pulse rate of 110 bpm.
A rapid Focused Abdominal Sonography for Trauma (FAST) abdominal ultrasound scan was
performed within 30 minutes, first by the emergency department consultant, then by the
radiology specialist registrar. The FAST scan was positive for intra-abdominal fluid;
the source of bleeding could not be identified, however, as the scan was difficult to
interpret due to the recent liposuction. A computed tomography (CT) scan was done within
a hour of the ultrasound scan. It showed a large volume of free intraperitoneal fluid in
perihepatic space, paracolic gutters and pelvis. The spleen was displaced medially with
heterogeneous haematoma seen laterally with active contrast extravasation indicating
persistent bleeding. The haemorrhage was extraperitoneal but deep to the abdominal wall
musculature ( Large amount of diluted blood surrounding the liver (A) and large amount of
blood extravasating from the spleen (B)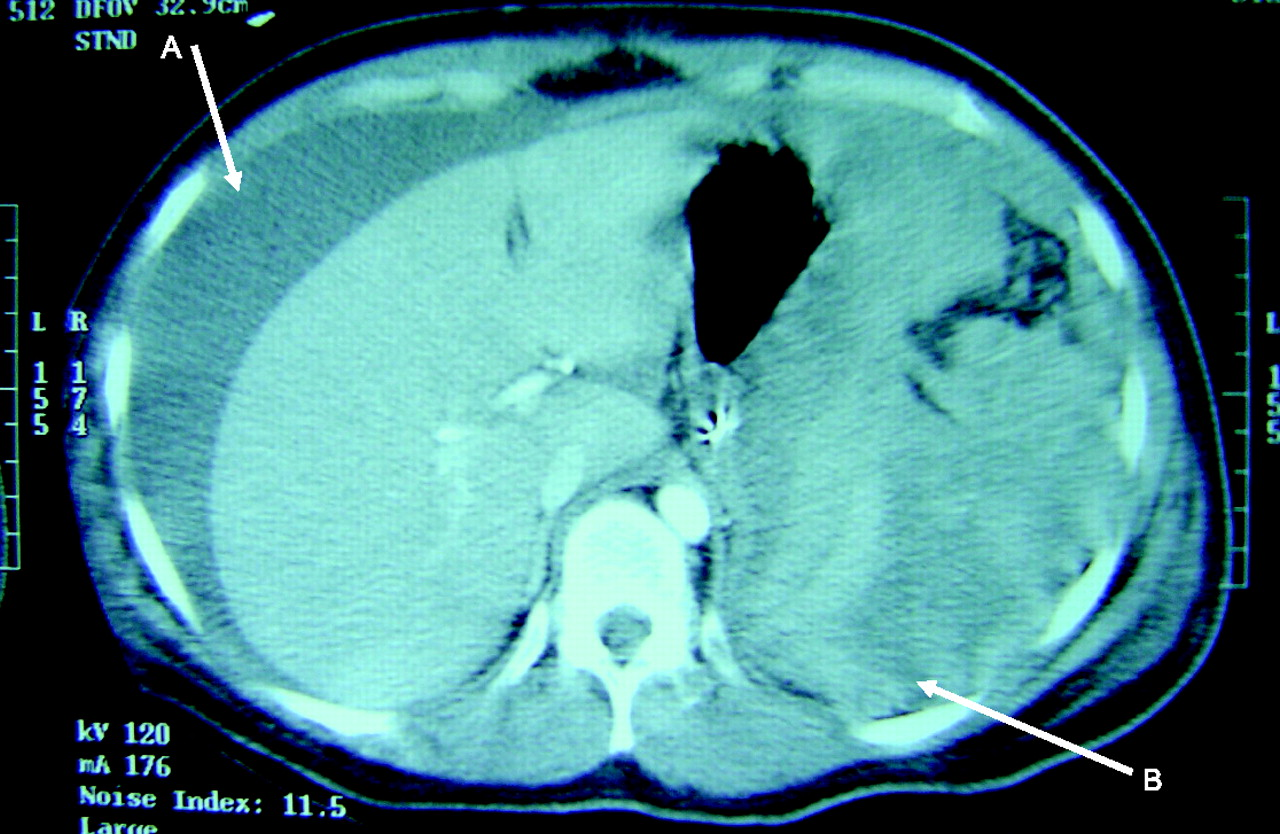
As the patient had continuing abdominal distension and pain she underwent an emergency laparotomy within 4 hours of arriving in the resuscitation room. Perioperatively, she received six units of packed red cells, three units of fresh frozen plasma, one unit of platelets and 300 mL of cryoprecipitate. At emergency laparotomy she was found to have approximately two litres of diluted blood in the abdomen. The superficial layer contained clear fluid, with blood in the lower sedimented layer. One litre of fresh blood was drained from the abdomen and one litre of clotted blood was evacuated from the lower abdomen. Rapid continuous packing of the abdomen with large swabs revealed that the source of the bleeding was a damaged spleen. A distinctive trochar puncture mark in the lower lateral pole of spleen was identified, and splenectomy was performed. There was no further bleeding noted. The patient made an uneventful postoperative recovery. Postoperatively she received vaccination against HIB and pneumocccocus and was discharged home on oral penicillin medication. At follow up in clinic at six weeks there were no problems noted.
Discussion
Reported complications of abdominal liposuction
Major non fatal complications can occur in 0.14–0.38% of cases and include anaesthetic complications, deep venous thrombosis, pulmonary embolism and fat embolism. 1 , 3 Intraoperative acute fluid imbalance may cause acute renal failure, pulmonary oedema or cardiac failure and intraoperative cardiac arrest. 10, 11, 12, 13
Fatal complications have been reported, with risk of death varying from 3 to 100 per 100,000. In a large series from the USA between 1994 and 1998, Grazer et al. reported 95 deaths out of 496,245 operations (19.1 per 100,000). 14 Though mortality from liposuction procedures is reported as 0.003–0.02%, some authors claim higher rates, with pulmonary embolism as leading cause (23.4 ± 2.6%). 15 The second most common cause of death is abdominal viscus perforation (14.6%), with up to 50% mortality following the perforation. 10 Rao et al. analysed three deaths between 1993 and 1998 in the New York area. His data suggested that there is controversy surrounding the normal dose of lignocaine (10–55 mg/kg), and that lignocaine toxicity could have contributed to bradycardia, hypotension and cardiac arrest. 16 Other causes of mortality include anaesthetic complications (10%), adult respiratory distress syndrome, and fat embolism (8.5%). 12 , 17 , 18 For further reading on the morbidity and mortality of abdominal liposuction, we recommend the review by Yoho et al. 19 In conclusion, doctors and surgeons should be aware of the many complications of liposuction as these patients may present to the accident and emergency department.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
None