
Abstract
We report the case of a 26-year-old man who presented with a non-painful priapism with a history of 3 months permanent erection after suffering a perineal trauma. An arteriocorporal fistula with a turbulent flow between the right cavernosal artery and the corpus cavernosum, conclusive for a high-flow priapism was initially detected by colour Doppler ultrasound. A superselective embolization with Gelatin sponge was safe and effective to treat the high-flow priapism. The use of gelatin sponge resulted in a temporary embolization with long-term effect of penile detumescence and preservation of erectile function.
Priapism is defined as a pathological condition of a penile erection that persists beyond or is unrelated to sexual stimulation (1–4). Following the recommendations of the American Urological Association (AUA) priapism is categorized into ischemic and non-ischemic priapism. Essential elements of the ischemic or low-flow priapism are clinical characteristics of pain and rigidity, diagnostic characteristics of absence of cavernosal arterial blood flow, pathophysiological characteristics of a closed compartment syndrome, and a time limit of 4 h prior to emergent medical care (2). The ischemic type which arises from many varied causes mandates immediate intervention. The underlying mechanism is a veno-occlusive outflow obstruction and high cavernous pressures. Corporal fibrosis and permanent erectile dysfunction can result from ischemic priapism that fails to resolve with therapy (5).
The non-ischemic or high-flow type is usually the result of perineal trauma. Patients typically present with a painless erection due to an arterial damage leading to arteriocorporal fistulas (ACF) (6–8) and occasionally, to an associated pseudoaneurysm (9). Transcatheter embolization of the distal internal pudendal arteries is the treatment of choice for high-flow priapism and a useful alternative to surgery (7). Most patients present to the emergency department within the first week after suffering from pelvic trauma causing a progressive priapism (10). However, there may be spontaneous resolution of high-flow priapism in non-treated patients even weeks after a postperineal trauma (11).
We describe a case of a chronic high-flow priapism without penile detumescence for more than 3 months.
Case report
A 26-year-old man presented with a non-painful priapism in the urology ambulatory care unit. The patient reported having a permanent full erection for more than 3 months following a perineal trauma by falling from a ladder and hitting his pelvic floor on the window board. The physical examination 3 months after the trauma revealed stiff corpora cavernosa and a well-perfused corpus spongiosum. There was no visible or palpable perineal trauma. He had no history of sickle cell disease and denied any use of cocaine. The ability to perform sexual intercourse was not impaired. A penile color Doppler sonography was performed and demonstrated an arteriocorporal fistula with turbulent flow between the right cavernosal artery and the corpus cavernosum, conclusive for a high-flow priapism.
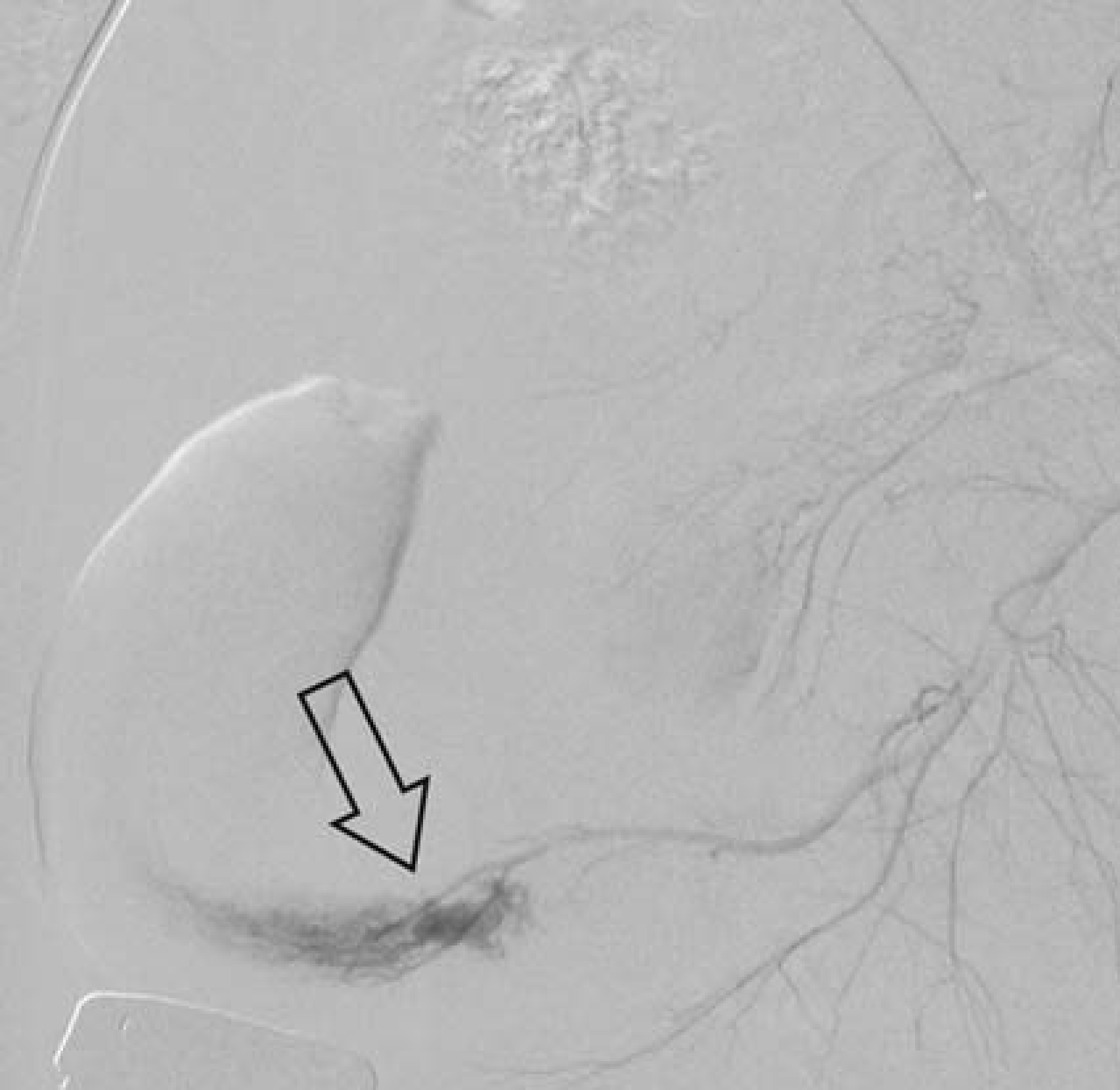
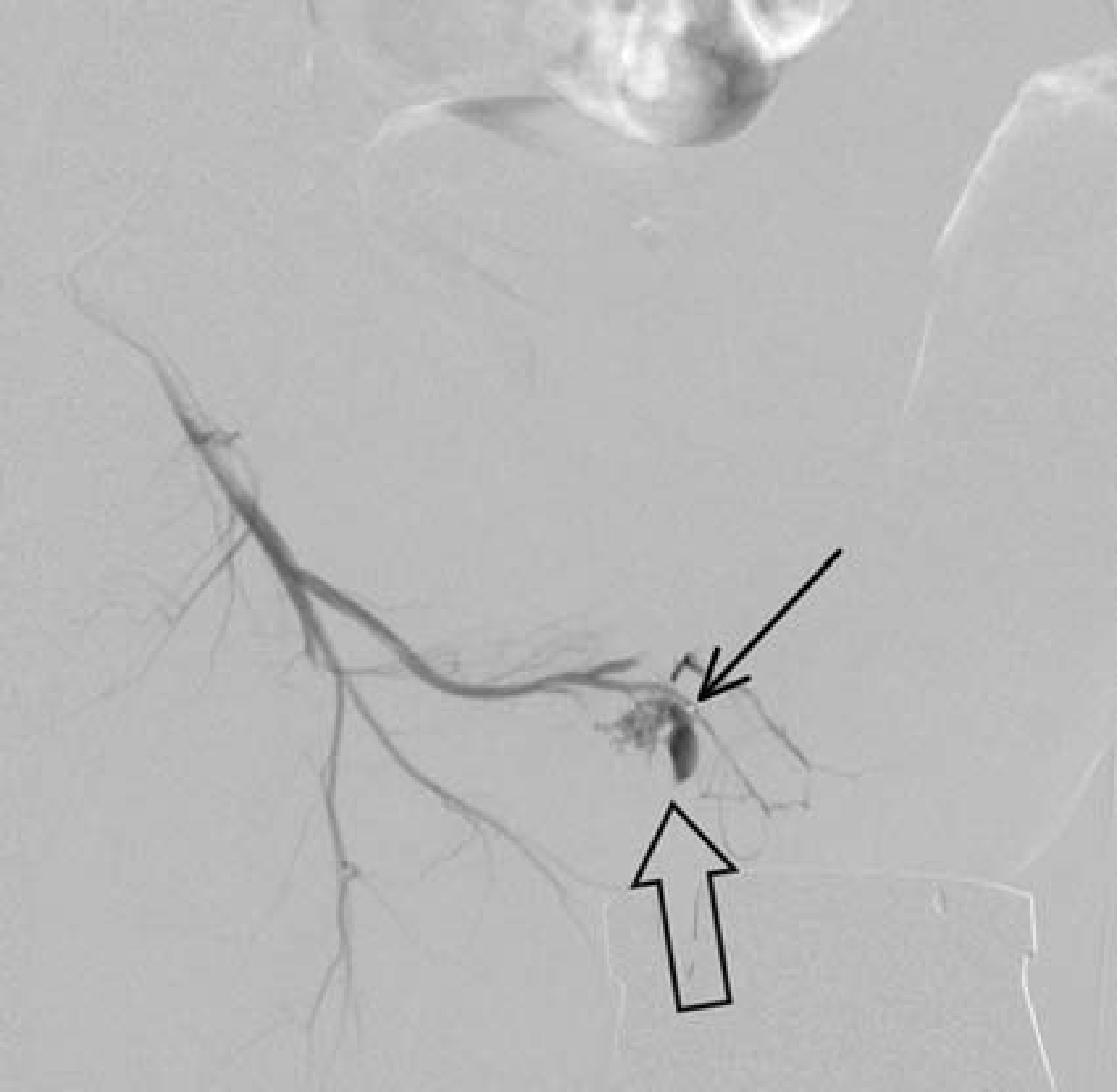
The patient was admitted to our hospital and a selective angiography was performed. The internal pudendal artery was catheterized bilaterally with a 4 F RIM Tempo4 open-ended catheter (Cordis, Miami, FL, USA) by a right transfemoral approach and a selective angiography was performed. The diagnostic angiography revealed the presence of a bilateral contrast leak from the cavernosal artery to the corpus cavernosum which was most prominent via the right cavernosal artery (Figs. 1 and 2). Thereafter a microcatheter (2.7 F; Microferrit; Cook, Bloomington, IN, USA) was placed into the cavernosal artery with its catheter tip positioned right into the leak to the corpus cavernosum (Fig. 3). The fistula was then embolized with gelatin sponge. The gelatin sponge was prior to the procedure fragmented into small pieces with a scalpel and eluted in contrast media resulting in a viscous thick fluid. Approximately 2 mL of the gelatin contrast media elution was injected via the microcatheter until stasis of the leakage was obtained. A superselective embolization via the right cavernosal artery was performed. The ACF disappeared completely (Fig. 4). The patient described a complete penile detumescence 48 h after the procedure.

The selective angiography of the right internal pudendal artery demonstrating a mark blush of contrast media which is resulting from arteriocavernosal fistula (arrow) from injury of the cavernosal artery
There is a bilateral arteriocavernosal fistula (arrow), less prominent in the angiogram of the left internal pudendal artery
For gelatin sponge embolization a microcatheter is placed with its catheter tip (thin arrow) into the orifice of the arteriocavernosal fistula (large arrow)

The selective angiogram of the right internal pudendal artery shows a complete occlusion of the arteriocorporal fistula. The gelatin sponge is impacted in the corpus cavernosum (arrow)
Follow-up consisted of a color Doppler sonography 6 weeks after embolization. No ACF was detectable. The cavernosal arteries and the corpora cavernosa were bilaterally intact and well perfused. The priapism resolved completely and the patient reported a normal erectile function (Fig. 5).

A follow-up color Doppler sonography performed 6 weeks after embolization shows intact cavernosal arteries and corpora cavernosa bilaterally (large arrows). (a) Sagittal ultrasound scan, (b) axial ultrasound scan of the penis base, dorsal arteries (thin arrows), doral vein (transparent arrow)
Discussion
Selective arterial embolization is recommended for the management of non-ischemic priapism in patients who request treatment (12). Autologous clot (10) and absorbable gels (13, 14), which are non-permanent embolizing agents, are preferable to microcoils (15), N-butyl-cyanoacrylate (1) or polyvinyl alcohol (16), being permanent agents, in the inter-ventional radiologic management of non-ischemic priapism (5). Surgical management of non-ischemic priapism such as the ligation of the internal pudendal artery may be regarded as an option of last resort (3). Some authors suggest a conservative approach with external perineal compression as treatment option (17). In literature the spontaneous resolution rate of a high-flow priapism is reported with up to 62% (18).
The rationale of the arterial embolization approach is to achieve detumescence at an early stage in order to prevent impairment of the erectile function. Even if the consequences of non-ischemic high-flow priapism are not severe, it is still associated with a social inconvenience. In our case the patient was seeking help at the urology ambulatory care unit as late as 3 months after the initial perineal trauma mainly because of personal discomfort. The temporary embolization with gelatin sponge seems to be the least invasive embolization method avoiding the risk of permanent vascular occlusion and postprocedure erectile dysfunction (19). The reviewed literature indicates resolution of high-flow priapism in 78% of cases treated with permanent embolization techniques and an associated erectile dysfunction rate of 39%. In contrast, temporary embolization techniques had a 74% resolution rate and 5% associated erectile dysfunction rate (3).
In conclusion, the primary goal of the treatment for high-flow priapism is to resolve penile erection and at the same time preserve erectile function. The use of color Doppler sonography is useful in confirming the diagnosis. Selective arterial embolization has been identified as the treatment of choice. In our case a temporary embolization with gelatin sponge proved to have a long-term effect on penile detumescence and preservation of erectile function.