
Abstract
Summary
Objective
To assess reasons for low uptake of immunization amongst orthodox Jewish families.
Design
Qualitative interviews with 25 orthodox Jewish mothers and 10 local health care workers.
Setting
The orthodox Jewish community in North East London.
Main outcome measures
Identification of views on immunization in the orthodox Jewish community.
Results
In a community assumed to be relatively insulated from direct media influence, word of mouth is nevertheless a potent source of rumours about vaccination dangers. The origins of these may lie in media scares that contribute to anxieties about MMR. At the same time, close community cohesion leads to a sense of relative safety in relation to tuberculosis, with consequent low rates of BCG uptake. Thus low uptake of different immunizations arises from enhanced feelings of both safety and danger. Low uptake was not found to be due to the practical difficulties associated with large families, or to perceived insensitive cultural practices of health care providers.
Conclusions
The views and practices of members of this community are not homogeneous and may change over time. It is important that assumptions concerning the role of religious beliefs do not act as an obstacle for providing clear messages concerning immunization, and community norms may be challenged by explicitly using its social networks to communicate more positive messages about immunization. The study provides a useful example of how social networks may reinforce or challenge misinformation about health and risk and the complex nature of decision making about children's health.
Introduction
Concern about the re-emergence of certain childhood infectious diseases has followed evidence about declining rates of immunization since publicity was given to claims associated with a (now discredited) 1998 study 1 of the triple MMR vaccine and autism. During 2003/04, more than two thirds of Primary Care Trusts (PCTs) in England (221 of 294) reported less than 85% coverage for MMR. 2 Local variations included 19 PCTs with coverage below 70%, 15 of which were located in London.
Lower rates of childhood immunization have been found amongst disadvantaged
communities
3,
4,
5
and within certain minority ethnic communities where uptake of preventive health
programmes has traditionally been low.
6
,
7
In the City and Hackney area of east London there are exceptionally low rates of
immunization amongst the orthodox Jewish community (46% for both diphtheria and MMR), in
spite of relatively high rates (80 and 90%) for other ethnic groups in the area and an
overall rate of 70% of children aged two being immunized for MMR
8
( Population Database: Regional Interactive Child Health System (2002)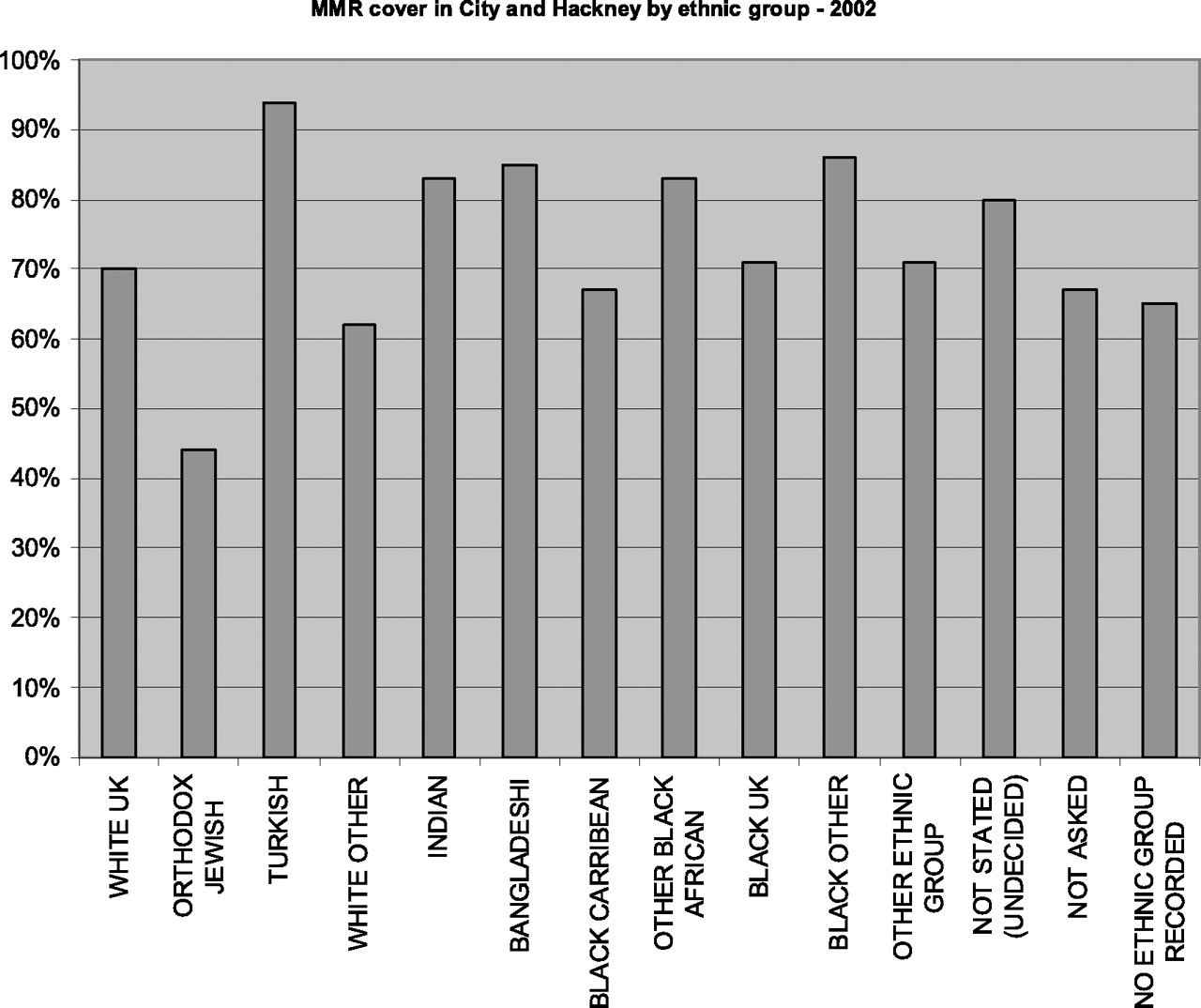
Quantitative studies conducted before the MMR media scare found that this community valued immunization but wanted better access to services. 9 Perceptions of unsympathetic treatment by practice staff, logistical difficulties associated with large family size and fears of allergic reactions have also been identified as factors in explaining low immunization uptake. 10 In relation to BCG immunization, also low in orthodox Jewish groups, explanations have pointed to the perceptions of community members that they are less vulnerable to tuberculosis because of a mutual aid ethos which historically has prevented families experiencing dire poverty, and are safe from infection by ‘outsiders’ because of the enclosed nature of the community. 11 The influence of mass media (television, newspapers, magazines and the internet) on attitudes to immunization in this community is assumed to be weak because reluctance to integrate with other ethnic groups leads community members to resist exposure to such media. 12 Communicating risk is complex and messages are not received or interpreted in a homogeneous way in the general population, 13 yet very little is known about how such messages may be filtered and circulated within minority communities.
Our study investigates whether there are specific religious or ethnic reasons for low uptake of immunization amongst orthodox Jewish families in North East London and explores perceptions of barriers such as larger family size, the role of local health care services, and the significance of wider sources such as local and national media reporting.
Setting
The orthodox Jewish community in North East London is the largest such community in Europe. The 2001 Census 14 indicated that 5.3% of Hackney residents are Jewish, although local estimates suggest that the actual figure may be double this, with approximately 20,000 members. The community is largely insular, providing many services for its members. Adhering strictly to Jewish law means that the cost of living for this group is higher than for others. Key factors include the cost of kosher food and the need, for religious reasons, to send children to private Jewish schools. There is also evidence of more domestic overcrowding in the orthodox Jewish population, as families tend to be larger and have more children under 16 in comparison with other groups. 15
Good health is regarded extremely highly and it is considered to be a religious obligation to seek medical attention when ill. 16 It is not uncommon for serious illnesses to be concealed, particularly hereditary, chronic or mental illness. There are many diverse voluntary groups within the community which provide health and social care services. While local statutory health services are used in times of illness, or where there is a need for hospitalization (particularly maternity), the use of complementary health care facilities and practitioners is growing in popularity. Some health promotion activities are not considered appropriate, such as inviting unmarried women to participate in cervical screening. 17
Methods
The orthodox Jewish community is particularly difficult to reach as secular contact is regarded with suspicion. Records of two general practices known to serve a high proportion of the orthodox Jewish community were used to select children aged between 2–3 years. Mothers were contacted by letter and telephone, with researchers emphasizing that the study was independent of their GP and their religious community. A total of 14 women agreed to take part. We also used ‘snowballing’, where participants are asked to suggest others who may take part, and a further 11 women were recruited in this way. This is a common method for qualitative investigations of populations that are otherwise hard to reach or who have limited contact with health professionals and allows us to further examine the social processes which surround health decision making. 18 , 19 There were no significant differences in characteristics between the two groups. Most respondents (20 of 25) were born and had lived in the area all their lives. The mean age of mothers was 29.7 years (range 21–44). Family size varied, with women having between one and nine children (mean 4.1). Most participants (21 of 25) had no additional educational qualifications beyond completing secondary school.
Preliminary background interviews were conducted with ten health care staff who had significant contact with the community through local GP practices and who were either responsible for implementing immunization programmes or may be expected to give advice on this to orthodox Jewish mothers. These included five outreach workers with specific links to the community (e.g. responsible for support in areas including nutrition, mental health, family support and baby clinic); one health visitor; one GP, one Practice Manager; one Practice Nurse; and one receptionist. Members of the research team also met with local Rabbis and discussed the study with GPs and health related community workers to secure approval from religious leaders and to develop a culturally appropriate research design. Ethical approval was awarded by the North East London and The City Research Ethics Sub Committee and the Ethics Committee for the London School of Hygiene and Tropical Medicine. Off Site Hazard and Risk Assessments were completed for the interviewers at the London School of Hygiene and Tropical Medicine.
Interview protocol.
Transcripts were read and discussed by members of the team, who marked key passages according to analytical themes. Researchers used some of the principles of grounded theory, developing analytical constructs which were then applied in an iterative manner across the sample allowing us to confirm, reject or modify concepts during the study. 20 Responses to key questions were thus cross-tabulated and commonalities and differences were highlighted across all participants and for each immunization (BCG, MMR and DTP [diphtheria, tetanus and pertussis/polio]). This was designed to reflect the complexity of decision making, since it was found that most participants did not statically occupy a ‘pro’ or ‘anti’ position on immunization, varying their views over time and in relation to each kind of immunization. Deviant cases were particularly sought out in order to explore the factors which influenced those participants who did not adhere to community norms. No new themes emerged after analysis of 25 transcripts, which suggests that theoretical saturation had been reached. 21
Results
Only one participant had fully immunized all four of her children. The rest indicated
that they perceived BCG to be unnecessary, or that they were undecided about the
advisability of MMR or the whooping cough element of DTP, or that they would be less
likely to immunize their younger children than they had been for the older ones. The
difficulty of taking children along to clinics was not raised spontaneously by mothers.
Mothers were also asked about their perceptions of local health care services. Negative
perceptions were highlighted mainly in relation to restricted practice opening times or
having to rearrange appointments because of a sick child. About half of the mothers (13
of 25) said they felt neutral about the local services or thought they were ‘fine’; one
wanted to change her GP for personal reasons. Criticisms focused on lengthy waiting
times (6 of 25) or complementary medicine being unavailable (4 of 25) rather than staff
insensitivity. Just one respondent mentioned that staff could be more culturally aware
‘I just feel that maybe some health visitors should be taught more about
Jewish people… make them more aware that we're not offish, we're just very
busy.’ (participant 18)
Health professionals were sometimes praised for their sensitive and supportive role:
‘I have a good relationship with my health visitor who is a blessing. You
know ‘cause I suffer from manic depression after childbirth so she keeps on
visiting me. She's ever so nice, she's really helped me. She does more than her
job. She spends a lot of time with me and I appreciate it.’
(participant 2)
Social networks and media influence
Informal networks
‘There is always an anxiety… maybe through bad publicity. You hear little bits of information here and there and it plays on your mind… You know “why didn't Tony Blair give his last one the immunization?”’(participant 8)
‘This [child] hasn't had the MMR yet, the youngest, because of all the scares. The other two [children] had everything.’ (participant 18)
‘I'm hearing so many different things about [the MMR] that I just don't know… there's so much about autism and all these horrible things and measles, mumps and rubella aren't really deathly diseases. I'm kind of leaning towards not doing it.’ (participant 16)
‘Some people have told me that they have caught cancer, I don't know if that is true or not, they say from the immunization of MMR.’ (participant 12)
Safety
Perceptions of BCG
Danger
Adverse effects of immunizations (MMR and pertussis)
‘In my head it's like this. I have a healthy child and an immunization is a disease. I am putting the disease in the child. Who knows how good this immunization is? You know all the stories about immunizations and there are bad batches.’ (participant 17)
‘(The belief is that) with immunization you have a healthy child and then you're injecting a foreign something that could change that child. That's what happens with the immunizations. With the other health issues, exercise and… nothing's going to happen to them if they do exercise, or go swimming or… you know what I mean?’ (Key informant 1, outreach worker)
In the face of such threats, religiously inspired fatalism played an important part
in supporting a decision not to immunize:
‘When you don't know what to do, when there's a risk involved both
ways, then there's no need to put yourself in the danger of doing one of
them. By not doing it (we) trust that God will help you out of these
things.’ (participant 13)
‘I feel that if God wants her to get it [an illness] she will get
it.’ (participant 4)
Most participants (23 of 25), when asked what came to mind when they heard the term
‘MMR’, linked it with such fears. Two women, though, did not associate this with
anxiety and in fact perceived MMR as a routine immunization which they – and,
crucially, others in their social networks – gave to their children:
‘Nothing in particular (comes to mind). I knew I had to do it so I just
did it.’ (participant 2)
‘Everybody gives it. I've never really worried about (it). I'm happy to
give them. Why should (children) suffer basically? If there's something to
prevent that? That's basically my decision why I did it… All my friends went
and all my sisters (to the clinic for immunizations). It doesn't take long,
it doesn't cost any money and why not?’ (participant 1)
These two cases are important because they exemplify that different social norms exist within the same community. Social networks may therefore act as a support or deterrent to immunization for some women.
Discussion
Statement of principal findings
Low rates of immunization in the orthodox Jewish community we studied were not perceived to be due to practical difficulties associated with large families, or to insensitive cultural practices of health care providers. In a community relatively insulated from direct media influence, word of mouth is nevertheless a potent source of rumours about vaccination dangers, whose origin may lie in media scares. Combined with religious fatalism and a more generalized concern about the potential for harm done to the community from outside influence, such rumours succeed in raising vaccination anxieties to high levels. At the same time, the factor of community cohesion (and perhaps religious security) may also explain the relative safety felt in relation to tuberculosis. Paradoxically, in this case feelings of safety led to low BCG immunization rates, as found by other investigators. 22
The study identified that individuals in this community have a range of views on these matters. Changes in attitudes over time appear to have occurred, with many families having partially immunized their children, perhaps holding back with younger ones in the light of currently raised levels of anxiety. Additionally, the two cases where women not only immunized their children routinely but also believed that others in their immediate networks did so are of particular interest. Such variability suggests that efforts by local health care providers to influence members of the community, perhaps by feeding positive stories of the benefits of immunization into the informal system for circulating rumour, may be influential.
Strengths and weaknesses of the study
Our sampling from this difficult-to-reach population may be more likely to contain individuals open to contact with ‘outsiders’, something that may be associated with a greater willingness to immunize. In the light of this, the finding that anxieties about MMR were so common is all the more remarkable. The explanations provided by these interviewees for their own behaviour are likely to be helpful in understanding the views of others in the community who did not participate in the study. We were also unable to access those who do not receive Western medicine due to our recruitment from general practices. This is a problem which has been noted in other studies of ethnic minority groups and health beliefs, 23 although recent studies have suggested that complementary medicine is not necessarily considered to be an alternative to immunization. 24
Implications for clinicians and policy makers
Our findings suggest that it is important to monitor the views and practices of this community over time as these do not remain static. In turn, a better understanding of how and why they change will provide beneficial leads in identifying how health providers may make culturally sensitive interventions. It may be possible to challenge community norms by explicitly using its existing social networks to communicate more positive messages about immunization, though it is important to recognize that this group have information networks that span several countries, including the USA and Israel. During the period May to 18 July 2007 there were a total of 39 cases of measles in Hackney, most of these involving children from the orthodox Jewish community. 24 Outbreaks of measles in orthodox Jewish communities in Jerusalem were most likely to involve unvaccinated children, prompting calls for special attention to specific sub-populations. 25 Investigations of how different socially situated groups receive and process health information will yield benefits for minority communities and the wider population.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
We would like to thank all of those who agreed to take part in the study. Thanks to Tamar Sutton who was involved in the initial study design and conducted some of the interviews and thanks to Clive Seale for comments on an earlier version of the paper