
Abstract
Polyarteritis nodosa (PAN) is characterized by multisystem necrotizing vasculitis, primarily affecting small-to-medium-sized muscular arteries, and it is typically found in middle-aged men. PAN is rarely found in the female genital tract (including the uterus), and imaging of the uterus with PAN has not previously been reported. Reported is a case of a 78-year-old patient with uterus enlargement who was diagnosed with PAN through clinical findings and images. Computed tomography and magnetic resonance imaging findings of a uterus affected by PAN are presented and reviewed, and potential characteristic findings of the uterine with PAN are discussed.
Polyarthritis nodosa (PAN), which predominantly involves small-to-medium-sized arteries such as the renal arteries and arteries in the skin, rarely involves the female genital tract (1,2). Although computed tomography (CT) and magnetic resonance imaging (MRI) have previously revealed PAN by in the renal and gastrointestinal tract arteries, it has not revealed PAN in the female genital tract. Reported is a case of an elderly woman with PAN of the uterus confirmed by CT and MRI.
Case report
A 78-year-old woman with a history of hepatitis B and Sjögren syndrome was admitted to a local clinic near her house experiencing prolonged fever and leg pain. After being transferred to our hospital, a complete physical examination revealed leg livedo. She did not notice atypical genital bleeding. Laboratory tests showed high levels of C-reactive protein, a high white blood cell count and a high erythrocyte sedimentation rate. The patient's tumor markers were normal, except for high CA-125. In order to exclude aortitis, focal infection, or malignancy, a whole-body contrast-enhanced multidetector-row computed tomography (MDCT) examination was performed and three-dimensional CT angiography (3-D CTA) was reconstructed. Transaxial images and maximum intensity projection (MIP) of the MDCT showed multiple microaneurysms in the liver (Fig. 1a and b) and irregularity and ectasia of the celiac and renal arteries (Fig. 1c). Multiple microaneurysms in the liver and irregularity and ectasia of the renal arteries were seen with 3-D CTA (Fig. 1d). Transaxial images of the MDCT showed that the patient's uterus was large for her age (Fig. 2). In order to rule out endometrial cancer, pelvic MRI was performed. T2-weighted imaging (WI) and diffusion-weighted imaging (DWI) showed the thickness of the endometrium and uterine muscle. T2-WI and DWI (Fig. 3a and b) also showed high signal intensity in part of the parametrium. However, MRI did not show disarray of the uterus’ structure or a tumor. A pathological examination of the endometrium performed to rule out the presence of endometrial cancer showed significant infiltration of neutrophils with no malignancy. Hence, she and her condition were carefully followed.
Based on physical findings (leg pain, livedo, elevated C-reactive protein, and fever) and the microaneurysms found in her liver by 3-D CTA, systemic polyarteritis nodosa (PAN) was diagnosed and methylprednisolone was administered. Two months later, her fever and leg pain had disappeared. Follow-up whole-body CT with 3-D CTA and pelvic MRI were then performed. Follow-up 3-D CTA showed that the multiple microaneurysms in her liver had completely disappeared, although irregularity and ectasia of the celiac and renal artery had remained (Fig. 4). Follow-up pelvic MRI showed that the thickness of both the uterine endometrium and muscle had diminished, and the signal intensity on both DWI and T2-WI in the parametrium had decreased (Fig. 5).
(a) Initial MDCT of the arterial phase shows multiple microaneurysms (arrow) in the left hepatic lobe. (b) Initial MDCT of the arterial phase shows the ectatic right renal artery (arrow). (c) Multiple microaneurysms of the liver are clearly seen on the MIP (arrow). (d) 3-D CTA shows multiple microaneurysms in the liver (red arrow) and irregularity and ectasia of the right renal artery (yellow arrow)
Initial MDCT of the delayed phase shows a uterus that is large for the patient's age as well as thickening of the endometrium and the uterine muscle (arrow)
Discussion
Polyarteritis nodosa (PAN) is a systemic necrotizing vasculitis of medium and small arteries that rarely involves the female genital tract. It is divided into two types: isolated PAN and systemic PAN. Isolated PAN affects the female genital tract more frequently than systemic PAN (3). Additionally, patients with systemic PAN are older than patients with isolated PAN. Systemic PAN presents with less vaginal bleeding but more asymptomatic pelvic masses than seen with isolated PAN. Moreover, when PAN is found in the female genital tract, isolated PAN is primarily found in the cervix, but systemic PAN involves multifocal aspects of the female genital tract (3). These previously reported results are compatible with the present case.
(a) Initial T2-weighted MRI shows thickening of the endometrium and the uterine muscle with high signal intensity (arrow). (b) Initial DWI shows high signal intensity of the endometrium, uterine muscle and left parametrium
In this case, although asymptomatic thickening of the endometrium was seen, the possibility of endometrial cancer could not be excluded. Retrospectively, three characteristic findings were identified. First, although uterus enlargement was found, thickening was seen not only in the endometrium but in the uterine muscle as well. Therefore, the uterine structure was anatomically normal. Second, both the uterine muscle and a part of the parametrium showed diffusely high signal intensity on DWI. No continuity of high signal intensity was found on DWI between the Uterus muscle and the parametrium. Although high signal intensity of the uterus and the parametrium on DWI may suggest not only inflammation but also cancer, the lack of continuity is compatible with systemic PAN, which involves the multifocal female genital tract. Third, after the methylprednisolone was administrated, the uterine size normalized and the high DWI signal intensity of the endometrium, muscle, and parametrium resolved.
Follow-up 3-D CTA after treatment with methylprednisolone shows that the multiple microaneurysms of the liver had completely disappeared (red arrow), although the irregularity and ectasia of the right renal artery remained (yellow arrow)
According to previous literature, hysterectomy is usually performed in these types of cases because the uterine enlargement was suspected to be caused by endometrial cancer (4,5). If it is determined that the uterine enlargement is caused by PAN, hysterectomy can be avoided. However, in order to make a definite diagnosis of PAN, especially in the female genital tract, it is necessary to prove the presence of necrotizing vasculitis during the pathological examination. MRI can contribute to the diagnosis of PAN of the uterus.
(a) Follow-up on T2-WI shows that the thickening of the uterine endometrium and muscle is resolving. (b) Follow-up 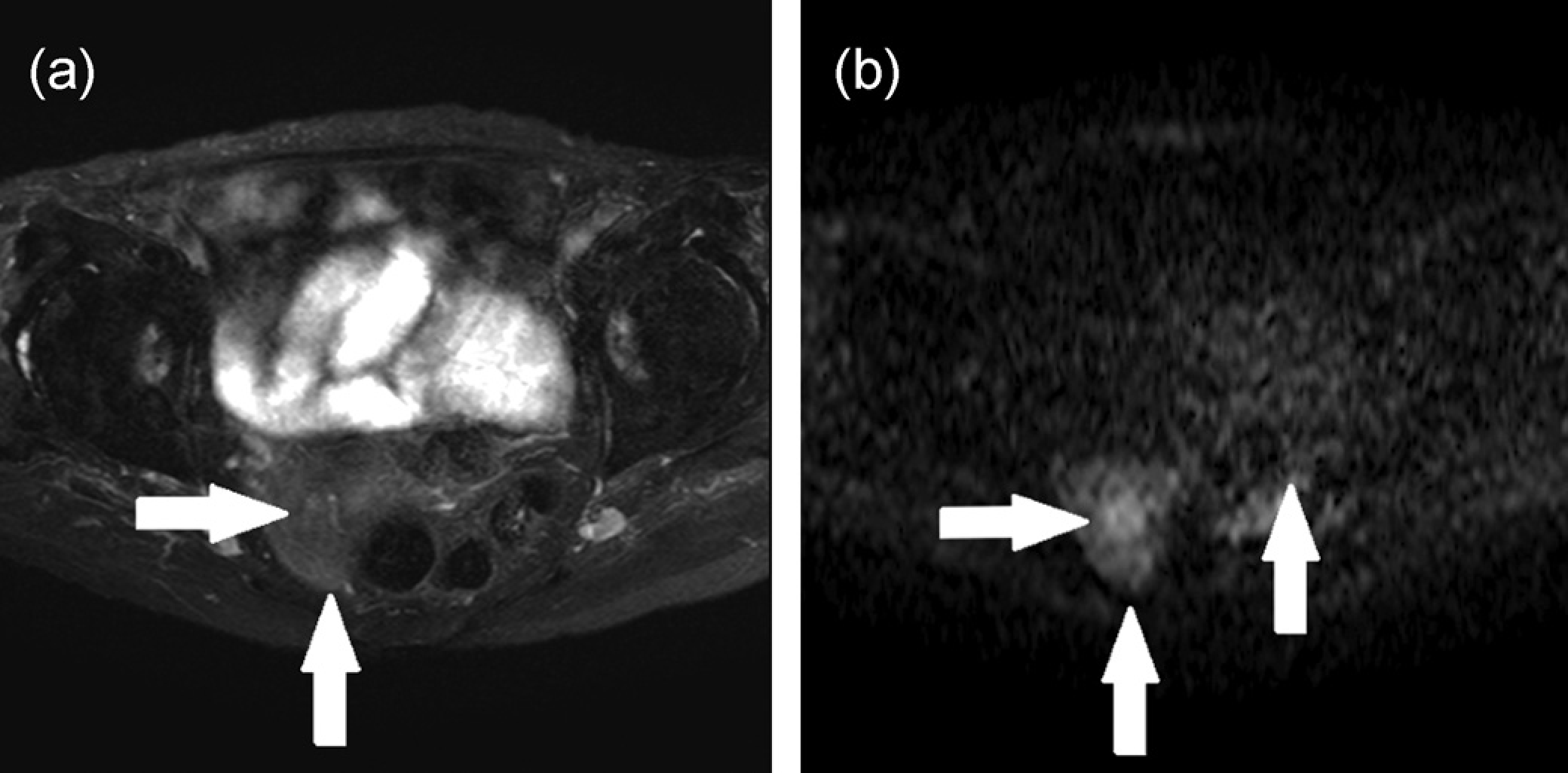
In conclusion, the characteristic MR findings highlighted in the present report may be helpful for differentiation between PAN involving the uterus and endometrial cancer.