
Abstract
In South Asian countries, conventional vascular risk factors like hypertension, diabetes mellitus, cardiac disease, smoking, obesity, atrial fibrillation are the dominant ones, while other aetiologies like rheumatic heart disease, infective meningitis-related infarcts and postpartum cerebral venous thrombosis also constitute a big fraction. This review discusses the evidence of prevalence of various risk factors in South Asian countries and possible measures to combat the rising burden of cerebrovascular disease. The last part of the review discusses prevention and identification of risk factors that are unique to or especially found in patient population of South Asia.
Declarations
Risk factors for stroke among Indian population
Stroke is aetiologically more heterogeneous than ischaemic heart disease (IHD). While IHD is practically always a result of atherothrombotic process, stroke in a significant proportion of cases results from lipohyalonosis or arteriolosclerosis (haemorrhagic stroke; lacunar infarctions), venous thrombosis and cerebral aneurysms, although atherothrombosis probably accounts for a majority of cases. Risk factor studies and preventive strategies for these different aetiological subtypes of stroke require different approaches. Lumping them together may mask the role of certain risk factors in the aetiology of stroke. For example, high cholesterol is a risk factor for ischaemic stroke, but low cholesterol appears to be a risk factor for haemorrhagic stroke. 1 If risk factor studies do not analyse the two types of stroke separately, the role of cholesterol as a risk factor may be underestimated.
Causes of and the risk factors for stroke in South Asia may bear many similarities with those in developed countries, but some causes like rheumatic heart disease and postpartum cerebral venous thrombosis, which are unusual in developed countries, are still common in South Asia. The risk factors for atherothrombotic vascular disease appear very similar, but there have been few methodologically rigorous examination of all potential risk factors in stroke in India. No prospective population-based cohort study has been reported from India.
Case-control studies are usually conducted to determine risk factors of a disease but are associated with multiple sources of bias. Ideally, a community-based study with all incident cases of stroke should be compared with a random sample of age and sex-matched or unmatched controls from the ‘healthy’ population. Even with the best precautions to obtain the measurements by blinded observers (impossible for some variables like body mass index [BMI]), the possibility of stroke affecting the variables and recall bias cannot be ruled out. This is why the risk factors with borderline association (odds ratio [OR], <3) are not considered to be established or important. From primary and primordial prevention point of view, the studies should study only first strokes.
There has been no such community-based case-control study of risk factors for stroke. Hospital-based studies are associated with varying degrees of survivor bias and referral bias. With this caveat in mind, the following points about risk factors for stroke can be made:
The risk factors for ischaemic stroke and coronary artery disease are similar;
The risk factors for both ischaemic and haemorrhagic stroke in India are similar to those in other countries;
Non-modifiable risk factors are age, sex, race, low birth weight and genetic factors.
Modifiable risk factors for ischaemic stroke include hypertension, smoking, diabetes, high cholesterol, heart disease including atrial fibrillation, obesity, past history of transient ischaemic attack (TIA), carotid or intracranial arterial stenosis and reduced consumption of fruits and vegetables. For haemorrhagic stroke, hypertension, smoking, alcohol consumption and probably low cholesterol are risk factors. For cerebral venous thrombosis in the postpartum period, the risk factors are largely unknown, though low socioeconomic status, anaemia, malnutrition and dehydration appear to be common risk factors.
’Young’ individuals may develop stroke due to a variety of other risk factors that are seen rarely and probably worldwide, for example, arterial dissection, connective tissue diseases, vasculitides, Moyamoya syndrome, migraine haematological disorders, substance abuse, mitochondrial cytopathy and rare genetic conditions. The following paragraphs from Warlow et al. 2 seem pertinent to quote in this context: 2 ‘There is nothing very different about the young compared with the elderly ischaemic stroke or transient ischaemic patient. The range of causes is similar. However, under the age of 40 years neither thromboembolism nor “complex” small vessel disease are at all likely, although not impossible, whereas over the age of 60 years these disorders become overwhelmingly more likely than anything other than embolism from the heart. Young patients attract more than their share of attention and tend to get more intensively investigated, which is not unreasonable because the proportion with an unusual (and often treatable) cause is undoubtedly higher than in the elderly. Innumerable series of “young stroke patients”, meaning anything from younger than 30 years to less than 50 years, probably depending on the age of the author, have been reported. The mix of causes and proportion with “no cause” depend on referral bias; investigation intensity; diagnostic criteria differences and fashion over time; all these can change as more putative causes are discovered.’
Stroke in Bangladesh
Risk factor studies
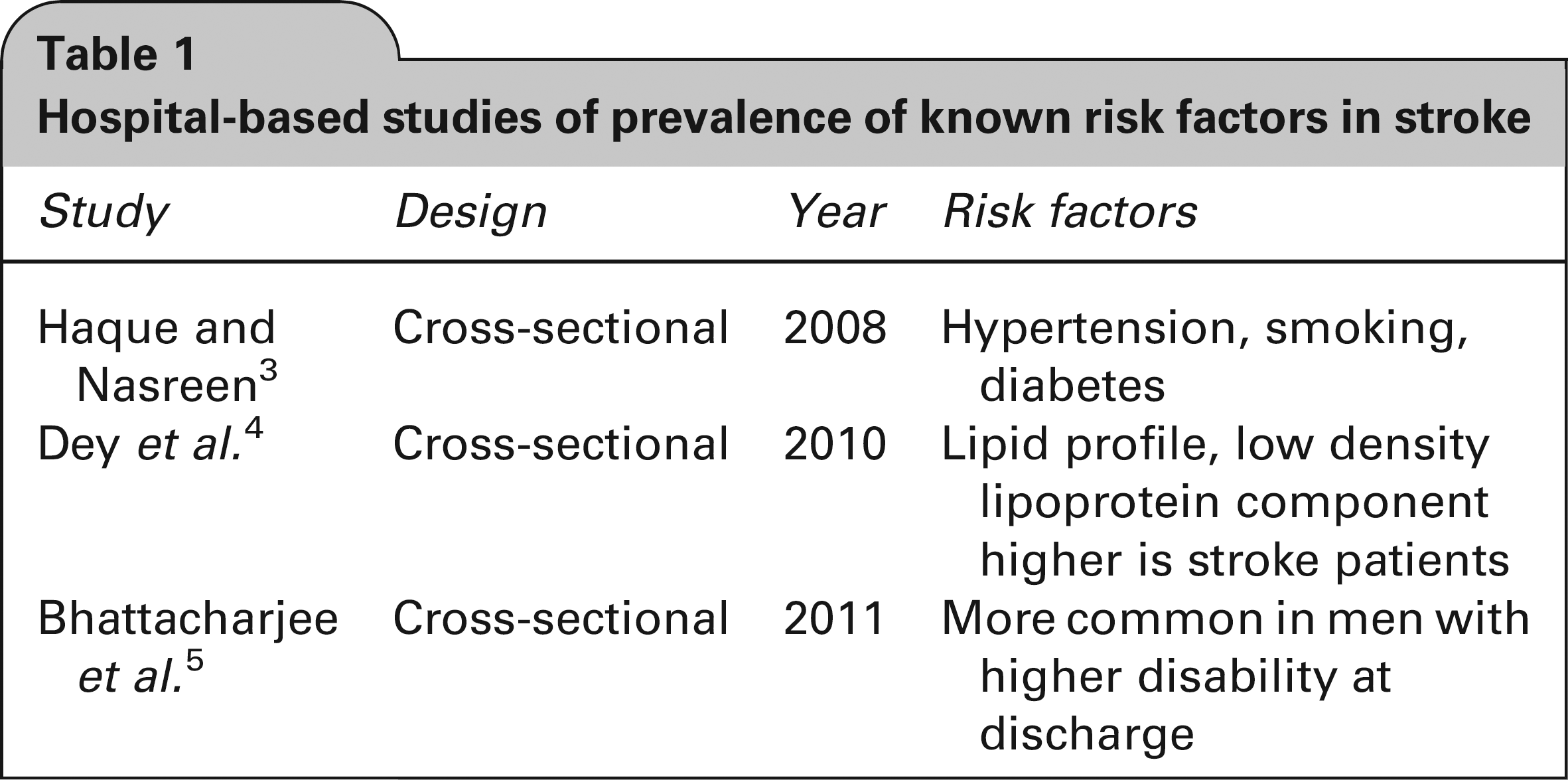
Conventional risk factors for stroke, like hypertension, diabetes mellitus, ischaemic heart disease, atrial fibrillation and dyslipidaemia, smoking, male gender and previous stroke, have been seen in hospital-based studies conducted in this area of South Asia in single centre3–5 or multicentre studies6,7 which have mainly looked at coronary heart disease risk factors.
The hospital-based studies were cross sectional in design and included small numbers of stroke patients (48 and 177 in two studies). They gave a simplistic description of the demographic patterns and conventional risk factor occurrences as mentioned in Table 1.
Hospital-based studies of prevalence of known risk factors in stroke
Other vascular risk factors that have been studied in the Bangladesh population are waist-to-height ratio, 8 Apolipoprotein E 9 and increased FVII levels. 10 The study by Sayeed et al. 8 was a cluster sampling of rural inhabitants (5713 found eligible) and found that waist-to-height ratio is a better obesity index than BMI and waist-to-hip ratio for predicting diabetes, hypertension and lipidemia. This study did not look at the occurrence of stroke in this population. The study by Chowdhury et al. 9 was a case-control study of 227 cases and 190 controls. It suggested that both apoE epsilon3/epsilon4 genotype and epsilon4 were risk factors for cerebral thrombosis in the cortical artery region, whereas epsilon 2 was a risk factor for haemorrhagic stroke in the elderly. The study by Kain et al. 10 was conducted in West Yorkshire with subjects who were originally from India, Pakistan or Bangladesh. A total of 140 cases and 90 controls were studied. The results suggested that South Asian women have increased FVII levels and that women with a history of ischaemic stroke have a decreased fibrinolytic potential in comparison with men.
Another study conducted in Singapore among South Asians found that intracranial stenosis was more prevalent than extracranial stenosis. 11
Stroke in Nepal
Risk factors like smoking, hypertension, alcohol, atrial fibrillation and diabetes mellitus have been found in retrospective case series12–14 in Nepali patients (Table 2).
Prevalence of known risk factors of stroke in Nepal

Stroke in Pakistan
Risk factors
In a recent cross-sectional survey in an urban slum, 15 the odds of cerebrovascular events (CVEs) with a single risk factor ranged from 1.59 for diabetes to 2.23 for history of myocardial infarction. The range of odds for CVE with two risk factors was between 1.83 (hypertension and diabetes) and 2.37 (diabetes and obesity). However, the odds of having stroke are 2.15 times more in people who have two or more risk factors than those with only one risk factor. Odds were higher for CVE when more than two risk factors were combined. A combination of diabetes, hypertension and obesity predicted the odds for CVE to be 2.44, while the addition of a family history of CAD/stroke to this data-set increased the odds to 3.4. The highest odds were found to be in combination of hypertension, diabetes, obesity and cigarette smoking (OR, 4.9). Similar risk factors were found in an earlier study. 16 It found that the adjusted OR for stroke in adults aged 40 years or over in the Pashtun community in Karachi, Pakistan were significantly higher with extra salt in food, diabetes and increased systolic blood pressures. This study did not specifically look at obesity and history of myocardial infarction.
In a hospital-based retrospective audit of medical records, hypertension was the most common modifiable risk factor seen in 78.0%, followed by diabetes in 40.3% and dyslipidaemia in 31.5%. 17 This is similar to earlier studies18–21 (Table 3). In young stroke, common causes of stroke detected were infective meningitis (tuberculosis and bacterial) and hypertension (for haemorrhagic stroke), predominantly in men. Cardioembolism, pregnancy-induced hypertension and puerperal sepsis were other major causes. 23 In paediatric patients meningitis and encephalitis were found to be the most common aetiology. 22
Studies on prevalence of the known risk factors done in the last decade in Pakistan

Stroke in Sri Lanka
Risk factors
While conventional risk factors have been found to be prevalent in hospital-based studies in Sri Lanka,24,25 also in young stroke 26 uncommon causes of stroke like bites due to Russell's Viper (Daboia russelii) have been reported exclusively from Sri Lanka. 27
Vascular risk factors exclusive to South Asia
While major established cardiovascular risk factors like hypertension, smoking, hypercholesterolaemia and type 2 diabetes mellitus are also prevalent in South Asia, 15 a number of dietary habits like consumption of desi dalda and ghee as well as other forms of tobacco like hukkah, gutka and paan have not been studied. 28 Among emerging risk factors studied, South Asians have higher concentration of fibrinogen and plasminogen activator inhibitor-1 (PAI-1). 29
Inflammatory markers like high-sensitivity C-reactive protein (hs-CRP) have been found to be higher in South Asian populations, 30 although there are conflicting reports. 31 Elevated plasma homocysteine and Lipoprotein (a) have been seen in patients of South Asian ethnicity.32,33
Infections, peripartum sepsis and cardioembolic stroke as a result of rheumatic heart disease still remain the most common cause of stroke in young.23,34 While the prevalence of genetic factors is also being studied in this part of the world, 35 the main limitations are inadequate management of risk factors 36 and delay in bringing the patients to medical services.
How to solve the problem of stroke burden
The key to solving the problem of stroke is prevention. Even with the best and most developed health-care system, the treatment of stroke is not likely to significantly impact the burden due to stroke. For example, thrombolysis, even under the best circumstances, cannot reach more than 500–1000 of 1.6 million stroke cases estimated to occur in 2015. This is assuming that the number of centres practicing thrombolysis in India increases to 50 and each centre is able to carry out thrombolysis in 20 patients per year. Therefore, the axiom, ‘prevention is better than cure’ is very true for stroke.
Prevention
Approaches to stroke prevention involve actions to achieve primordial, primary, secondary and tertiary prevention. Primordial prevention of stroke refers to strategies designed to prevent or minimize the development of risk factors for stroke (e.g. smoking prevention and control). It is, essentially, primary prevention of risk factors. Primary prevention of stroke refers to the treatment of established risk factors in the population to prevent occurrence of first-ever stroke (e.g. treatment of hypertension, diabetes). Secondary prevention refers to the control of risk factors to prevent a recurrent stroke. Tertiary prevention refers to effective management of patients with established stroke with the aim of preventing disability arising from stroke.
Primordial prevention: Community-based programmes to increase physical activity, to improve nutrition and to prevent smoking and other tobacco use, comprehensive worksite wellness programmes, nutritional modifications and diabetes screening have all been shown to reduce the costs of health care and cardiovascular risk in population studies and should be implemented in both developed and developing countries. 37
Primary prevention: The risk factors that have to be addressed in South Asian countries for primary prevention are not very different from the conventional vascular risk factors prevalent in the developed nations, but the detection and prevention of stroke due to rheumatic heart disease, 38 postpartum state 39 and neuroinfections will greatly decrease the burden of disease due to treatable causes. Well-documented and modifiable risk factors include hypertension, exposure to cigarette smoke, diabetes, atrial fibrillation and certain other cardiac conditions, dyslipidaemia, carotid artery stenosis, sickle cell disease, post-menopausal hormone therapy, poor diet, physical inactivity and obesity and body fat distribution. Less well-documented or potentially modifiable risk factors include the metabolic syndrome, alcohol abuse, drug abuse, oral contraceptive use, sleep-disordered breathing, migraine headache, hyperhomocysteinemia, elevated lipoprotein(a), elevated lipoprotein-associated phospholipase, hyper-coagulability, inflammation and infection. 40
Secondary prevention: For the treatment of vascular risk factors in patients who have had a stroke, blood pressure reduction to optimum levels is recommended beyond the first 24 hours, besides glycemic and lipid control. 41 The selection of an antiplatelet agent should be individualized on the basis of patient risk factor profiles, cost, tolerance and other clinical characteristics. The addition of aspirin to clopidogrel increases risk of haemorrhage and is not recommended for routine secondary prevention after ischaemic stroke or TIA. These additions in the American Heart Association/American Stroke Association recommendations are especially applicable in developing countries where the economics of antiplatelet agent use have implications not only on the compliance but also preventing practitioners from using an alternate antiplatelet or combinations under the impression that they have better effectiveness. Anticoagulation should be started in every patient with atrial fibrillation (valvular or non-valvular unless contraindicated. Anticoagulation should be considered for all patients who have ischaemic stroke associated with mitral valve disease, prosthetic heart valves, or within three months of myocardial infarction. Anticoagulation should not be started until brain imaging has excluded haemorrhage and 14 days have passed from the onset of an ischaemic stroke (except when a demonstatic intracardiac thrombus is present). Anticoagulation should not be used after TIAs or minor strokes unless cardiac embolism is suspected. Any patient with a carotid artery territory stroke and minor or absent residual disability should be considered for carotid endarterectomy. Carotid ultrasound should be performed on all patients who would be considered for carotid endarterectomy. Carotid endarterectomy should only be undertaken by a specialist surgeon with a proven low complication rate, and only if the stenosis is measured at greater than 70%. 41 All patients should be assessed for other vascular risk factors and be treated or advised appropriately. All patients should be given appropriate advice on lifestyle factors (such as not smoking, regular exercise, diet, achieving a satisfactory weight, reducing the use of added salt). Therapy with a statin should be considered for all patients with history of TIA or ischaemic stroke and low density lipoprotein (LDL) cholesterol may be reduced 15–20% of the baseline value. Although all of these recommendations are from studies conducted in non-South Asian countries, they can very well be applied to South Asian nations. 42 Apart from this the contribution of poor nutrition in outcome after stroke 43 is also exclusive and needs focus in this part of the globe. Thus if we take into account the relative risk reduction associated with various evidence-based interventions for secondary prevention from published meta-analyses 44 and apply it to an Indian population of one million taking the reported prevalence of various risk factors, the number of strokes avoided per year with use of various interventions in descending order are as follows: blood pressure lowering by 10 mmHg (61), aspirin (23), aspirin and dypir-idamole (22), lowering of LDL cholesterol by 1 mmo1/L (19), smoking cessation (19), anticoagulants (15), glycated haemoglobin lowering by 0.9% (3) and carotid revascularization (3).
Tertiary prevention: This requires effective and evidence-based management of stroke according to published guidelines. 45 For example, early surgery in patients with intracerebral haemorrhage may prevent death and disabilities. Random assignment to decompressive hemicraniectomy within 48 hours of onset of the symptoms of malignant middle cerebral artery territory infarction is associated with a reduction in death or dependency from 76.5% (conservative) to 60.2% (surgery) (absolute risk reduction [ARR], 16.3%; 95% confidence interval, -0.1–33.1%). 9 If 2% (30) of the 1500 patients with acute ischaemic stroke had malignant middle cerebral infarction causing neurological deterioration that was treated by means of decompressive hemi-craniectomy, 11 the number of dead or dependent could be reduced by five (30 x 16.3% [ARR]), which is about 0.5% of all 1000 new cases of death and dependency. 46
Prevention of recurrence of intracerebral haemorrhage
Hypertension, if present, should be adequately controlled. Control of other risk factors for stroke like diabetes and smoking should also be emphasized. Saccular aneurysm needs to be treated by clipping or endovascular occlusion as in the case of subarachnoid haemorrhage. Arteriovenous malformation (AVM) should be treated by surgical excision, endovascular embolization or radiosurgery or a combination of the three depending on the site and size of the AVM. Vasculitis or other medical conditions require specific treatment to prevent recurrence of intracerebral haemorrhage.
Limitations of preventive strategies
Although the preventive strategies for all stroke types have been exhaustively studied worldwide, in South Asia, apart from the conventional preventable and non-preventable risk factor modification, what still needs to be explored are known and preventable factors exclusive to the socioeconomic, cultural, environmental and coexisting nutritional and infection-related factors here. What also needs to be addressed prospectively in studies here are whether there are any genetic predispositions to stroke among patients in South Asia.39,47,48
Footnotes
Acknowledgements
None