
Abstract
Hypertriglyceridaemia is an established cause of acute pancreatitis and responds to insulin therapy in addition to lipid lowering medication. We report a case of severe hypertriglycaeridemia of 149 mmol/L in a 36–year–old man with type 2 diabetes who presented to the surgical ward with abdominal pain due to pancreatitis and developed acute cholestasis, jaundice and eruptive xanthomata. His triglycerides improved to 3.8 mmol/L with sliding scale insulin within two weeks of in-hospital stay. However, his total cholesterol remained raised at 23.7 mmol/L. The lipoprotein electrophoresis confirmed the presence of lipoprotein X associated with bile obstruction, which contributed to an increase in total cholesterol. The total cholesterol normalized on improvement of his cholestasis.
Case
A 36–year–old Caucasian man was admitted to the surgical ward in this hospital with the third episode of acute on chronic pancreatitis in the previous six years. Two earlier such events were followed by recurrent complex pancreatic surgery. He also had a cholecystectomy performed for gallstones. The patient had an eight–year history of type 2 diabetes, poorly controlled by treatment with metformin and insulin (glycosylated haemoglobin [HbA1c] 12.5%, 113 mmol/mol) and a history of non-alcoholic steatohepatitis. Prior to the admission in order to control his lipid profile he had been on atorvastatin tablets for months but had run out of his medications and was off them for approximately eight weeks. He has never smoked and ceased drinking alcohol after the first episode of pancreatitis in 2005. His past history included self-administration of steroid and testosterone injections in the year 2000 for building muscle strength before participating in heavy-lifting competitions.
Physical examination revealed a body mass index of 32 kg/m2 and jaundice with hepatomegaly. There was no xanthelasma, arcus or tendon xanthomata, but there was a rash on his thighs - features consistent with the diagnosis eruptive xanthomata.
He had elevated blood levels of lipids: triglycerides of 149 mmol/L (reference range <1.7 mmol/L) and cholesterol of 31.3 mmol/L; blood glucose varied and fluctuated between 10 and 20 mmol/L. thyroid stimulating hormone was 1.7 mU/L. The liver function tests included alanine transaminase 92 U/L (0-45), γ-glutamyltransferase 149 U/L (0-55), total bilirubin 19 μmol/L (0-21) and alkaline phosphatase 151 U/L (40-130). Lipase was raised at 2803 U/L.
He was given one tablet of fenofibrate 160 mg but the liver function tests deteriorated the following day: alanine transaminase 249 U/L, γ-glutamyltransferase 1135 U/L, bilirubin 324 μmol/L and alkaline phosphatase 1154 U/L. The fenofibrate was stopped immediately. The patient was subsequently started on an insulin sliding scale that resulted in better sugar control and a significant reduction in triglycerides: 33.2 mmol/L and subsequently improved to 12.6 mmol/L after five days. His total cholesterol continued to be high (19.4 mmol/L) despite treatment with insulin and his blood glucose was in the normal range. The lipoprotein electrophoresis (Figure 1) showed the presence of lipopro tein X. A liver biopsy suggested non-alcoholic steatohepatitis and concluded that drug induced cholestasis could not be excluded.
The lipoprotein electrophoresis shows the presence of lipoprotein X (middle). Total cholesterol measured on the same sample was 23.7 mmol/L and triglycerides were 3.8 mmol/L. Total cholesterol was raised due to the presence of lipoprotein X. The lipoprotein electrophoresis pattern on the right confirms the disappearance of Lipoprotein X but shows staining at the origin suggesting presence of chylomicrons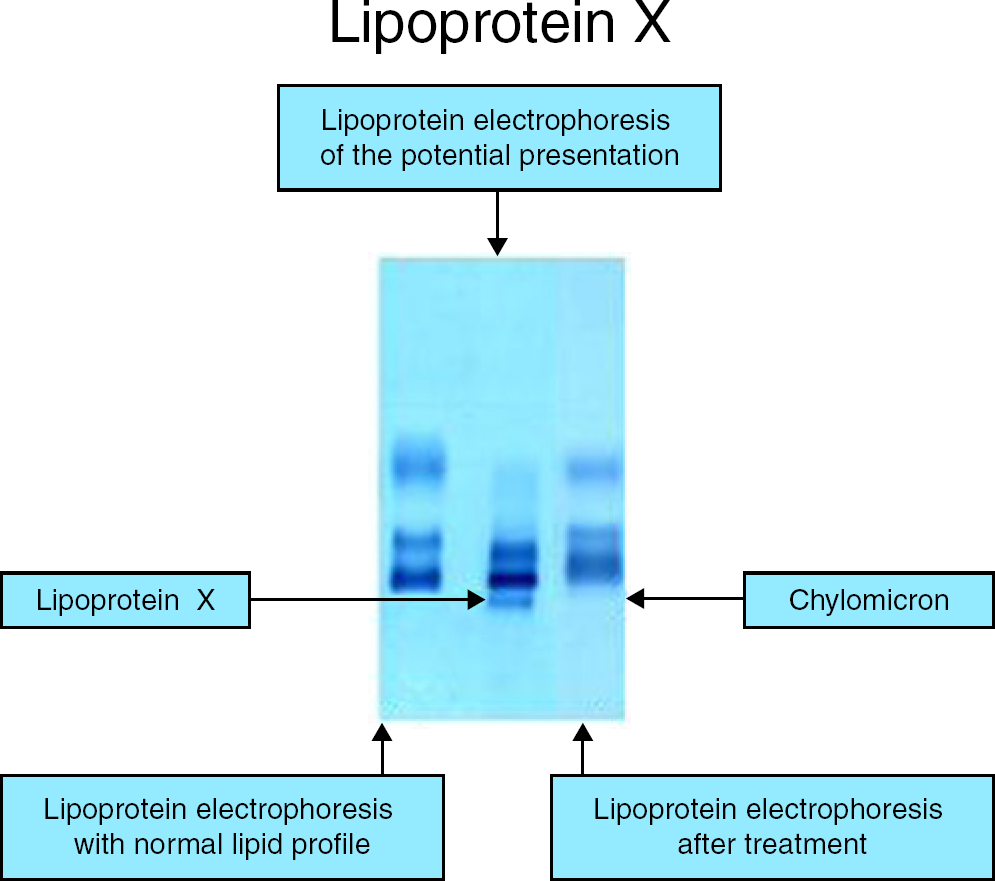
After three weeks of hospital stay and therapy with insulin, a low fat diet, fluid replacement and analgesia, the patient was discharged home.
Six weeks later, on his outpatient follow-up appointment in the Lipid Clinic, his total cholesterol remained raised at 23.7 mmol/L despite a fall in triglycerides concentration to 3.8 mmol/L. His Apo B was 1.5 g/L (0.6-1.3). Some of the liver function tests were still deranged (alanine transamin ase 424 U/L, bilirubin 194 μmol/L). γ-Glutamyltransferase and alkaline phosphatase were persistently high at 1546 and 1171 U/L. Patient was still jaundiced and has lost 10 kg in body weight since the last acute presentation. His abdominal pain had resolved and capillary glucose concentration were oscillating between 6 and 8 mmol/L with overall HbA1c of 4.7% (28 mmol/mol) on treatment with insulin: Lantus Solostar 25 units in the evening and Novorapid 30 units three times a day. The lipoprotein X later disappeared on improvement of his cholestatic picture (Figure 1) and his lipids normalized.
Discussion
We present a complex case of a patient with inadequate control of diabetes, hypertriglyceridaemia and cholestasis with the presence of lipoprotein X.
To our knowledge, this is one of very few reports of a case with a triglyceride value of 149 mmol/L. The most likely cause of the high triglycerides in this case is insulin resistance, obesity and no lipid-lowering medication for weeks preceding his acute presentation. Although we did not test the patient for lipoprotein lipase deficiency, the genetic abnormality is still very likely.
Hyperlipoproteinaemias types are recognized causes of up to 7% of all pancreatitis cases.1,2 In our patient, with no recent history of alcohol consumption, high triglycerides remain the likely cause of the pancreatitis. There is some evidence that cholestasis and biliary obstruction may be contributing to the hypertriglyceridaemia as well.1,3 Steroids, like many other drugs, have been documented to cause acute pancreatitis. 2 However, in view of the steroid use for only a short period of time and long before the first episode of pancreatitis, it is unlikely to have been a potential cause of pancreatitis. The effect of anabolic steroids on triglycerides is well known. 4 It has been suggested that relatively low doses do not affect the serum triglyceride concentrations, while it cannot be excluded that higher doses elicit an increase. The recent study by Morikawa et al. 5 showed that anabolic androgenic steroids may reduce the removal of plasma chylomicron remnants 5 that may potentially contribute to the high triglycerides concentration.
There are previously published reports of chronic pancreatitis-induced cholestasis, mainly in patients who abused alcohol. 6 Our patient had not consumed alcohol since the first episode of pancreatitis six years before but the hypothesis that the recurrent pancreatitis initiated the severe and long-lasting cholestasis cannot be excluded. It is noteworthy that fibrates have been documented to cause acute cholestatic hepatitis. 7 Our patient had already mildly deranged liver function tests on admission to the surgical unit which significantly deteriorated with the commencement of fibrates. Therefore, it is also possible that fibrates triggered the cholestasis, in the background of a chronic pancreatitis-induced cholestatic picture.
Lipoprotein X
Lipoprotein X is an abnormal lipoprotein that appears in the serum samples of patients with obstructive jaundice and is a marker of cholestasis.8–10 Lipoprotein X is primarily responsible for the unusual lipid composition and characteristic plasma lipid concentrations in obstructive jaundice.8,11
It is an intestinal lipoprotein catabolized rapidly in the liver and, therefore, largely undetectable in normal, fasting plasma, but accumulates in the plasma when the rate of degradation is reduced. 12 It has been reported that bile acids inhibit lipoprotein lipase - one of enzymes participating in the degradation of lipoproteins. 12
Lipoprotein X is a spherical particle that aggregates strongly. Phospholipids (66.5%) and unesterified cholesterol make up the bulk of lipoprotein X.9,11 Protein (5.8%), cholesterol esters and triglycerides make up 12% of the composition of the lipoprotein X. Intact lipoprotein X contains a protein moiety of a unique composition consisting of a mixture of albumin (approximately 40%) and the specific apolipoprotein ApoX (60%). The amino acid composition and the immunochemical characteristics of this lipoprotein X differs slightly from those of apolipoproteins A and B. 8 One important characteristic feature of lipoprotein X is its mobility toward the cathode on agar-gel electrophoresis13,14 that has been also noted on our patient's lipoprotein electrophoresis. Additionally, in our case Apo B has been only slightly raised above the reference ranges indicating that LDL containing Apo B has not contributed to the high concentration of total cholesterol. At the time of Apo B analysis, triglycerides have been only modestly raised suggesting that high concentration of total cholesterol has not been a result of raised VLDL. These findings strongly imply that high total cholesterol concentration was a consequence of the Lipoprotein X presence.
The plasma concentration of lipoprotein X is significantly correlated with the plasma activity of alkaline phosphatase and serum bilirubin, but seems to be superior to these two parameters in the differentiation between intrahepatic and extrahepatic cholestasis. 15 Lipoprotein X concentration above 400 mg/dL is highly indicative of extrahepatic biliary obstruction. 15 In our patient, although the presence of lipoprotein X was confirmed, the amount of the lipoprotein was not quantified. Therefore, it is not certain whether the intra-or extra-hepatic cholestasis resulted in the formation of lipoprotein X in this patient.
Interestingly, despite the highly-increased cholesterol concentration, bioactivities of lipoprotein X may be responsible for the phenomenon of decreased atherosclerosis. It has been documented that lipoprotein X prevents the origination of oxidized LDL products and thus reducing LDL atherogenicity.16,17 Moreover, the presence of lipoprotein X is a transient phenomenon and resolves with improvement in liver function tests. Thus, the effect of the lipoprotein X on atherosclerosis is negligible.
Noteworthily, apart from patients suffering from extra- or intra-hepatic cholestasis, lipoprotein X can be found in the rare inherited disease of lecithin cholesterol acyl transferase deficiency (LCAT). 18 Lipoprotein X has been also detected in the blood of patients with acute viral hepatitis, 19 drug-induced cholestatic hepatitis 20 and in patients with ischaemic stroke. 21
The effect of hypercholesterolemia and hypertriglyceri-daemia on the measurements of electrolytes has been well investigated. 22 Similarly, the presence of very high levels of lipoprotein X has been shown to be a rare cause of pseu-dohyponatraemia, 23 that we also noticed in our patient at the acute presentation. However, the sodium of 126 mmol/L (135-145) might have been a result of a combination of hyperglycaemia (19 mmol/L), hypertrigliceridae-mia and lipoprotein X.
Conclusion
This report highlights the importance of measuring triglycerides in cases with pancreatitis and the significance of using insulin for treatment. It also shows the benefits of lipoprotein electrophoresis as the total cholesterol continued to be high due to the presence of lipoprotein X.
Declarations
Footnotes
Acknowledgement:
We would like to thank laboratory technicians from Clinical Pathology Department at Nottingham University Hospitals Trust for providing us with the serum lipoprotein electrophoresis scans for this case report.