
Abstract
Summary
Three cases of laryngopharyngeal primary squamous cell carcinoma presenting with thyroid nodules are described. The key message to take away from these cases is that patients with advanced malignancy of the upper aerodigestive tract can present with a thyroid nodule.
Case series
Case 1
An 83-year-old woman presented with a six-month history of progressive dysphagia, hoarseness, weight loss and a left-sided neck lump. Examination revealed a hard thyroid mass moving on swallowing. Ultra-sound scan confirmed a 2 cm mass in the left thyroid lobe. Fine needle aspiration cytology (FNAC) showed metastatic squamous cell carcinoma. Barium swallow and subsequent pharyngoscopy under general anaesthesia showed a malignant stricture of the cervical oesophagus. Palliative radiotherapy was declined by the patient, who died two months later.
Case 2
A 60-year-old woman presented with a six-week history of a right-sided neck lump, dysphagia, hoarseness, weight loss and aspiration when drinking. On examination, there was a right lower neck mass and right vocal cord palsy. FNAC was non-diagnostic. An MRI scan showed a mass arising in the right lobe of thyroid encasing the carotid sheath and brachiocephalic artery (Figure 1). Open biopsy of the mass showed moderately differentiated squamous cell carcinoma. Endoscopy under general anaesthesia showed a small supraglottic carcinoma. Palliative chemotherapy was declined and the patient died six weeks later.
Case 3
The family of the third case, that of a small supraglottic cancer metastasising to the thyroid, would not give consent to publication of further clinical details.
Discussion
Palpable thyroid nodules are common and the majority are benign. It is estimated that of the population of England and Wales, 3 million (5%) have a palpable thyroid goiter, 1 with 1500 new cases of thyroid cancer being diagnosed each year. 2 Careful clinical assessment, ultrasonography, FNAC and sometimes diagnostic hemithyroidectomy help identify those patients with thyroid carcinoma. It is also important to identify the even smaller number of patients who present with a thyroid nodule due to a metastasis, 3 since such patients usually have advanced malignant disease. Thyroidectomy in such patients is likely to be difficult and carry increased risks of complications. The procedure would be of questionable therapeutic value and, more importantly, may lead to a delay in diagnosis of the primary disease.
T1 weighted non-contrast axial MRI showing heterogeneous thyroid mass encasing bracheocephalic and carotid arteries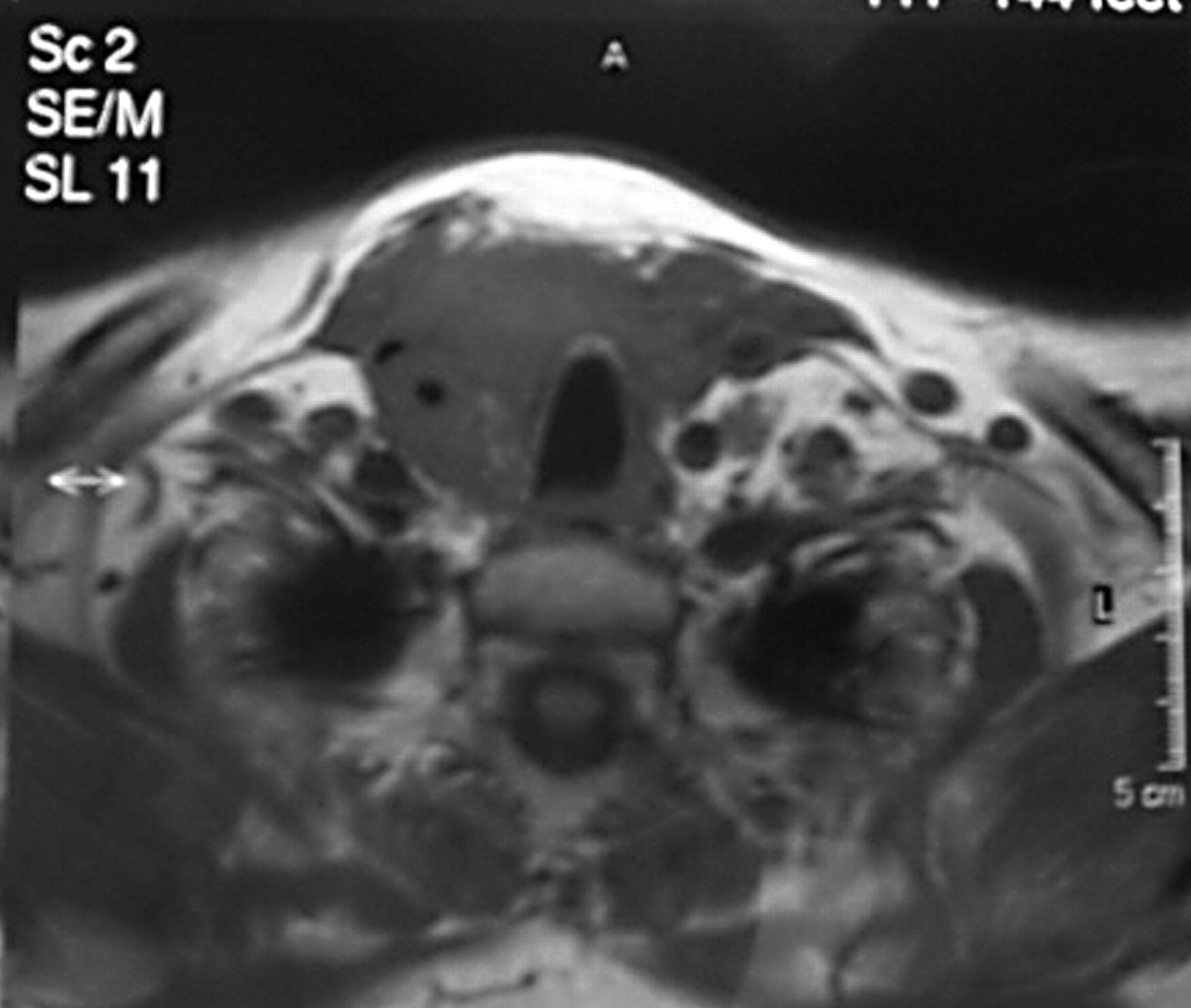
The majority of metastatic thyroid carcinomas are diagnosed after detection of the primary source, but between 5 and 36% present as the primary lesion. 4 , 5 Clinically, the presentation of secondary thyroid malignancies is similar to that of primary thyroid pathology, namely with symptoms of a thyroid lump, dysphagia, dysphonia and weight loss. 5 , 6 In a retrospective study of 43 patients with metastasis to the thyroid gland performed, 42% presented with a firm, painless thyroid mass. 6
The most common primary sources of metastatic thyroid nodules presenting clinically are extracervical, namely renal cell carcinoma, adenocarcinoma of the lung, breast and skin, and gastrointestinal cancer. 3 , 6 , 7 At autopsy, the most common primary sources are breast (26%), and lung (25%), melanomas (11%) and renal cell carcinomas (10%). 3 Metastasis to the thyroid gland is associated with a very poor prognosis, with mean survival time ranging from two weeks to three months. 4 , 6 In our series, it is clear that thyroidectomy would not have been advantageous to any of the patients, though aggressive treatment with surgical resection has a place in certain cases. 7
Key message
Patients with advanced malignancy of the upper aerodigestive tract can present with a thyroid nodule.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
None