
Abstract

Sometimes there is a need to answer important clinical questions quickly. The Research Governance Framework (RGF) for Health and Social Care, which was introduced in England in 2005, aimed to improve the efficiency and quality of research in the NHS, but has introduced a new layer of bureaucracy which is preventing important questions being answered. 2007 saw the publication, in the JRSM, of two studies highlighting the unacceptable bureaucracy in the Research and Development system (
Other systems have successfully removed unnecessary bureaucracy, and a useful model is the Multicentre Research Ethics Committees (MREC). Variations in the functioning of ethics committees had erected barriers to research and a new system of multicentre ethics approval was introduced in the UK during the last decade to address some of the problems highlighted by researchers when undertaking studies involving more than one site. 3 The use of standardized means of assessment by the new multi-centre research ethics committees means that their approval is transferable throughout the entire UK. 4 Local R&D offices are now throwing up the same barriers that local research ethics committees once were and currently constitute the major impediment to multi-site research. 4 , 5
Sometimes failure to answer important questions quickly can have major implications for clinical practice. For example, we attempted to survey UK psychiatrists in response to an urgent need to describe their prescribing practice. In December 2003, the Committee on Safety of Medicines (CSM) issued guidelines suggesting that fluoxetine was the only safe antidepressant for use in child and adolescent depression. Clinicians were struggling with having to implement an immediate and radical change in their practice and we wanted to find out how they (and, by inference, their patients) were coping with this by implementing a nationwide questionnaire survey.
As our study was low risk, specific written approval by R&D offices other than our local one was not deemed necessary by MREC, but we were advised inform all relevant R&D offices. However, nearly one-third of all primary care trusts then requested further information. To our dismay, we found ourselves in the midst of a slowly emerging and eventually insurmountable bureaucratic response from the R&D departments, as demonstrated in Figure 1. There was an alarmingly wide variation in requirements, ranging from requests for simple documentation to the request that all members of the Scottish research team apply for honorary clinical contracts in a particular English Hospital Trust.
The survival graph shows that after 70 days, we only had formal approval from 15% of PCTs. From the shape of the curve, it is clear that our study would never have gained approval from all the relevant parties, at least within our research project's (or researchers') lifetime. Reluctantly, we realized that our urgent and important question had been condemned to a bureaucratic trashcan.
We attempted to drive forward a national response to the problem by describing our abandoned study to key UK policy figures, but despite significant efforts it proved impossible to influence change in the system for the UK as a whole. Fortunately the Scottish R&D Consortium was more receptive, and as a direct result of our findings, there are now plans to pilot a Multi-Centre Research and Development Office (MRAD) that will create a standardized system in Scotland.
Survival plot for R&D approval (Kaplan-Meier method)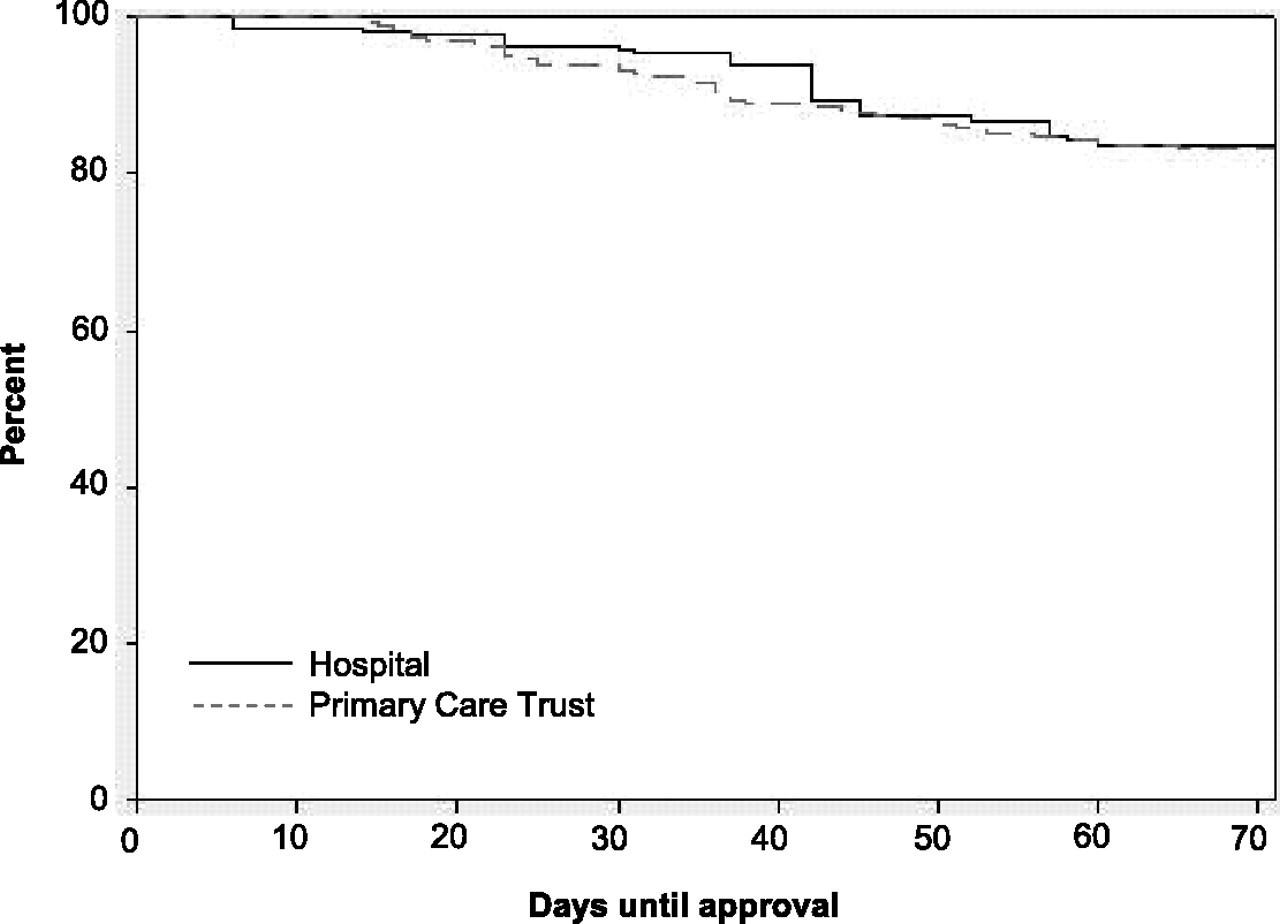
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
None