
Abstract
Overwhelming evidence exists that thrombus generation resulting from platelet activation and aggregation is the primary process involved in the occurrence of the myocardial infarction and stent thrombosis. Despite the proven clinical efficacy of dual antiplatelet therapy, wide antiplatelet response variability associated with clopidogrel therapy was demonstrated in pharmacodynamic studies where approximately one in three patients exhibited high on-treatment platelet reactivity (HPR). Generally, physicians do not objectively assess the intensity of the adenosine diphosphate–P2Y12 interaction in their high-risk patients treated with clopidogrel. Instead most clinicians use a non-selective or one-size-fits-all approach. HPR and CYP2C19 LoF carriage are associated with clinical outcomes in high-risk clopidogrel-treated patients who have undergone percutaneous coronary intervention (PCI). Although we do no yet have conclusive evidence from a large-scale randomized trial that personalized antiplatelet therapy improves patient outcomes, a class IIb recommendation has been given in the guidelines to perform genotyping or phenotyping in high-risk PCI patients if a change in antiplatelet therap will ensue based on the test results. It may be reasonable at this time to assess platelet function and perform genotyping in clopidogrel-treated high-risk patients and treat with more potent P2Y12 receptor therapy selectively.
Introduction
Overwhelming evidence indicates that thrombus generation resulting from platelet activation and aggregation is the primary process involved in the occurrence of the myocardial infarction (MI) and stent thrombosis. Despite the proven clinical efficacy of dual antiplatelet therapy (DAPT) of aspirin and clopidogrel, wide antiplatelet response variability associated with clopidogrel therapy was demonstrated in pharmacodynamic studies where approximately one in three patients exhibited high on-treatment platelet reactivity (HPR).1–3 A strong association between HPR and recurrent ischaemic event occurrence in percutaneous coronary intervention (PCI) patients has been demonstrated in observational studies of thousands of patients utilizing multiple ex vivo laboratory analyses. Despite the fundamental importance of unblocked P2Y12 receptors in the genesis of thrombosis and well-established limitations of clopidogrel, physicians generally do not objectively assess the intensity of the adenosine diphosphate (ADP)–P2Y12 interaction in their high-risk patients treated with clopidogrel. Instead most clinicians use a non-selective or one-size-fits-all approach.1–3 Indeed, this non-selective approach to clopidogrel therapy is paradoxical compared with the objective assessments and adjustments frequently made during treatment of cardiovascular disease patients with other drugs. Moreover, single-nucleotide polymorphisms (SNPs) of gene encoding enzymes associated with clopidogrel metabolism, particularly carriage of the CYP2C19 loss-of-function (LoF) allele, has been associated with higher post-PCI ischaemic risk including stent thrombosis. 3
DECLARATIONS
PAG has received research funding, consultation fees and honoraria from Astra Zeneca, Daiichi Sankyo/Lilly, Pozen, Bayer Healthcare, Sanofi-Aventis, CSL Pharmaceuticals, Accumetrics, Nanosphere and Haemoscope and honoraria from Merck, Daiichi Sankyo/Lilly, Boerhinger Ingleheim, Johnson and Johnson, AstraZeneca and Discovery Channel; YHJ received honoraria for lectures from Sanofi-Aventis, Daiichi Sankyo Inc. and Otsuka; UST received honoraria from Accuemtrics
This study was sponsored by Sinai Hospital of Baltimore
Not applicable
Sinai Hospital of Baltimore
All of the authors contributed to this manuscript and PAG supervised the writing
Methods
The authors searched PubMed and Ovid databases for English language articles addressing personalized antiplatelet therapy and also previous articles written by the authors through March 2012. The keywords – platelet, platelet function, genetic testing, clopidogrel and acute coronary syndrome (ACS) were used.
Genotype and clopidogrel metabolism
Clopidogrel is a prodrug that requires conversion into an active metabolite for biological activity. Approximately 85% of absorbed clopidogrel is hydrolyzed by hepatic carboxylesterase-1 into an inactive carboxylic acid metabolite, and 15% is metabolized in a two-step oxidative process into an active metabolite by hepatic cytochrome P450 (CYP). It has been proposed that CYP2C19 is the major enzyme involved in the generation of clopidogrel active metabolite. The labile active metabolite forms a disulphide bond with the P2Y12 receptor as platelets pass through the liver, irreversibly binding and antagonizing the receptor for the lifespan of platelets. 2 Clopidogrel response variability has been mainly attributed to the variability in active metabolite generation which in turn is caused by: (1) variable absorption that may be influenced by an ABCB1 gene polymorphism and (2) variability in CYP isoenzyme activity that is influenced by SNP carriage and drug–drug interactions. 2
P-glycoprotein (P-gp) is an adenosine triphosphate-dependent efflux transporter encoded by the ABCB1 gene.
4
Controversy exists regarding whether the ABCB1 C3435T variant is associated with clinical outcomes in clopidogrel-treated patients.2,3 Several SNPs influence CYP2C19 enzyme activity. The CYP2C19*1 allele denotes the wild type (i.e. normal function) and the two most frequent variants associated with LoF SNPs are CYP2C19*2 resulting in a non-functioning protein and CYP2C19*3, resulting in a premature stop codon.5,6 The gain-of-function (GoF) CYP*17 allele is associated with increased gene transcription and increased enzyme expression. The frequency of these alleles differs across ethnicity (Figure 1).
6
SNPs of CYP2C19 gene and prevalence of genetically predicted metabolizers in different ethnicities. Reprinted from Gurbel PA, Shuldiner AR, Bliden KP, Ryan K, Pakyz RE, Tantry US. The relation between CYP2C19 genotype and phenotype in stented patients on maintenance dual antiplatelet therapy. Am Heart J 2011;161:598-604, with permission from Elsevier
Hulot et al. 7 first demonstrated impaired clopidogrel responsiveness in young healthy male subjects with the CYP2C19*1/*2 genotype compared with the CYP2C19 wild type (*1/*1). Subsequently, numerous studies in healthy individuals have shown consistent findings of a negative influence of CYP2C19 LoF allele carriage on clopidogrel response across ethnic groups.3,5,7–9 In May 2009, the US Food and Drug Administration first added information about CYP2C19 genetically predicted poor metabolizers (*2/*2) to the Plavix drug label. It noted that healthcare professionals should be aware that tests are available to determine genotype and the antiplatelet response in poor metabo-lizers is increased by high-dose clopidogrel. However, this observation in healthy volunteers has not been observed in patients treated with PCI. Use of other antiplatelet agents or alternative dosing strategies of clopidogrel to overcome the influence of the LoF allele was also proposed. 4
The influence of CYP2C19*2 carriage on clopidogrel response variability was confirmed by a genomewide association study conducted in healthy Amish individuals administered clopidogrel (75 mg/day) for seven days. In this study, the contribution of the CYP2C19 locus to clopidogrel response variability as measured by ADP-induced platelet aggregation was ∼12% and the association increased in a gene–dose-dependent manner. Subsequently, other studies indicated that CYP2C19*2 allele carriage status was accountable for up to 12% of clopidogrel response variability or on-treatment platelet reactivity to ADP. In addition to CYP2C19*2, CYP2C19*3 carriage, which is more common among the East Asian population, was also associated with a reduced response to clopidogrel. 10
In a study by Gurbel et al. involving stented patients on DAPT, there was no association of *2 or *17 allele carriage with platelet reactivity during aspirin therapy alone. During DAPT, platelet aggregation was higher in those carrying the *2 allele than in non-carriers (P ≤ 0.01), but did not differ between those carrying the *17 allele and non-carriers. There was a significantly higher prevalence of HPR based on 20 μmol/L ADP-induced aggregation in *2 allele carriers (49%) compared with wild type (26%) and *17 (20%) carriers. However, platelet function on DAPT was highly variable within all genotype groups except for *2 homozygotes where platelet reactivity was above the HPR threshold (Figure 2).
6
Platelet aggregation stimulated by 5 and 20 μmol/L ADP and prevalence of HPR in patients on clopidogrel maintenance therapy and relation to CYP2C19*2 genotypes. Reprinted from Gurbel PA, Shuldiner AR, Bliden KP, Ryan K, Pakyz RE, Tantry US. The relation between CYP2C19 genotype and phenotype in stented patients on maintenance dual antiplatelet therapy. Am Heart J 2011;161:598-604, with permission from Elsevier
Genotype and clinical outcomes
The influence of the CYP2C19 genotype on clinical outcomes in patients treated with clopidogrel has been studied extensively in coronary artery disease patients undergoing stenting and patients with ACS.3,5,9 In the TRITON-TIMI 38 (Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition with Prasugrel–Thrombolysis In Myocardial Infarction 38) trial of ACS patients undergoing PCI treated with clopidogrel,
9
CYP2C19 LoF allele carriers had a 53% relative increase in the composite of cardiovascular death, MI or stroke, as compared with non-carriers (12.1% versus 8.0%; hazard ratio [HR], 1.53; 95% confidence interval [CI], 1.07–2.19; P = 0.01) and three-fold increase in the risk of stent thrombosis (2.6% versus 0.8%; HR, 3.09; 95% CI, 1.19–8.00; P = 0.02). Other studies and meta-analyses subsequently strengthened the observation of an association between CYP2C19 LoF variant carriage and thrombotic clinical outcomes in PCI patients receiving clopidogrel therapy.11,12 In a collaborative meta-analysis of nine clinical studies involving 9684 patients (91% treated by PCI and 55% of whom had ACS),
11
carriers of one or two CYP2C19*2 alleles exhibited significantly increased rates of cardiovascular events compared with non-carriers (HR, 1.55; 95% CI, 1.10–2.17; P = 0.01 and HR, 1.76; 95% CI, 1.24–2.5; P = 0.002, respectively). There was an increased risk of stent thrombosis among carriers of one or two CYP2C19 LoF alleles (HR, 2.67; 95% CI, 1.69–4.22; P < 0.0001 and HR, 3.97; 95% CI, 1.75–9.02; P = 0.001, respectively). Indeed, the observations showing an association between CYP2C19 genotype and clinical outcomes during clopidogrel administration are mostly derived from platelet-oriented ischaemic events: PCI-related MI or stent thrombosis. Therefore, the influence of CYP2C19 genotype on ischaemic event occurrence has not been demonstrated in non-PCI patients (Figure 3).13,14
Relation of CYP2C19 loss-of-function carrier status to clinical outcomes in clopidogrel trials. HRs are presented at the top of the respective columns. ACTIVE, Atrial Fibrillation Clopidogrel Trial with Irbesartan for Prevention of Vascular Events; CURE, Clopidogrel in Unstable Angina to Prevent Recurrent Events; LoF, loss-of-function allele
Finally, it should be noted that the CYP2C19 isoenzyme is not the only factor determining the antiplatelet response to clopidogrel since even in genetically predicted poor metabolizers, some degree of platelet inhibition has been observed where no enzyme activity is expected. It is conceivable that in CYP2C19 poor metabolizers, other isoenzymes, particularly CYP3A4, a very abundant hepatic enzyme, may play an important role in clopidogrel bioactivation. Moreover, clopidogrel metabolism is influenced by concomitantly administered agents such as proton pump inhibitors, calcium channel blockers, warfarin and cigarette smoke that either inhibit or enhance CYP activity or compete with clopidogrel during hepatic CYP-mediated metabolism (Figure 4).
15
Therefore, the evaluation of the CYP2C19 metabolic phenotype, for example, by the pantoprazole breath test, may be more informative than genotyping alone.
16
In addition, demographic variables such as age, renal failure, diabetes and body mass index also influence the platelet response to ADP by either directly affecting platelet function or by affecting clopidogrel metabolism. The final platelet reactivity phenotype and clinical outcomes of patients treated with clopidogrel are the result of all of these influences. However, genotyping may be more relevant in clopidogrel naive patients to be treated with PCI to determine the optimal initial antiplatelet treatment strategy. Whether genetic testing is complementary to platelet function testing is unknown. A comparison of genetic and platelet function testing is given in Table 1.
Various factors influencing platelet reactivity and clinical outcome during clopidogrel therapy. BMI, body mass index; CAD, coronary artery disease; CCB, calcium channel blocker; DDI, drug-drug interaction; LPR, low on-treatment platelet reactivity; PPI, proton pump inhibitor; SJW, St John's wort. Reprinted from Gurbel PA, Ohman EM, Jeong YH, Tantry US. Toward a therapeutic window for antiplatelet therapy in the elderly. Eur Heart J 2012;33:1187-9, with permission from the European Society of Cardiology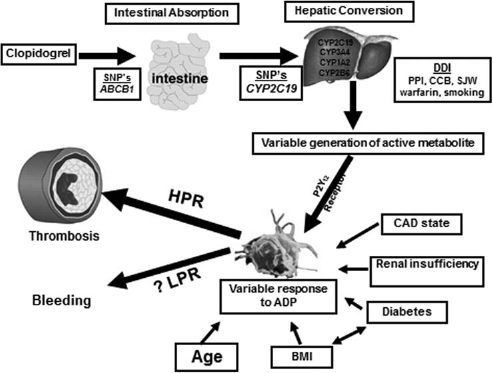
Comparison between genotyping and platelet function testing

Rationale for platelet function testing
Clopidogrel response variability was first reported in the PCI population in 2003. 1 In 2005, the relation of poststenting ADP-induced platelet aggregation to ischaemic event occurrence was first demonstrated in the PREPARE-POST-STENTING study. 16 Since then numerous translational research studies conducted worldwide involving thousands of patients utilizing multiple laboratory tests have reached the identical conclusion: patients treated with PCI who have high platelet reactivity to ADP (HPR) are at increased risk for both short-term and long-term post-PCI ischaemic event occurrence, including stent thrombosis.5,6,17 These studies have primarily used a single measurement of reactivity determined either immediately before PCI or at the time of hospital discharge. A recent consensus statement proposed cut-off values based on receiver operating characteristic (ROC) curve analysis for different platelet function assays to be used in future studies of personalized antiplatelet therapy (Table 2).18–21
Important studies linking HPR to ischaemic events based on ROC curve with a specific cut-off value

AU, aggregation units; CVD, cardiovascular disease; LTA, light transmittance aggregometry; MACE, major adverse clinical events; VASP-PRI, vasodilator stimulated phosphoprotein-platelet reactivity index
In a meta-analysis of studies using the Verify-Now point-of-care assay, a higher rate of composite primary endpoint occurrence was associated with a PRU (P2Y12 reaction units) ≥230 (HR, 2.10; 95% CI, 1.62–2.73; P < 0.0001). In addition, death (HR, 1.66; 95% CI, 1.04–2.68; P = 0.04), MI (HR, 2.04; 95% CI, 1.51–2.76; P < 0.001) and stent thrombosis (HR, 3.11; 95% CI, 1.50–6.46; P = 0.002) were also associated with the same PRU cut-off, lending further support for the potential role of monitoring P2Y12 receptor blocker therapy as a prognostic marker. 22 Furthermore, in the recently presented ADAPT-DES (Assessment of Dual Antiplatelet Therapy with Drug-Eluting Stents) study (n = 8349), an investigation of the relation of post-PCI platelet reactivity measured by the Verify Now assay to thrombotic event occurrence, patients with >208 PRU had a three-fold adjusted hazard for the occurrence of 30 day stent thrombosis. 23 Fifty percent of 30 day definite or probable stent thrombosis occurrence was solely attributable to HPR by multivariate analysis.
Similarly, recent observational studies indicated that very low platelet reactivity was associated with bleeding.
24
The concept of a therapeutic window of P2Y12 receptor reactivity associated with both ischaemic event occurrence (upper threshold) and bleeding risk (lower threshold) has been proposed similar to the international normalized ratio range used for coumadin therapy, potentially allowing for personalization of antiplatelet therapy (Figure 5).
25
Post-PCI ischaemic/thrombotic clinical events. The sigmoid cumulative frequency curve in patients with post-PCI ischaemic/ thrombotic clinical events relative to platelet reactivity to ADP. These data support the concept of a therapeutic window for P2Y12 blockade. Reprinted from Bonello L, Tantry US, Marcucci R, et al. Consensus and future directions on the definition of high on treatment platelet reactivity to adenosine diphosphate. J Am Coll Cardiol 2010;56:919-33, with permission from the American College of Cardiology Foundation
Prospective personalized antiplatelet studies
Small prospective studies have provided evidence that HPR is not just a prognostic marker but a modifiable risk factor. Tailored incremental loading doses of clopidogrel and selective GP IIb/IIIa receptor blocker administration administered to PCI patients with HPR following clopidogrel loading was effective in reducing subsequent post-PCI ischaemic outcomes.26,27 In the GRAVITAS (Gauging Responsiveness with a Verify Now Assay-Impact on Thrombosis and Safety) trial, the first large scale investigation of personalized antiplatelet therapy in elective PCI, patients with >236 PRUs (n = 2214) were randomly assigned to receive either high-dose (600 mg initial dose and 150 mg/day thereafter) or standard-dose clopidogrel (no additional load, 75 mg/day). 28 The same six-month composite ischaemic event occurrence (only 2.3%) was observed in the high- and standard-dose groups. GRAVITAS enrolled many low-risk patients; the event rates were very low; and the regimen to combat HPR (double-dose clopidogrel) was phar-macodynamically suboptimal (40% HPR prevalence at 30 days). All of these factors may have affected the ability to assess the utility of personalization (56). However, the possibility remains that HPR is a non-modifiable risk factor. 29 The result of the large scale PLATO (Study of Platelet Inhibition and Patient Outcomes) and TRITON trials that demonstrated a greater antithrombotic effect associated with P2Y12 inhibitors that have more potent ex vivo antiplatelet effects than clopidogrel argue strongly against HPR being a non-modifiable risk factor.30,31 The HPR threshold mentioned in the consensus statement was determined by ROC curve analysis and is only applicable to the PCI population. However, based on the group of patients from GRAVITAS treated with standard-dose clopidogrel, an even lower threshold defining HPR (∼170 PRU) was associated with optimal identification of patients destined to experience ischaemic event occurrence. It was suggested that this ‘immunity to thrombosis’ cut-off should be considered the new therapeutic target in the PCI patient. 32
It should be taken into consideration that the currently accepted HPR cut-off values have been associated in many studies with modestly increased odds ratios for ischaemic event occurrence and are associated with high negative predictive values and low positive predictive values (PPV). However, given the overall low prevalence of thrombotic events, the low PPV is not unexpected. 3 Although platelet reactivity plays a major role in ischaemic event occurrence, adding demographic and clinical variables and, potentially, genotype to platelet reactivity measurements to form a combined risk factor may improve risk prediction. Future algorithms that include the results of a platelet function test and genetic testing with other factors, similar to a TIMI or Global Registry of Acute Coronary Events risk score, may improve our ability to detect the thrombosis-prone patient and optimally guide the antiplatelet therapy regimen.
It has also been argued that stent thrombosis rates are so low now in the era of third generation DES that the magnitude of the clinical problem is not as great as before. A common response from the interventionalist is, ‘I just don't see stent thrombosis in my practice’. However, in the contemporary ADAPT DES registry, 30-day stent thrombosis rates in patients with PRU >208 was 0.81%. 23 Finally, it may be impossible now to conduct any prospective personalized antiplatelet therapy trial where there is randomization to a known inferior pharmacodynamic regimen once HPR is identified. The latter impediment was demonstrated in the aborted TRIGGER-PCI (Testing Platelet Reactivity in Patients Undergoing Elective Stent Placement on Clopidogrel to Guide Alternative Therapy with Prasugrel trial) where about one-third of patients declined randomization once they knew they had HPR. 33
Ongoing studies, including the TRILOGY ACS (Targeted Platelet Inhibition to Clarify the Optimal Strategy to Medically Manage Acute Coronary Syndromes) (NCT#00699998) Platelet Function Substudy and future studies will provide valuable information and potentially influence the field of personalized antiplatelet therapy.
Personalized antiplatelet therapy in the surgical patient
Irreversible inhibition of platelet function associated with thienopyridine therapy carries a substantial risk of bleeding, particularly in patients undergoing coronary artery bypass graft surgery (CABG). Up to 15% of patients presenting with ACSs will require CABG, and bleeding complications and transfusion of red blood cells in these patients have been associated with adverse outcomes. In a recent study, the utility of triaging patients-based clopidogrel responsiveness measured by thrombelastography for the first time isolated on-pump CABG was demonstrated. 16
Conclusions
The evidence to this date indicates that CYP2C19 LoF allele carrier status is an important independent predictor of the pharmacodynamic response to clopidogrel. HPR and CYP2C19 LoF carriage are associated with clinical outcomes in high-risk clopidogrel-treated patients who have undergone PCI. However, recent studies have indicated that high maintenance-dose clopidogrel (150 mg daily) is not a highly effective strategy to overcome the influence of LoF allele carriage, particularly in poor metabolizers.
3
Data from TRITON TIMI-38 and PLATO trials strongly suggest that prasugrel and ticagrelor are effective alternatives to overcome the influence of the LoF allele carrier status and pharmacodynamic studies suggest that prasugrel and ticagrelor are effective in overcoming HPR status during clopidogrel therapy (Figure 6).9,34–36 Two ongoing trials, ARCTIC (NCT#00827411) and PAPI-2 (NCT#01452152) are prospective personalized antiplatelet therapy trials that will add important information about the role of phenotyping and genotyping, respectively.
Prasugrel and ticagrelor are effective in overcoming influence of LoF allele status during clopidogrel therapy. TRITON-TIMI, trial to assess improvement in therapeutic outcomes by optimizing platelet inhibition with prasugrel-thrombolysis in myocardial infarction; PLATO, platelet inhibition and patient outcomes
Therefore, it may be reasonable at this time to assess platelet function in clopidogrel-treated high-risk patients (patients with current or prior ACS, history of stent thrombosis and target vessel revascularization, poor left ventricular function, multivessel stenting, complex anatomy [e.g. bifurcation, long and small stents], high body mass index, diabetes mellitus and patients co-treated with proton pump inhibitors) and treat with more potent P2Y12 receptor therapy selectively. Clopidogrel is pharmacodynamically effective in about two-thirds of patients undergoing PCI; these patients do not have HPR. Ischaemic risk is much greater in patients with HPR. Therefore, selectively treating two-thirds of patients with generic clopidogrel may provide significant cost-savings. Unselected therapy with the new P2Y12 receptor blockers is associated with increased bleeding. Although we do not yet have conclusive evidence from a large-scale randomized trial that personalized antiplatelet therapy improves patient outcomes, a class IIb recommendation has been given in the European and American guidelines to perform genotyping or phenotyping in high-risk PCI patients if a change in antiplatelet therapy will ensue based on the test results.37–39
Footnotes
Acknowledgements
None