
Abstract
Summary
This review is based on Pubmed, Medline and Internet literature searches, supplemented by knowledge from textbooks, conference presentations, and personal communications with experts in the field of hearing restoration and patients. We have not specifically selected a time limit for our literature searches; however, the majority are articles from the past 5 years.
Introduction
In the UK there are approximately nine million people with hearing impairments, and a further 28 million in the USA 1 , 2 , 3 More than half of these individuals are over the age of sixty-five. 4 With the world's population ageing, the already substantial but somewhat hidden social and financial burdens of hearing loss seem likely to increase. Significant advances in a variety of devices, from conventional hearing aids to auditory neural prostheses, are enabling hearing restoration with improved cosmesis and enhanced sound quality. Recent developments in genetics, the understanding of hair cell degeneration, and auditory neural pathways, have paved the way for promising research into novel regenerative therapies. Despite vast technological developments, utilization of devices remains low; of the two million people in the UK owning hearing aids, only one and a quarter million use them regularly. Furthermore, it is estimated that another four million people experiencing significant hearing impairments have not obtained an aid. With the myth of the iconic bulky hearing aid still prevailing, the cost-effectiveness and notable quality of life improvements provided by hearing restoration appear to pass unnoticed. This review will explore some of the major advances in this field, and will attempt to predict the future for hearing restorative techniques.
The complexity of deafness
The audiogram is the conventional clinical assessment of hearing loss measured in ‘decibels hearing level’ (dBHL). The threshold, the minimal audible level of a tone for a normal hearing listener, is under 25dBHL across all frequencies. Higher thresholds imply hearing loss, classified into mild (25–39dBHL), moderate (40–69dBHL), severe (70–94dBHL) and profound (≥95dBHL).
There are many causes of hearing loss. The majority are due to deficits within the cochlea or central auditory pathways, termed sensorineural hearing loss (SNHL), and can range from mild to profound. Anything that restricts the transmission of sound from the outer ear to the cochlea is termed conductive hearing loss (CHL). This usually causes a mild or moderate hearing impairment. The multiple deficits that hearing loss encompasses require complex amplification and sound conduction strategies to correct. 5 For example, poor pitch discrimination, which includes difficulty in separating sounds of a similar frequency, can result from the loss of cochlear hair cells. This, in turn, can contribute to difficulty in differentiating speech from background noise, especially if both are composed of similar frequencies. SNHL can also reduce the ‘dynamic range’ or the normal difference in threshold of sounds that are justaudible from those that are uncomfortably loud. Simply increasing the loudness of all sounds is therefore an unsatisfactory treatment strategy for the majority of patients. It is the ever-improving technical capabilities of newer devices, particularly in the separation and selective amplification of i) speech from background noise, and ii) faint sounds more than intense sounds, that have significantly increased their ability to truly aid hearing.
Conventional air-conduction hearing aids: from analogue to digital
These are aimed at patients with mild to severe hearing loss, and incorporate a microphone that converts sounds into electrical signals, returned to the ear as amplified sounds.
5
The prominent ear moulds of the ‘behind-the-ear’ devices have reduced in size, and have been joined by a range of more discreet ‘in-the-ear’ and ‘in-the-canal’ devices ( Conventional air conduction hearing aids: in-the-canal (A), in-the-ear (B) and behind-the-ear (C) devices. Reproduced with permission from Oticon UK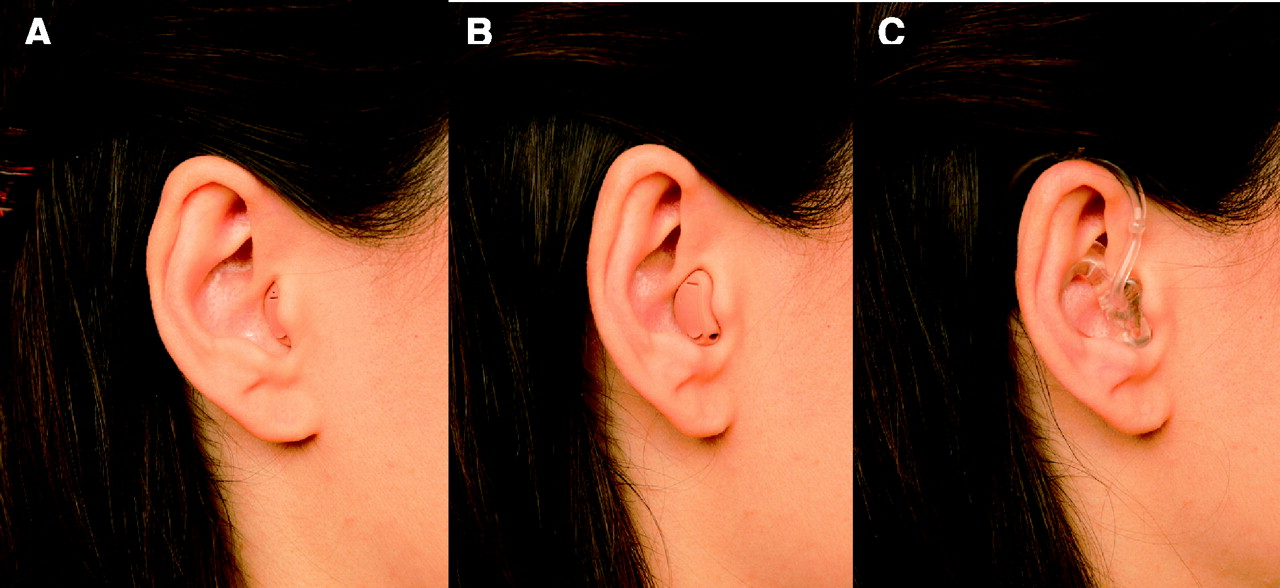
Directional microphones and induction loops: from mouth to ear
Directional microphones have been recently introduced, allowing speech from one direction to be preferentially amplified over the surrounding background noise. 9 Triple-microphone aids are being developed to further this concept. 10 These are replacing the omni-directional microphones that collect sounds regardless of source location. Induction loops, telecoils and, less commonly, frequency modulation (FM) systems can convert a speaker's voice directly into magnetic, electrical or FM signals that can be received with more clarity by hearing aid users. With obvious benefits, these have become increasingly commonplace in public places and on telephones.
Bone-anchored hearing devices
These devices are predominantly used in individuals who experience difficulty wearing a conventional air-conduction aid with an ear mould, due to recurrent ear infections. However, the indications have recently extended to individuals with single-sided deafness (SSD). The ‘Bone-Anchored Hearing Aid’ (BAHA™) incorporates a titanium plate that is surgically anchored to the skull on the hearing-impaired side, to directly simulate the inner ear by conducting sound vibrations through the bone. This allows for hearing from both sides of the head and overcomes the acoustic shadow cast by the head. Although the BAHA™ cannot fully restore directional hearing to individuals with profound SSD, it has been shown to significantly improve speech detection in noise and quality of life, particularly when compared to alternative devices such as ‘Contralateral Routing Of Sound’ (CROS) aids. 11–13 CROS aids utilize bilateral conventional aids, with a microphone at the impaired ear conveying information to the functioning ear, either by wire or wireless technology (e.g. FM or Bluetooth). These aids, perhaps due to the earlier inconvenience of connection wires, have never achieved widespread use. Conversely, with over 15,000 users worldwide, the BAHA™ is a well-established system. 14 The BAHA Intenso™ is a recent addition to the range of available sound processors, which aims to compensate for a mild SNHL in the better hearing ear. If it gains approval for this use, it would expand the clinical indications for bone-anchored hearing devices.
Implantable middle ear devices
A diagram of an ear with a middle-ear implant. Reproduced with permission from MED-EL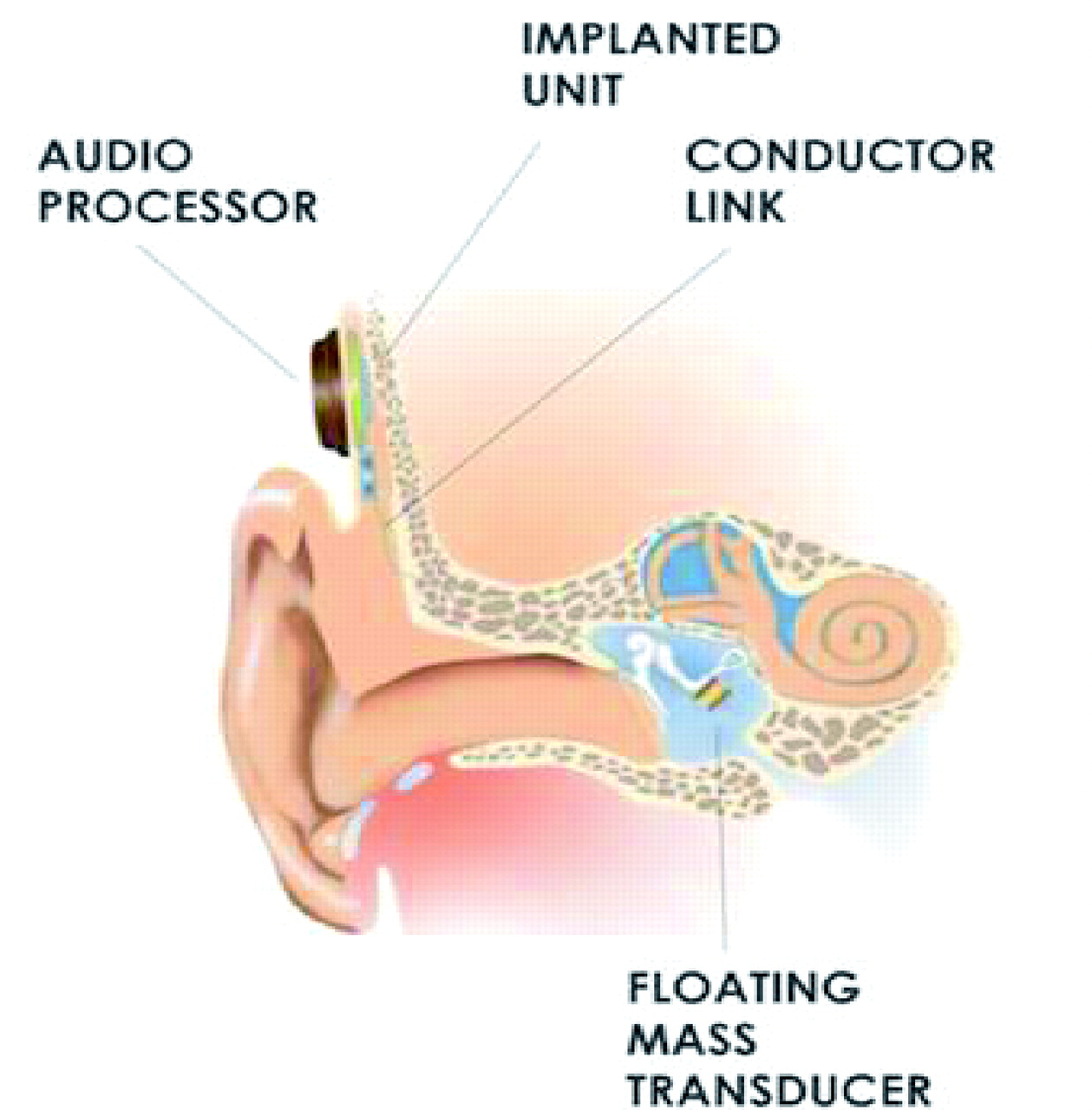
Cochlear implants
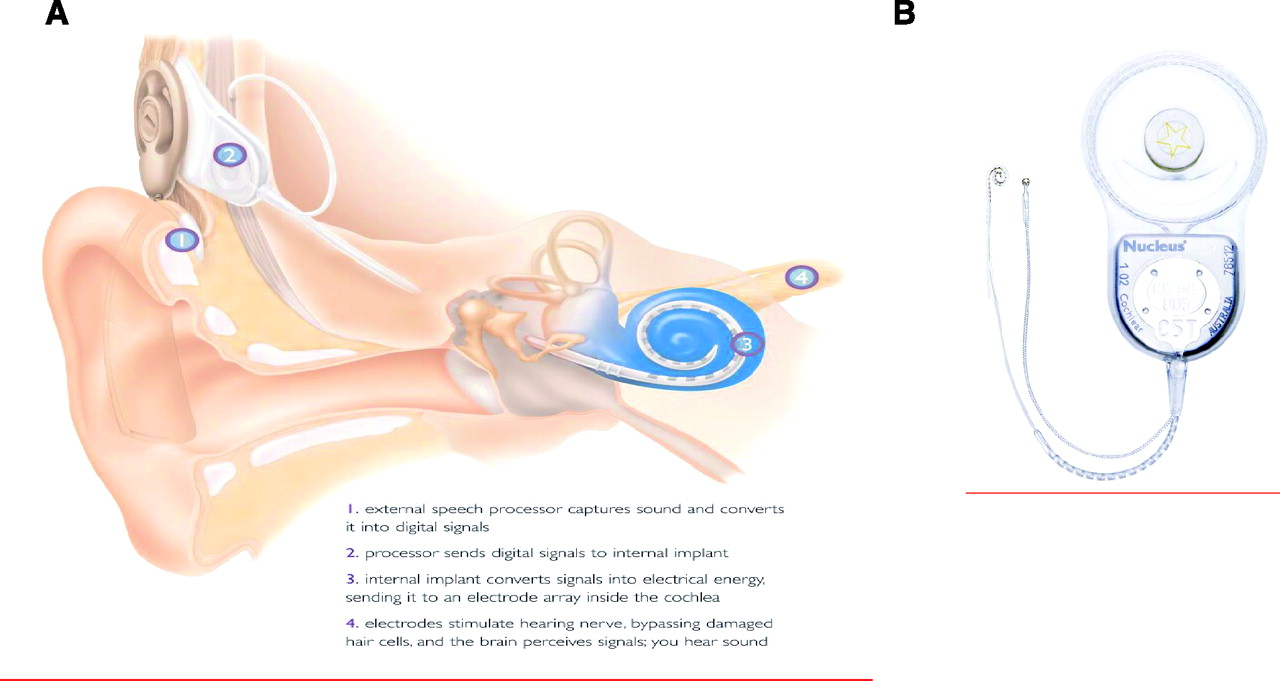
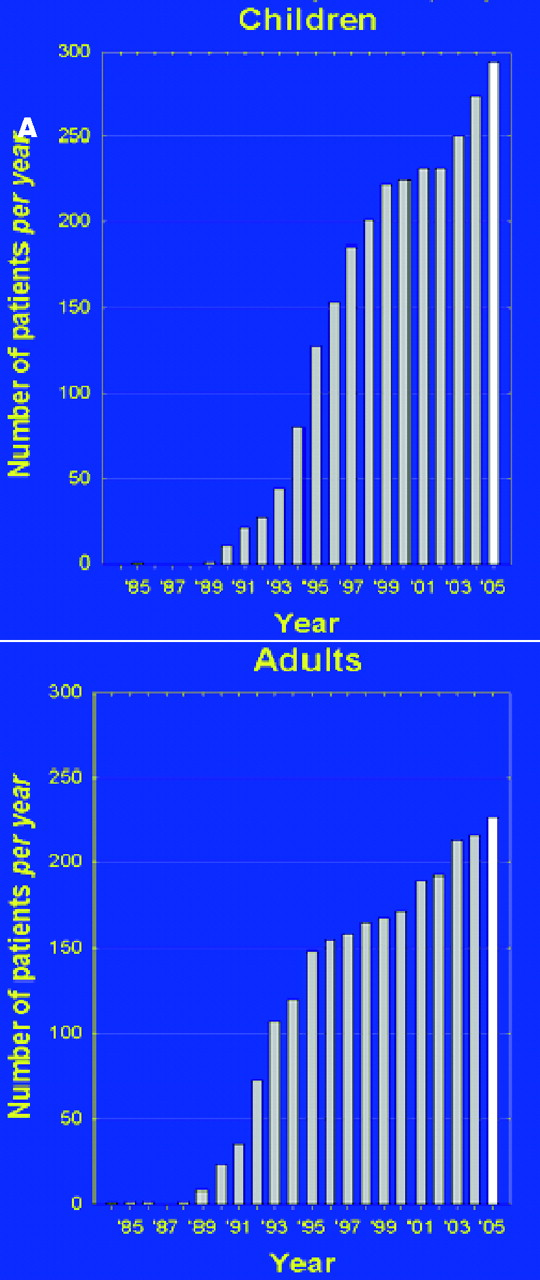
A diagram of an ear with a cochlear implant (A) and a photograph of the surgically-implantable components of a device (B). Reproduced with permission from Cochlear AG Numbers of children (A) and adults (B) receiving cochlear implants per year, in the UK. Reproduced with permission from Professor Quentin Summerfield
19
Until recently, the mainstay has been unilateral implantation. However, normally-hearing individuals use two ears to hear speech in noise and localize sounds effectively. For this reason, bilateral CI is being trialled worldwide. Although preliminary results are extremely encouraging, cost-benefit data is now required. 25 Compared with conventional ‘electric-only’ CI, evidence suggests that surgery aiming to preserve residual low-frequency acoustic hearing can benefit CI patients, with improved word recognition in noise and music appreciation. 26 Furthermore, the combined use of a CI in one ear and a hearing aid in the other may also yield improved speech recognition in noisy environments. 27
The recent introduction in the UK of the Universal Neonatal Hearing Screening program has enhanced the early detection of hearing loss amongst newborns. As delays in treatment worsen the degeneration of the disused auditory pathways, early intervention has been proven to provide maximal cost-effectiveness and quality of life improvement.
1
Early correction is particularly important for the 12,000 UK children born prelingually deaf, in whom the lack of early auditory input can restrict language development, a prerequisite for social interaction.
2
,
28
Likewise, long delays prior to implantation are associated with poor hearing outcomes amongst individuals who have experienced normal hearing before the onset of deafness.
29
As the developing auditory system is particularly sensitive to the effects of sensory deprivation, it seems imperative that children who acquire deafness after meningitis are assessed for CI without significant delay. Furthermore, the cost per quality-adjusted life year (QALY) benefits of CIs are enhanced when interventions are appropriately prioritized based upon duration and severity of deafness and preoperative performance with conventional aids. For example, those that have been deaf for >30years and already benefit from acoustic hearing aids may not benefit from a CI.
30
( M, now 4 years old, was noted to be a ‘very quiet’ baby. By 6 weeks of age, his parents were particularly concerned; subsequent audiological and evoked-brainstem response investigations confirmed bilateral profound SNHL, and genetic testing revealed a causative connexin 26 mutation. At the age of 18 months, M was surgically-implanted with a left sided Nucleus Contour™ with Soft-tip™ cochlear implant (Cochlear Ltd.). A month later, this was connected to a body-worn speech processor and was ‘switched-on’. He now wears his speech processor behind his left ear (Esprit 3G™, Cochlear Ltd.), which is regularly re-tuned by audiologists. He continues to wear a conventional hearing aid in his right ear. Although speech and language understanding were initially markedly delayed, within months M was speaking about 80 distinct words that his parents could understand. Being a very sociable and friendly child, M made excellent progress. Attending nursery, with support from a teacher of the deaf, provided a suitably stimulating environment. The use of small teaching groups and tailored learning environments has helped minimize the difficulties associated with excess background noise. With the help of classroom assistants and speech and language therapists, M has now attained receptive and expressive language skills that are comparable to his normally-hearing peers and he is looking forward to starting at his local mainstream school.Case study
Midbrain and brainstem implants
(A) diagram of an auditory brainstem implant, including surface and penetrating electrode arrays, and (B) photograph of the surgically-implantable components of a device. Reproduced with permission from House Ear Institute & Cochlear AG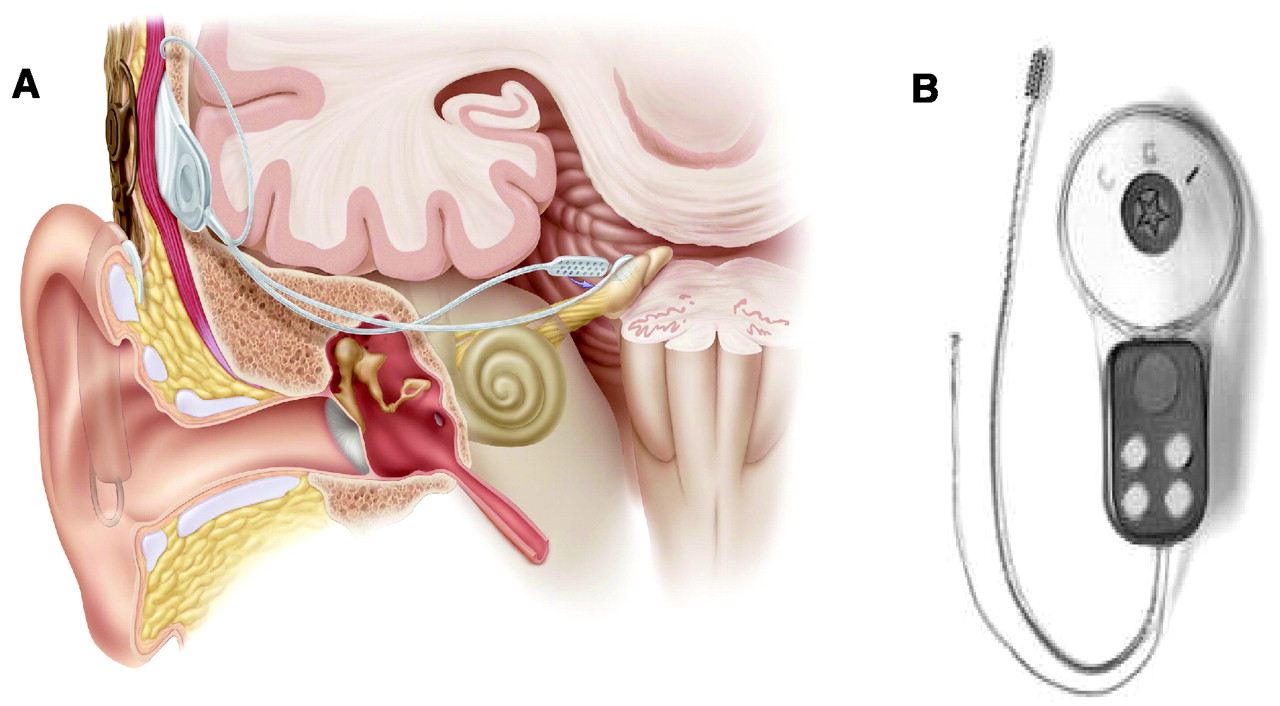
What are the economic implications of deafness?
Hearing restorative treatments undoubtedly improve quality of life; however, the seemingly high initial costs of fitting and maintenance may have restricted their use. In the UK, two and a half million hearing-impaired people are of working age (16 to 60 years). Considering lost productivity, provision of special education and medical care, the economic costs of untreated deafness and hearing loss are estimated to be as much as €92 billion and $56 billion per annum in Europe and the USA, respectively.
2
Given that the cost of gaining a QALY is lowest for those treated both at a younger age and sooner following deafness, the overall financial benefits of restorative treatments are significant for healthcare services and employers alike.
1
,
33
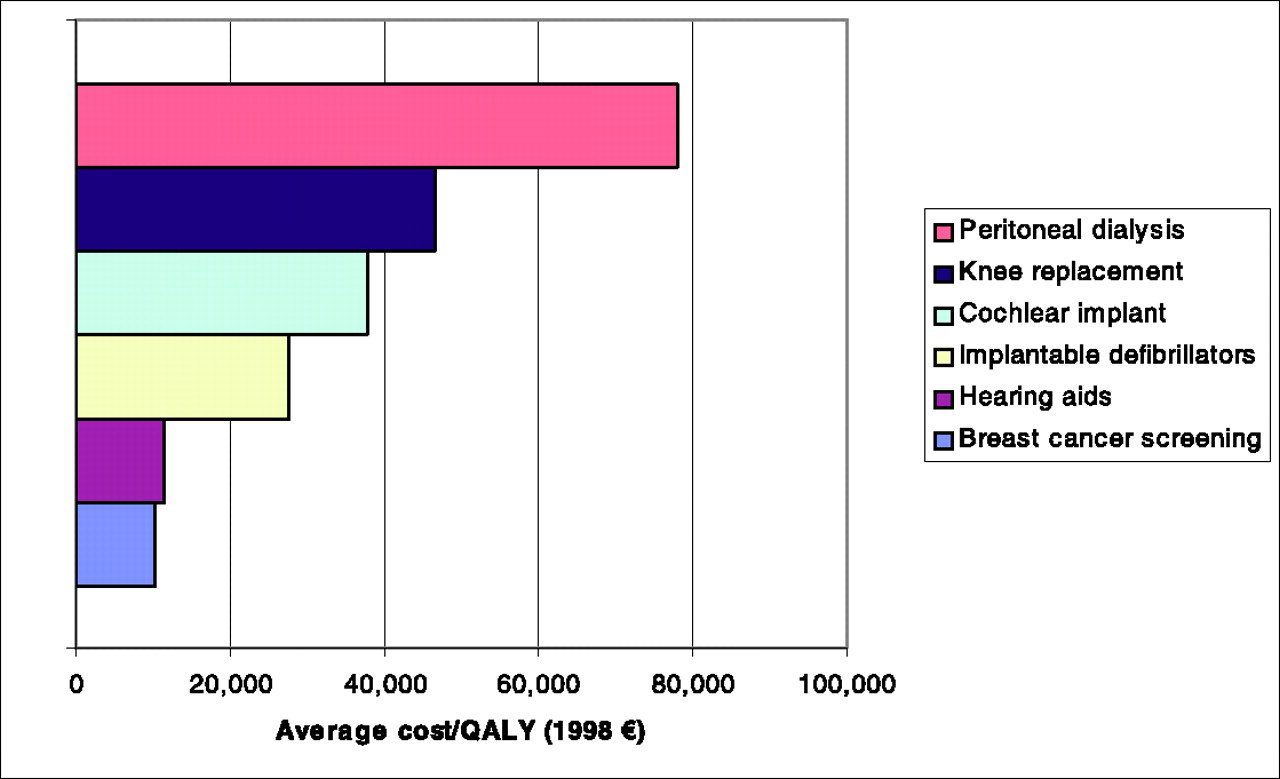
For example, the lifetime costs per QALY reveal that CIs are a cost-effective intervention in the majority of patients, irrespective of age (average cost per QALY is £27,142).
30
The figures are even more impressive when implantation is limited to those patients with profound deafness that fulfil more stringent selection criteria for benefit. Similarly, hearing aids are highly cost-effective in all age groups, with a QALY similar to that for breast cancer screening
2
,
33
(
Future: what is the next step?
Arguably, the greatest developments in the field of hearing restoration, to date, have been technological. Smaller, more discreet electronics, with increasingly sophisticated speech processing, noise reduction and wireless communication, have all improved the function, appearance and customized programmability of devices. 10 Even so, our ever increasing understanding of the structure and function of the auditory system, from the genetics of cochlear hair cell development to adaptation within the brain following hearing loss, 34 is showing great promise for producing novel treatment strategies for the future. The challenge to the field of hearing restoration is no longer to provide deaf individuals with a basic percept of hearing: through a broad range of existing interventions this is already widely attainable. Instead, hearing therapies must aim to restore ‘normal listening abilities’, such as hearing speech in noisy environments and the ability to localize sounds, which current devices seldom consistently provide.
Although CIs have already been incredibly successful worldwide, it is likely that the future will yield more sophisticated programming of bilateral implants in order to fine tune them for different listening environments. 25 Middle ear implants also have a promising future, particularly if their amplification of high-frequency sounds and their reliability can be improved to match that of CIs. Optimally, operative times for middle ear and cochlear implants, both currently at 3–5 hours for bilateral implantation, need to be refined. Furthermore, the development of totally implantable cochlear implants (e.g. TIKI, Cochlear Corporation's experimental program) and middle ear devices are likely to be advantageous due to improved cosmesis and lower risks of equipment damage. 15 Whilst most patients retain adequate auditory nerve cells for CIs to function, studies suggest more complex stimulation CI strategies (for example, the use of more channels) may require greater neuronal function for optimal outcomes post-implantation. 35 , 36 Indeed a problem associated with hair cell death is the inactivity-related degeneration of the spiral ganglion neurones (SGNs) that innervate the hair cells. A solution may be to incorporate drug delivery systems into the electrode design and, subsequently, to release neurotrophic factors into the cochlea to preserve or even regenerate spiral ganglion neurones following hair cell loss. 37 Two factors in particular, brain derived neurotrophic factor (BDNF) and neurotrophin-3 (NT3), have been identified as being vital for the survival of auditory and vestibular neurons. 38
Although birds are capable of regenerating cochlear hair cells, this is unfortunately not a feature available in humans. Ageing, noise, infections and ototoxic drugs are now known to trigger hair cell degradation, and subsequently SNHL, through a common pathway involving the caspase proteases.
39
In the UK, Audiology Departments often accept direct referrals from General Practitioners for adult hearing aid provision, provided the following criteria are met: Individual over 60 years of age No tinnitus No sudden onset or sudden deterioration of hearing loss No unilateral or asymmetrical hearing loss No earache or discharge No wax obscuring the view of the tympanic membrane No vertigo, other than that associated with old age If any of these criteria are not matched, an individual with hearing loss may be referred to an alternative specialist: usually an Ear, Nose & Throat Surgeon/Otologist, Audiological Physician or Community Paediatric Audiologist, as appropriate. British Cochlear Implant Group: www.bcig.org
MRC-Institute of Hearing Research: http://www.ihr.mrc.ac.uk/profile/
The British Deaf Association: www.britishdeafassociation.org.uk
The National Deaf Children's Society: www.ndcs.org.uk
The Royal National Institute for Deaf People: www.rnid.org.uk
Deafness research UK: www.deafnessresearch.org.uk
Specialist referral criteria
Further resources
Due to the anatomical and neurophysiological complexity of the central auditory system, the mechanisms underlying the encoding of speech and other sound signals in the brain are areas in which more gradual progress has been made. Research into these fundamental areas, as well as artificial intelligence and the development of neuronal networks of signal processing, may yield clues towards rebuilding or even replacing parts of the central auditory pathways. 10 The compensatory adaptation of the brain to prolonged deafness and the plasticity of the central auditory system to restoration of peripheral hearing is a key research area under active investigation. 20 , 42
In summary, hearing therapies are cost-effective and provide a significant improvement in patients' quality of life. 33 Biomedical science has made some encouraging early advances in the ultimate quest for a therapeutic agent to prevent or reverse cochlear damage. However, at this time, even the most optimistic observer would expect to wait at least a number of decades for such a cure. Therefore, clinical therapies for hearing loss largely remain focused upon the physical amplification of sound. As significant advances have been made in this field, appropriate device selection for individual patients is paramount, and the psychological implications of hearing loss and its subsequent treatment need to be considered as part of routine management. Further comparative evaluations are required of the outcomes of the various devices, using standardized tools to highlight reasons for dissatisfaction, non-compliance or dropout amongst patients. Hearing impairment may be considered by many to be a disability, but it does not have to be a handicap.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
The authors are grateful to Prof AJ King for his comments on an earlier version of this manuscript, and to Mr I Johnson for his insightful review of this paper. This work was supported by The Wellcome Trust & the Sir Peter Morris Surgeon ScientistProgramme, Nuffield Department of Surgery, Oxford University