
Abstract
Osteochondritis dissecans (OCD) of the humeral capitellum is a disorder affecting mainly boys between the ages of 12 and 15 years. The exact etiology of OCD is not clear, but it is believed that repetitive trauma is the primary cause. Genetic factors are thought to play a secondary role in the pathogenesis. We present 17-year-old identical twins with similar MRI and arthroscopic findings, suggesting that genetic components are involved in the etiology of OCD of the humeral capitellum.
Osteochondritis dissecans (OCD) is characterized by separation of an osteochondral fragment from the articular surface. The underlying bone from which the fragment separates has normal vascularity, as opposed to osteonecrosis (1). OCD of the humeral capitellum is a disorder affecting mainly boys aged 12 to 15 years. There is often a history of elbow overuse and many patients are baseball pitchers or other high valgus stress activity athletes (2-4). The exact etiology of OCD is not clear, but repetitive trauma to the poorly vascularized capitellum is believed to be the primary cause (5). Genetic factors are also thought to play a major role in the pathogenesis, but the data are rather limited (6-9). Here, we present 17-year-old identical twins with almost identical radiographic, MRI, and arthroscopic findings of OCD of the humeral capitellum.
Case report
17-year-old identical male twins had been actively playing ice-hockey for 7 years at a national level. During the last 18 months both patients had pain and occasional locking of the right elbow. The clinical history was unremarkable, as there were neither medical records nor history of previous major trauma to the elbow. Both were right-handed players, so more valgus stress on the right capitellum was created. On clinical examination, a slight extension deficit up to 5° of the affected elbow was present in both. There were no other clinical abnormalities.
Radiographs (Figs. 1 and 2) showed some flattening and subchondral lucencies of the articular surface of the capitellum in both patients. Also, multiple loose bodies in the joint space were seen. Twin B had a small osteochondral lesion at the anterior part of distal capitellar surface, and osteophytes at the medial aspect of the elbow as an early sign of arthrosis was seen as well. Joint effusion was present in both patients.

Lateral (a) and anteroposterior (b) views of Twin A. Subtle lucency and capitellar subchondral changes are seen (black arrows in (a) and (b)). Intra-articular loose bodies (white arrows in (a) and (b)) and joint effusion (white arrowhead in (a)) are present

Lateral (a) and anteroposterior (b) views of Twin B. Subtle lucency in capitellar subchondral bone is seen (black arrows in (a) and (b)). There is a small osteochondral fragment on the anterior portion of the distal capitellar surface (black arrowheads in (a) and (b)). There are also intra-articular loose bodies (white arrows in (a) and (b)) and joint effusion (white arrowhead in (a)). Early osteophyte formation is seen on the medial side of the ulna (curved black arrow in (b))
MRI was performed 3 months later using a 1.5T scanner (Siemens Symphony, Siemens Medical Solutions, Erlangen, Germany) with a standard flexible surface coil. Imaging was performed with the elbow in maximal extension. Coronal, axial, and sagittal T2 (TR 3000-5690/TE 107-110) and proton density (PD) (TR 3000-5690/TE 21-37) weighted spin-echo (SE) sequences with fat saturation were obtained with additional coronal T2 and PD SE sequences without fat saturation. Imaging matrix was 320 x 192-245, field of view ranged from 12 x 9 cm to 14 x 12.6 cm.
Twin A (Fig. 3) had cartilage defects, bone marrow edema, and osseous changes in the capitellum. Joint effusion and intra-articular loose bodies were also present. This twin had also osteophytes at the medial aspect of the elbow as an early sign of arthrosis.

MR images of Twin A. Coronal T2-weighted fat-suppressed spin echo (a), coronal PD spin echo (b), and sagittal T2-weighted fat-suppressed spin echo (c). Subchondral edema in the capitellum (white arrow in (a)) with overlying bony defects and cartilage defect of the capitellum (black arrows in (b) and (c)) are seen (Stage II) (15). There are loose bodies (white arrowhead in (a) and (c)) in the joint. On the ulnar side, osteophyte formation is recognized (white curved arrows in (a) and (b))
Twin B (Fig. 4) had joint effusion and intra-articular loose bodies. There were cartilage and osseous defects with surrounding edema in the capitellum. On the cartilage surface there was a small loose cartilaginous particle, as a hyperintense rim extending to the articular space on T2-w images surrounded it.

MR images of Twin B. Coronal T2-weighted fat-suppressed spin echo (a), coronal PD spin echo (b), and sagittal T2-weighted fat-suppressed spin echo (c). Subchondral bony defects in the capitellum (black arrow in (b)) with small T2 hyperintense rim surrounding the chondral lesion (white arrows in (b) and (c)) are seen. Loose bodies (white arrowheads in (a) and (b)) are both in the posterior joint recess and in the radiohumeral joint. Loose bodies and fluid insinuation between the osteochondritis dissecans lesion and parent bone are features of instability (Stage III) (15)
The right elbow arthroscopy was performed in lateral decubitus position with the forearm hanging freely over a bar. The anterior compartment was first examined through anterolateral and anteromedial portals, followed by posterior compartment viewing through posterolateral and posterior portals.
At arthroscopy, Twin A had a mild synovitis, and loose bodies were detected (Fig. 5). The articular surface of capitellum was soft without unstable cartilage or visible subchondral bone. There was fraying of the articular cartilage of the radial head but it was otherwise normal. Superficial damage was also seen on the articular cartilage of trochlea.
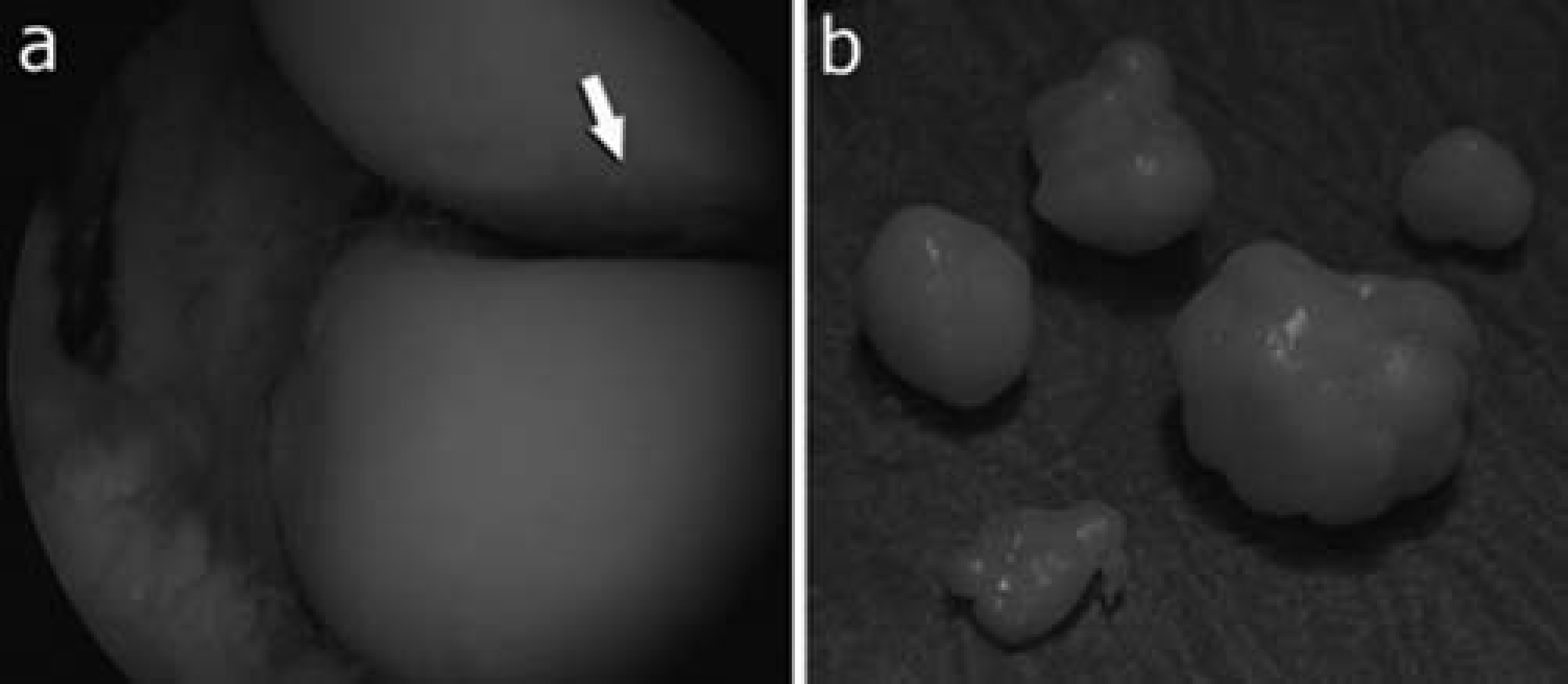
An anterolateral arthroscopic image of Twin A (a) showed slightly irregular surface of capitellum (white arrow in (a)). Removed osteochondral loose bodies (b)
Twin B also had mild synovitis and loose bodies (Fig. 6). There was softening of the cartilage on the articular surface of capitellum. Articular cartilage of the radial head was normal.

An anterolateral arthroscopic image of Twin B elbow (a) showed irregular surface of capitellum (white arrow in (a)), which was more severe than in Twin A. Some fraying is also seen in the radiocapitellar joint space (black arrow in (a)). Removed osteochondral loose bodies (b)
Discussion
The exact etiology of OCD of the capitellum is presently unknown, but repetitive trauma to the poorly vascularized capitellum is believed to be the primary cause (5). It should be noted that the word “osteochondritis” is a misnomer, as no inflammatory cells are present. OCD of the elbow almost always involves the anterolateral aspect of the capitellum, but there are some reports of OCD involving the trochlea, radial head, and olecranon (8, 10). The blood supply to the anterolateral aspect of the capitellum of the distal humeral epiphysis is weak and consists of end arterioles with no connection to adjacent metaphyseal vessels (5). In ice hockey the tensile stress placed on the medial aspect of the lower placed elbow during hitting the puck results in compressive forces between the radial head and the capitellum, potentially leading to osteochondrotic changes. Therefore, confounding factor in this case is the fact that both patients had a history of possible multiple microtrauma as both are right-handed ice hockey players.
This condition primarily occurs in the dominant elbow of young male baseball pitchers or less commonly in the elbow of young female gymnasts (2-4). Genetic factors have been thought to play a secondary role in the pathogenesis of the disorder. However, OCD patients in the same family (6, 7) and bilateral OCD (8, 9) have been reported, as well as identical knee lesions in identical twins (11).
Radiographs remain the imaging modality of first choice. Radiographs taken in the early stages of OCD may be normal or show only subtle changes in the capitellum. As the disease progresses, flattening of the contour, focal rarefaction, subchondral lucencies, and non-displaced fragmentation of the subchondral bone of the capitellum becomes evident. In the late stages, articular cartilage defects with loose bodies may be seen (12).
The disadvantage in radiographs, however, is its low sensitivity. Therefore, MRI is frequently used for detecting patients with early phases of OCD of the capitellum (13). Our MR protocol contained T2- and PD-weighted series with and without fat saturation. Also, T1-weighted images have been used to diagnose early OCD of the capitellum. Administration of intra-articular (i.a.) or intravenous (i.v.) contrast has been proven to be very useful (14). For i.a. contrast, if contrast insinuates between the OCD and parent bone, the lesion is unstable. Likewise, if there is contrast enhancement between the OCD and parent bone, the lesion is unstable. If there is no contrast enhancement at the interface of the OCD and parent bone, the lesion is stable. However, most centers like ours do not give i.v contrast for OCDs because often the non-contrasted images provide sufficient evidence whether OCDs are stable or unstable.
In conclusion, we present OCD of the capitellum in identical twins for the first time. Since these were identical lesions in identical twins, this supports the theory that OCD has a genetic background.