
Abstract
Summary
Various physiological processes can cause potentially misleading appearances in radioiodine whole body scans; proper understanding of the causes of these can therefore obviate diagnostic errors. Whole-body radioiodine scintigraphy with I131 or I123 is an accurate form of imaging used for management of differentiated thyroid carcinoma. Following thyroidectomy, any residual thyroid tissue or metastatic disease is ablated with high dose I131 and diagnostic images are acquired, demonstrating residual thyroid tissue and metastatic disease. However, atypical physiological uptake of I131 can simulate metastases.
Case history
A 29-year-old woman attended the endocrinology outpatient clinic for a mass in the left side of her neck of five years duration. There had been a recent increase in the size of the mass. Fine needle aspiration revealed papillary carcinoma of the thyroid in the left-sided neck nodes. At this time, the patient was three weeks post natal.
Seven weeks after the initial diagnosis was made, the patient underwent total thyroidectomy and left-sided modified radical neck dissection. Histological examination of the operative specimen confirmed the diagnosis of well-differentiated papillary carcinoma in the superior pole of the left lobe of thyroid. There was lymphatic invasion with extensive involvement of the neck nodes.
Nine weeks following surgery, the patient received 3.1 GBq of I131 as an
ablative dose for the thyroid remnant. Whole body imaging following I131
administration was performed to look for residual thyroid tissue, and also for local and
distant metastases. An irregular focus of uptake was present in her right breast only
( A: Whole body imaging with I131 scintigram. Anterior image shows a
unilateral irregular focus of uptake in the region of the right chest wall
(arrow). Physiological uptake is also noted in the stomach and bladder.
Specifically, there is no residual uptake in the neck. B: Whole body
I131 scintigram. Right lateral image localizes the uptake to the
right breast. [In colour online.]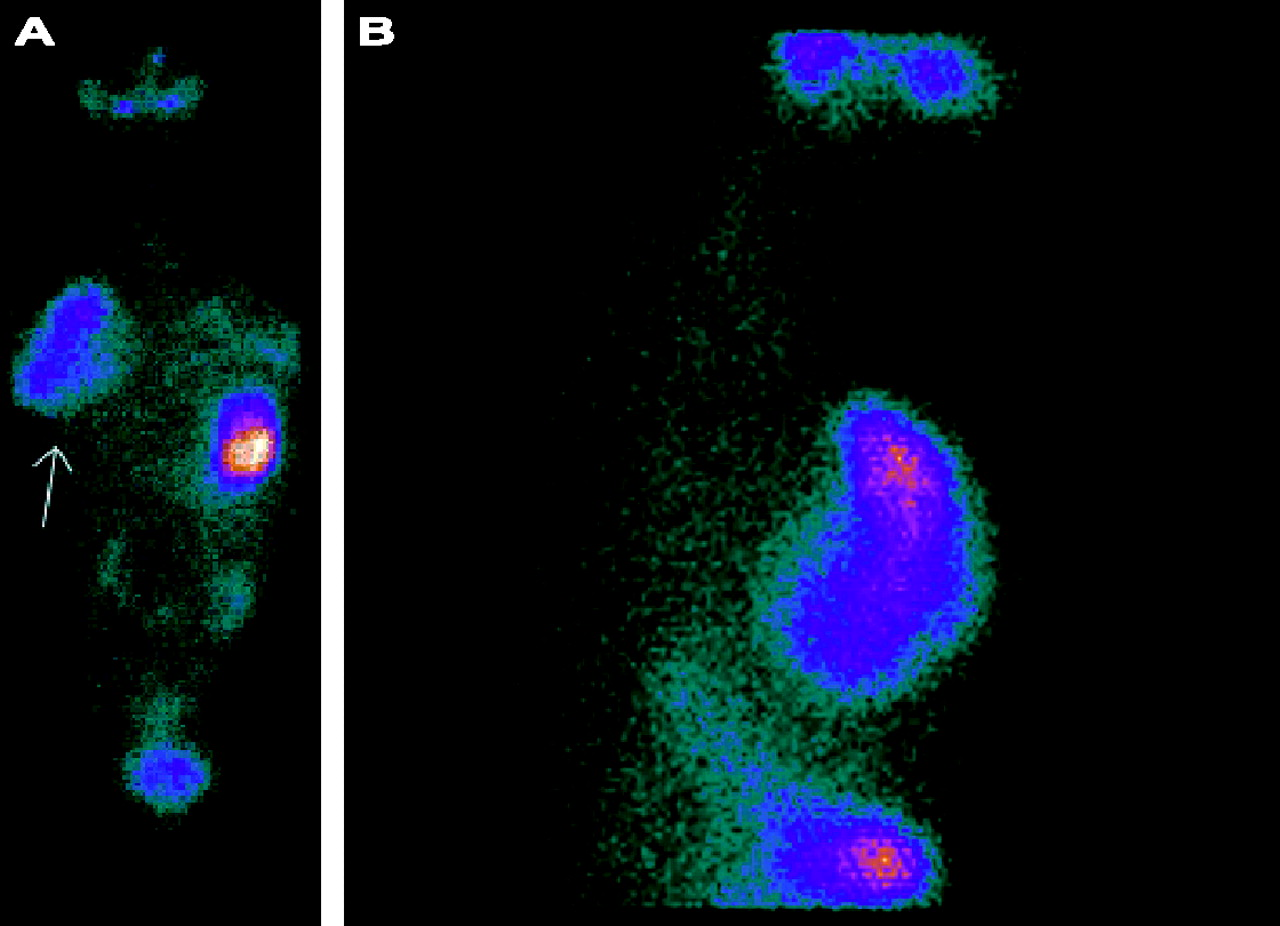
The patient had just ceased breast feeding prior to her therapy, and it transpires that
she had used only her right breast, giving the unusual pattern of iodine uptake. A
follow up diagnostic I123 scinitigram performed after 12 weeks showed no
uptake of radioiodine in either breast ( I123 scintigram obtained after 12 weeks shows no uptake in either
breast. No evidence of residual thyroid tissue or malignancy
Discussion
Whole body I131 scintigraphy is a commonly used procedure in the management of patients with differentiated carcinoma of the thyroid, post thyroidectomy. The presence of sodium iodide symporters in the basolateral surface of the thyroid follicular cells results in sodium-dependent active transport of iodine, its organification and retention. This forms the basis for investigating thyroid disorders and for ablation of thyroid using radioactive iodine, I131, which is both a gamma emitter (diagnostic), and a beta emitter (therapeutic). A diagnostic whole body scan performed at the time of radioablation of thyroid shows the presence of residual thyroid tissue, local and distant metastases.
Although this is a highly sensitive method for detecting thyroid tissue, false positive uptake can be seen in other organs possessing sodium iodide symporters. Normal physiological uptake occurs in salivary glands, the stomach and ectopic gastric mucosa. 1 Radioiodine is also taken up in lactating and non-lactating breast tissue, 2 and there are reports of over-expression of sodium iodide symporters in breast malignancies. 3
Bakheet and Hammani 4 have described four patterns of uptake in the breast in twenty female patients one week after they stopped breast feeding: ‘full’, ‘focal’, ‘crescent’ and ‘irregular’. The full pattern represents intense uptake over the entire breast. Central, subareolar uptake gives a focal pattern of uptake, whereas more intense peripheral uptake represents a crescent. The underlying cause for these patterns in not known. The fourth, irregular pattern of uptake, however, can mimic metastases. Thus while full, bilateral uptake is typically physiological, unilateral or irregular uptake was suggested to be highly suspicious for malignancy.
Preferential lactation from one breast is a common occurrence among breast feeding mothers. However, it can give rise to highly unusual and indeed suspicious imaging appearances. In this case, unilateral uptake of I131 was present in the right breast only as the patient had preferentially lactated only from the right side. This unusual pattern of iodine uptake should not be mistaken for metastatic disease or a breast primary. Careful history taking helps to avoid such diagnostic pitfalls.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
None