
Abstract
Lymphatic malformation/lymphangioma of the scrotum is rare. It is caused by lymphatic abnormalities and the most common sites are the neck and axilla. The scrotum is one of the most uncommon sites. We report the case of a 12-year-old boy with pathologically confirmed cystic lymphangioma/lymphatic malformation in the scrotum. The diagnosis was suspected from ultrasonography and magnetic resonance imaging. The most common cause of a cystic mass in the scrotum is scrotal hydrocele, but cystic lymphangioma/lymphatic malformation should be considered as a differential diagnosis for multicystic scrotal mass.
Lymphatic malformation/lymphangioma is composed of dilated lymphatic vessels caused by occlusion of the lymphatic drainage system due to congenital malformations or acquired causes such as the effects of trauma, infection, or surgery. The most common sites are the neck and axilla. The scrotum is one of the most uncommon sites. Two hypotheses have been proposed: that the condition results from malformation of lymphatic vascular pathways; and that it represents a tumor that grows by cellular (mainly endothelial) hyperplasia (1,2). The International Society for the Study of Vascular Anomalies (ISSVA) has classified vascular anomalies into these two categories. After a couple of revisions, the newest version of ISSVA classification refers to this condition as a vascular malformation (3). However, Ozeki reported that lymphangiomatosis of the thoracic wall shrank with administration of propranolol, a β-blocker and blocker of vascular endothelial growth factor, similar to the response of infantile hemangioma. This implies a tumor-like nature to the growth of lymphatic malformation (4). Usage of the terms “lymphatic malformation” and “lymphangioma” thus remains controversial.
We report a case of lymphatic malformation/lymphangioma occurring in the scrotum, one of the most uncommon sites.
Case Report
A 12-year-old boy presented to our hospital with a swollen right scrotum without tenderness. He had a surgical history of bilateral inguinal hernia, uncal hernia, and scrotal hydrocele at 2 years old. Ultrasonographic examination revealed a well-defined multicystic mass in the right scrotum. Color Doppler examination showed no blood flow in the septum of the cysts (Fig. 1). Bilateral testes were normal. Magnetic resonance imaging revealed a multicystic mass (6.5 × 6.5 × 9.0 cm) with multiple thin septae and locules located in the right scrotal sac. The mass showed high intensity on T2-weighted imaging and low intensity on T1-weighted imaging. On diffusion-weighted imaging, the mass showed no restriction of diffusion. The mass had displaced the right testis to the left. No evidence of any extrascrotal extension into the abdomen was noted (Fig. 2a-c). The radiological diagnosis was multiple scrotal hyadrocele or lymphatic malformation/lymphangioma. Since right scrotal swelling was progressing, surgery was performed.
Ultrasonography shows cystic mass filled with low-echoic component (a); Color Doppler imaging reveals no flow in the mass (b)
(a) T2-weighted image, sagittal view. There are multicystic masses in the scrotum. The septae are thin and reveal low signal intensity. No solid component can be identified. (b) T1-weighted image (image on the left: in-phase, image on the right: opposed-phase). The mass has low signal intensity. There is no signal drop in the opposed phase. (c) Diffusion-weighted image reveals no abnormal hyper intensity in the mass (arrow). The nodule with high signal intensity (arrow head) is correspondent with right normal testes and is displaced to the left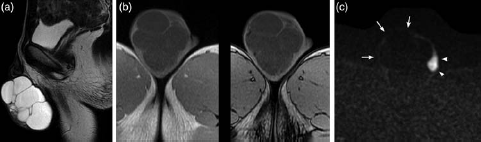
Surgical findings showed that the mass existing in the right scrotum had probably originated from the internal spermatic fascia. Microscopic examination revealed membranous tissue with some hemorrhage. Tissue thought to represent a thin wall of the cystic mass was identified as fibrous tissue with hemorrhage. Infiltration of lymphocytes around the small vessels was detected. Pathological findings were consistent with lymphatic malformation/lymphangioma.
Discussion
Lymphatic malformation/lymphangioma most frequently occurs in the head, neck, or axilla, and is occasionally found in the mediastinum or perineum. Lymphatic malformation/lymphangioma in the scrotum is very rare. A review of 535 pediatric cases with groin or scrotal swelling found lymphatic malformation/lymphangioma in only one case (0.2%) (5).
The pathophysiology of the lymphangioma is still controversial as mentioned above. In this case, previous surgery for hernia and hydrocele might have caused mechanical obstruction or overgrowth of lymphatic tissue and could thus have led to formation of the lymphatic malformation/lymphangioma.
The main clinical symptom is a non-tender swelling of the scrotum that gradually increases in size. Sudden enlargement with pain is usually a consequence of acquired causes such as trauma, hemorrhage, infection, or operation. Thickening of the scrotal epidermis can be seen when the cutaneous lymphatic flow is blocked in addition. The typical ultrasonographic findings of scrotal lymphatic malformation/lymphangioma are a multicystic extratesticular mass with homogeneous echo-free components showing no connection to the peritoneal cavity. The presence of echogenic components implies the existence of hemorrhagic materials or debris. Magnetic resonance imaging shows a multiloculated cystic mass with low signal intensity on T1-weighted imaging and high signal intensity on T2-weighted imaging. When hemorrhage is present, the component reveals rather lower intensity on T2-weighted imaging (6). Fluid-fluid levels are occasionally seen. Differential diagnoses include scrotal hydrocele, hematocele, inguinal hernia, spermatocele, spermatic varicoceles, and dilatation of the rete testis.
The Valsalva maneuver is useful to differentiate lymphatic malformation/lymphangioma from spermatic varico-celes and inguinal hernia. Presence of septal flow on color Doppler ultrasonography differentiates cystic lymphangioma/lymphatic malformation from hydrocele, pyocele, and hematocele, and the absence of color flow in the cystic spaces differentiates lymphangioma from varicoceles (7). However, in our experience, color Doppler examination cannot always show septal flow in lymphatic malformation/ lymphangioma. This may be partly explained if the septa are too thin to be detected on Doppler ultrasonography. Multiloculated scrotal hydrocele with no intraperitoneal extension is difficult to distinguish from lymphatic malformation/lymphangioma, since the imaging findings are almost the same.
Clinically, when a boy with enlarged scrotum and these image findings is encountered, we should first suspect scrotal hydrocele, as the prevalence of this disease is much higher than that of lymphatic malformation/lymphangioma. Diagnostic puncture is contraindicated for scrotal hydrocele, due to macroscopic or microscopic connections to the peritoneal cavity. Puncture can thus cause infection, which would differentiation from lymphatic malformation/lymphangioma even more difficult (8).
The history, clinical information and imaging findings should be considered comprehensively. Treatment basically involves complete surgical removal of the lesion. If any tissue remains, recurrence may result, so preoperative assessment of the location and nature of the lesion is critical.
In conclusion, scrotal lymphatic malformation/lymphangioma is rare, but represents an important differential diagnosis for multicystic scrotal mass.