
Abstract
Background
High-dose vitamin A influences glucose and lipid profile; however, the possible effects of moderate doses (25,000 IU/d) are conflicting. We aimed to compare the effect of vitamin A supplementation on several anthropometric and biochemical variables between obese and non-obese women.
Methods
This study was performed on 84 women among whom 56 were obese (body mass index [BMI] 30-35 kg/m2) and 28 were non-obese (BMI 18.5-24.9 kg/m2). Obese women were randomly divided into two groups: one group received 25,000 IU/d retinyl palmitate and another group received placebo. The third group was age-matched non-obese women who received 25,000 IU/d retinyl palmitate. At baseline and four months after intervention, fasting blood glucose (FBG), lipid profile, C-reactive protein (CRP) and liver enzymes were evaluated.
Results
Baseline concentrations of serum FBG and triglyceride in the obese vitamin A-treated group were significantly higher compared with the other groups (P = 0.004 and 0.007, respectively). A significant increase in serum FBG (P = 0.026), total cholesterol (TC) (P = 0.004) and low-density lipoprotein cholesterol (LDL-C) (P = 0.016) in the non-obese group and a significant decrease in serum high-density lipoprotein cholesterol (HDL-C) (P = 0.001) in the obese group was observed. Serum CRP increased significantly in the obese vitamin A-treated group (P = 0.03) and serum aspartate transaminase increased significantly in the obese and non-obese groups after vitamin A supplementation (P = 0.008 and 0.001, respectively).
Conclusions
Treatment with 25,000 IU/d vitamin A induced a mild elevation in serum lipids, CRP and liver enzymes in obese and non-obese women. Considering the other information about possible side-effects of excess vitamin A, use of vitamin A in this dose and duration should be considered with caution.
Introduction
Vitamin A and its retinoid derivates are essential regulators of several biological processes such as normal growth, development, reproduction and apoptosis. 1 Retinoids are used as potent chemopreventive agents for prevention and treatment of number of cancers, dermatological and haematopoietic disorders.2–5 In developing countries, vitamin A deficiency is an important nutritional problem and women of reproductive age and young children are at greatest risk. 6 Vitamin A supplementation is associated with large reductions in child and maternal mortality7,8 and is an integral part of public health programs in developing countries. 9 In addition, vitamin A has important roles in adipose tissue biology; it has been estimated that 10–20% of total body retinoids are stored in the adipose tissue. 10 Several animal models point to a relationship between vitamin A metabolism and adiposity, and it was reported that high-dose vitamin A supplementation led to a significant weight loss in obese compared with non-obese mice. 11 Similar results were reported by Berry and Noy. 12 However, the effect of vitamin A supplementation on body weight or metabolic parameters in human obesity has not yet been evaluated.
A disadvantage of vitamin A and its synthetic forms is that they cause adverse effects such as hepatotoxicity 13 and elevation in serum triglyceride (TG). 14 . The adverse effects of high doses of vitamin A have been well documented; however, the information about adverse effects of moderate doses (25,000 IU/d) in human are scarce and conflicting. In a pilot study by Goodman et al., 16 supplementation with 25,000 IU/d retinyl palmitate for a median of 1.5 y had no adverse effects in healthy subjects; whereas, Cartmel et al. 14 observed a significant increase in serum triacylglycerol and serum cholesterol in a randomized controlled trial of 25,000 IU/d retinyl palmitate given for a median of 3.8 y in a population at moderate risk of skin cancer.
The present study was designed to evaluate the possible effects of four-month vitamin A supplementation on several common biochemical and anthropometric parameters in healthy obese and non-obese women of reproductive age.
Materials and methods
Subjects
A four-month, randomized, double-blind, placebo-controlled trial was carried out on 84 healthy women, among whom 56 were obese (body mass index [BMI] 30-35 kg/m2) and 28 were non-obese (BMI 18.5-24.9 kg/m2). The sample collection period was between 22 May and 23 July 2010. Inclusion criteria were as follows: 20-52 y of age, BMI 30-39.9 kg/m2 for obese and 18.5-24.9 kg/m2 for non-obese women. Exclusion criteria included a history of diabetes, thyroid abnormalities, liver or renal disease and autoimmune disease, consumption of any dietary vitamin A supplements or treatment with drugs that may interfere with absorption or bioavailability of the supplement. Obese women were randomly divided into two groups: one group received 25,000 IU/d (∼7576 retinol equivalent/d) retinlyl palmitate and another group received placebo. The third group was an age-matched non-obese group who received 25,000 IU/d retinyl palmitate. The proposed time for taking the supplement was immediately after breakfast. Vitamin A and placebo softgels were indistinguishable and were packaged in identical bottles each containing 120 capsules. The subjects were advised to avoid pregnancy and to maintain their usual diet and physical activity during intervention period. The study period was four months and a monthly follow-up procedure was done with telephone contacts to ensure that subjects consumed the supplement regularly. Subjects with irregular use of the supplement were excluded from the study. Full-informed written consent was obtained from all of the participants, and the ethics committee of Tehran University of Medical Sciences (TUMS) gave ethical approval for the study.
Dietary assessment
Dietary intake was assessed by a three-day 24-h dietary recall questionnaire (including a weekend day) at baseline and at the end of the four-month trial and was analysed by the Nutritionist IV software program (N-squared Computing, Salem, OR, USA). Since, in the obese individuals, dietary intake of special nutrients are strongly associated to total energy intake, dietary vitamin A intake was adjusted for total energy intake by residual method. 17
Biochemical assays
Venous blood samples were collected from all participants at the entry to the study and four months after intervention. The blood samples were centrifuged and serum was extracted. Sera were stored at -70°C until the assay. Serum fasting blood glucose (FBG) was measured by the glucose oxidase-peroxidase (GOD-POD) method using a kit (Pars Azmoon, Tehran, Iran). Total cholesterol (TC), TG and high-density lipoprotein cholesterol (HDL-C) were analysed by an enzymatic colorimetric method (Pars Azmoon). Mean inter- and intra-assay coefficients of variation (CV) were <1.19% and <1.74% for FBG; <1.22% and <0.62% for TC; <1.60% and <1.82% for TG; and 1.8% and <0.82% for HDL-C, respectively. Serum low-density lipoprotein cholesterol (LDL-C) was determined by the Friedwald formula: LDL-C = TC - (HDL-C + TG/5). 18 The relative percentile change of biochemical variables was calculated as: baseline level - follow-up value divided by baseline level. Serum high-sensitivity C-reactive protein (hs-CRP) was measured by enzyme-linked immunosorbent assay method (DRG Instruments GmbH, Marburg, Germany). Mean inter- and intra-assay CV for hs-CRP were <4.1% and <7.5%, respectively.
Serum aspartate transaminase (AST) and alanine transaminase (ALT) concentrations were also determined by enzymatic methods (Kits from Pars Azmoon). Mean inter-and intra-assay CV for these tests were 4.40, 3.25 and 3.08, 6.22, respectively.
Statistical analysis
Data processing and statistics were performed by SPSS software (version 17; SPSS Inc., Chicago, IL, USA). All data were presented as mean ± SEM. Kolmogorov–Smirnov test was applied to test normality of distribution. All the data were normally distributed; therefore, comparison of variables between groups was performed by one way analysis of variance for parametric data using a Tukey's post hoc test for multiple comparisons. Paired t-test was performed to determine the effect of intervention on anthropometric and biochemical variables. All statistics were two-tailed and a P value less than 0.05 was considered significant. Sample size calculation was performed based on 80% power and an α-error of 5% to detect treatment effect of vitamin A on serum TG.
Results
During the four-month treatment period, a total of nine women (10.71%) withdrew from the study. In obese groups, there were six withdrawals with irregular use of supplement or placebo (n = 3), impossibility to be present at appointment (n = 2) and unwillingness to continue the trial (n = 1). Three withdrawals were in the non-obese group (one pregnancy and two irregular use of supplement). A total of 75 women completed the study. As shown in Table 1, there was no effect of vitamin A on anthropometric variables. There was no significant difference between dietary energy, macronutrients and vitamin A intakes in treatment groups before and after intervention (Table 2). Table 3 shows the biochemical variables of study subjects before and after intervention. Baseline concentrations of serum FBG and TG in the obese vitamin A-treated group were significantly higher than the other groups (P = 0.004 and 0.007, respectively); while there was no statistically significant difference between the groups in their initial concentrations of serum TC, LDL-C, HDL-C and liver enzymes. The concentrations of serum FBG, TC and LDL-C increased significantly in the non-obese group after vitamin A supplementation (P < 0.05); while serum HDL concentrations reduced significantly in the obese groups. There was also a significant increase in serum CRP concentrations in the obese vitamin A-treated group (from baseline concentrations of 4.55±to 6.24±1.21 mg/L, P = 0.03). Serum AST concentrations increased in the obese and non-obese groups after vitamin A supplementation (P = 0.008 and 0.001, respectively); serum ALT concentrations did not change significantly after intervention.
Anthropometric characteristics of three treatment groups before and after intervention
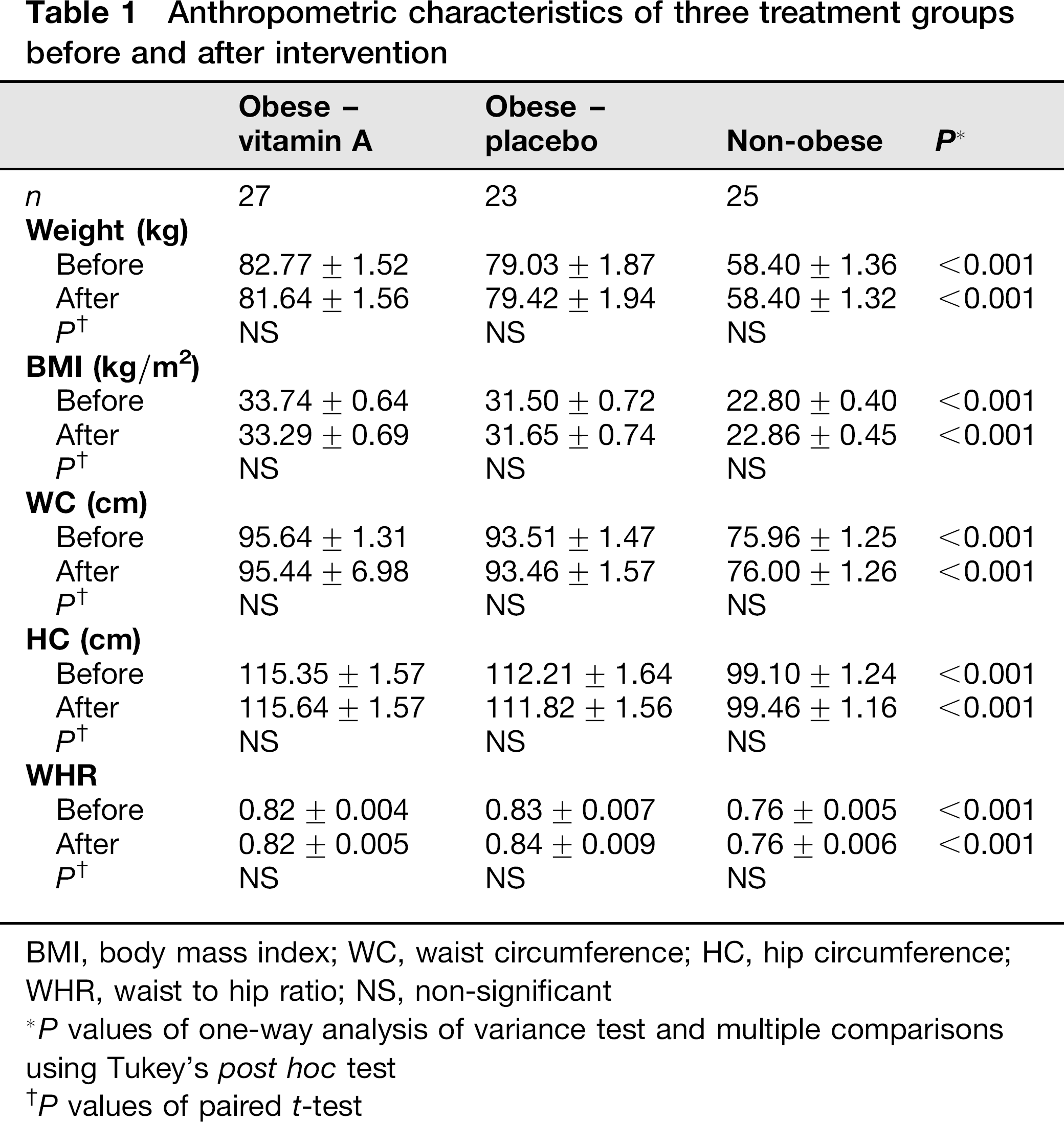
BMI, body mass index; WC, waist circumference; HC, hip circumference; WHR, waist to hip ratio; NS, non-significant
P values of one-way analysis of variance test and multiple comparisons using Tukey's post hoc test
P values of paired t-test
Dietary intake of energy and nutrients in three treatment groups before and after intervention
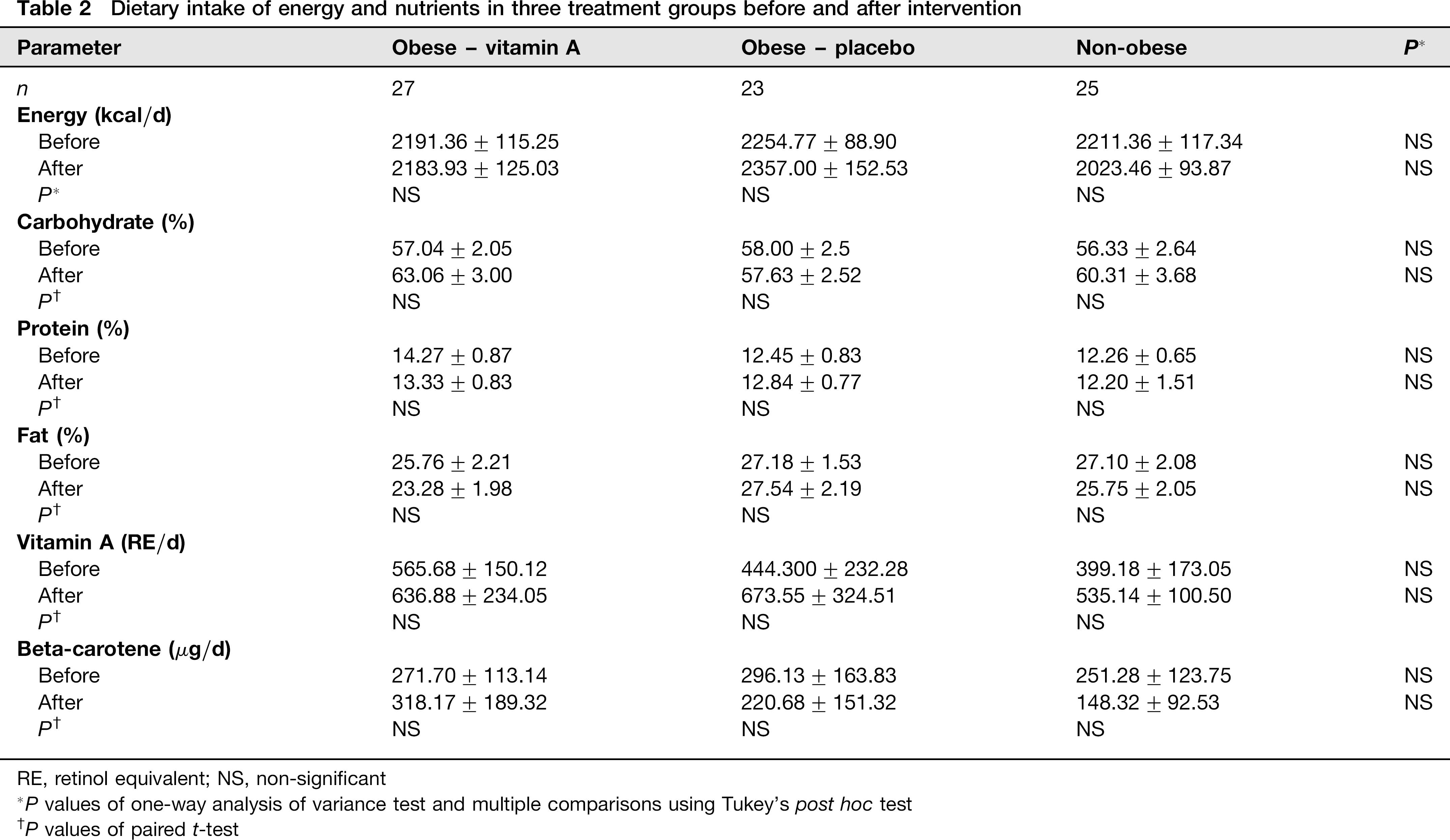
RE, retinol equivalent; NS, non-significant
P values of one-way analysis of variance test and multiple comparisons using Tukey's post hoc test
P values of paired t-test
Biochemical variables in three treatment groups before and after intervention
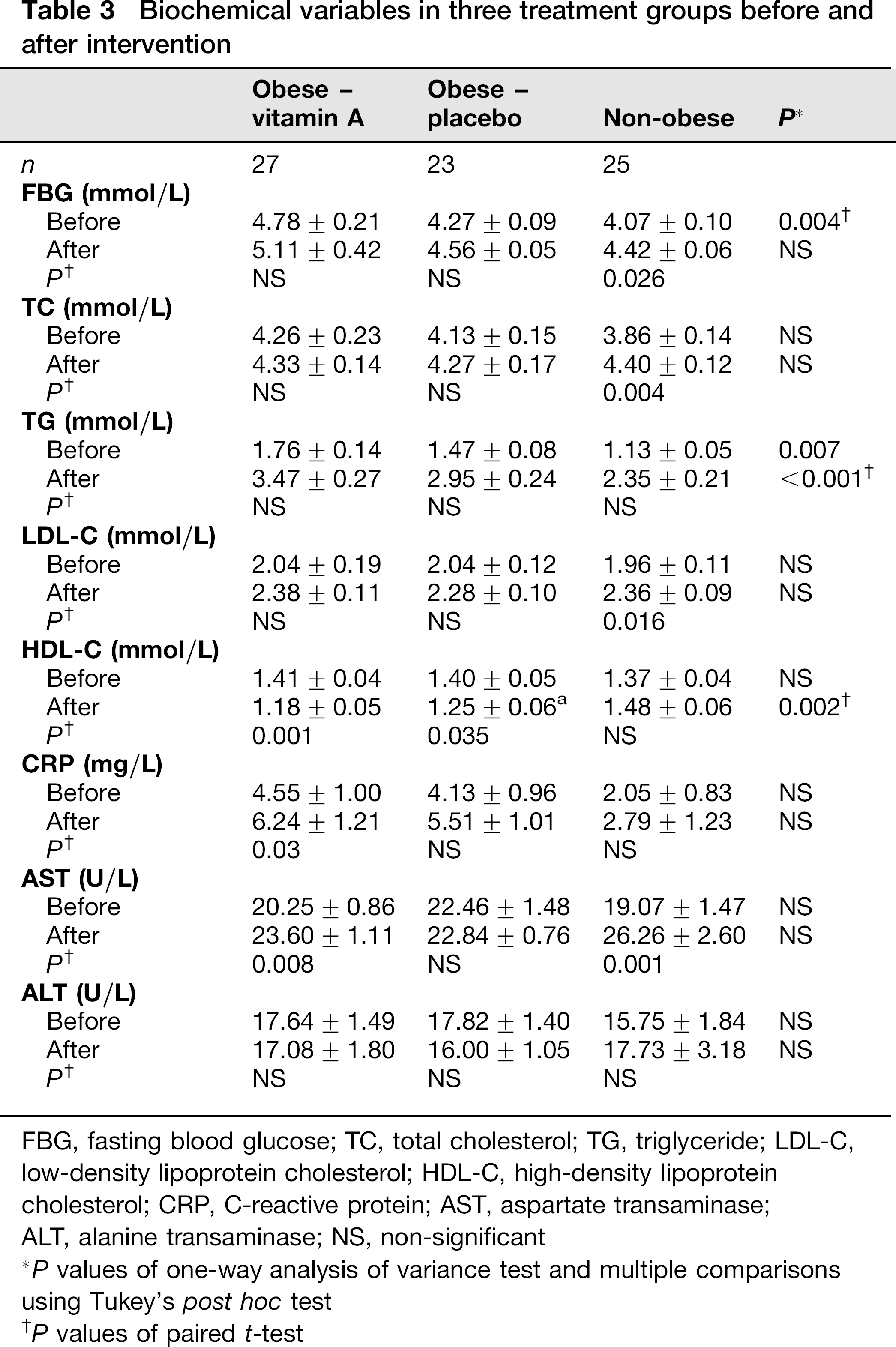
FBG, fasting blood glucose; TC, total cholesterol; TG, triglyceride; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; CRP, C-reactive protein; AST, aspartate transaminase;
ALT, alanine transaminase; NS, non-significant
P values of one-way analysis of variance test and multiple comparisons using Tukey's post hoc test
P values of paired t-test
Since the difference in baseline concentrations of FBG and TG between the obese vitamin A-treated group and other groups may affect the results, we also analysed the relative percentile change in biochemical variables between groups. The relative percentile changes of serum biochemical variables, which takes the initial values of parameters into account, were statistically significant for HDL-C (P < 0.01) and AST concentrations (P < 0.05, Table 4). When multiple comparisons were performed by Tukey's post hoc analysis, the relative change in serum HDL-C in the non-obese group was more pronounced than the other two groups; whereas, the relative change in AST was higher in the non-obese compared with the obese placebo-received group.
Comparison of the relative changes (%) in biochemical variables after 4 months in three treatment groups
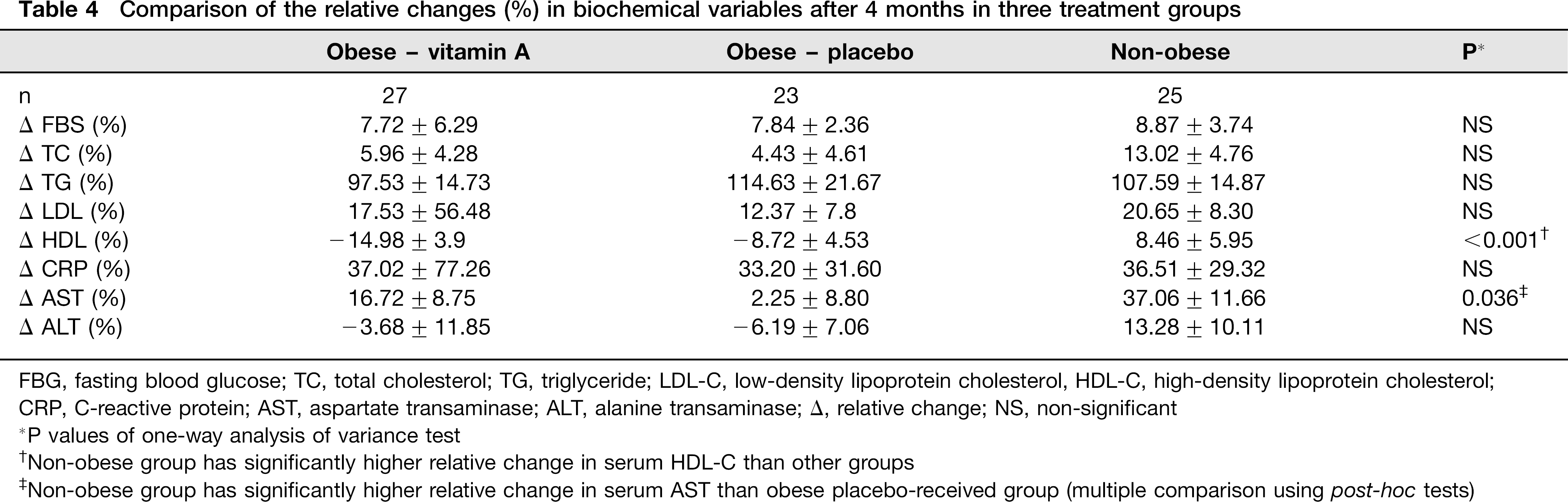
FBG, fasting blood glucose; TC, total cholesterol; TG, triglyceride; LDL-C, low-density lipoprotein cholesterol, HDL-C, high-density lipoprotein cholesterol;
CRP, C-reactive protein; AST, aspartate transaminase; ALT, alanine transaminase; Δ, relative change; NS, non-significant
P values of one-way analysis of variance test
Non-obese group has significantly higher relative change in serum HDL-C than other groups
Non-obese group has significantly higher relative change in serum AST than obese placebo-received group (multiple comparison using post-hoc tests)
Discussion
This interventional study demonstrates that vitamin A supplementation significantly increased serum FBG, TC, LDL-C and AST concentrations in non-obese and serum CRP and AST concentrations in obese women. Serum HDL-C concentrations were also significantly decreased in obese women after vitamin A supplementation. These findings were in agreement with the findings of Cartmel et al. 14 and Omenn et al. 19 Synthetic retinoids have also been reported to cause an increase in fasting serum glucose, TG, TC and LDL-C and a concomitant decrease in HDL-C.20,21 There are several mechanisms that could explain these findings. Vitamin A and its retinoid derivates enhance phosphoenolpyruate carboxykinase gene transcription and glucose production by hepatocytes.22,23 It has also been shown that vitamin A enhances hepatic production of apoprotein C-III. This protein prevents very-low-density lipoprotein (VLDL) from binding to the surface of endothelial cells of blood vessels and delays their lipolysis by lipoprotein lipase. This ultimately leads to higher serum TG concentrations. 24 Virtually, most plasma LDL is derived from VLDL particles, 25 suggesting the possible reason for serum LDL-C elevation due to vitamin A supplementation in our study.
Vitamin A-induced decrease in serum HDL-C in obese women in our study, consistent with previous reports by Corbetta et al. 1 and Cartmel et al., 14 can be attributed to the downregulatory effect of retinoids in apolipoprotein A-I gene expression in hepatocytes. 1
Serum CRP concentrations increased significantly in the obese vitamin A-treated group. This result was similar to the finding of Filteau et al., 26 who reported increased serum CRP concentrations after supplementation with 200,000 IU/d retinyl palmitate for four months in children of areas with marginal vitamin A deficiency. Accordingly, synthetic retinoids have also been shown to increase serum acute phase proteins such as CRP. 27 It has been suggested that the elevation is due to the increased production of CRP in the liver or increased responsiveness of acute phase proteins to major inducer cytokines such as interleukin-6.26,27 However, it should be remembered that in our study, the increase in serum CRP concentrations is clinically insignificant and there was also a similar but non-significant increase in the obese control group.
Higher baseline concentrations of serum FBG and TG in obese women in our study, consistent with previous reports, suggest that obesity is associated with abnormal metabolic profile and dyslipidaemia.28–30 Serum AST concentrations significantly increased in the vitamin A-treated groups but not in the placebo group (P < 0.01). This finding agrees with that of Geubel et al. 31 Although the elevation in AST activity in our study was in the accepted reference intervals for liver enzyme activity and cannot be considered as vitamin A hepatotoxicity, hypervitaminosis A is usually identified as serum retinyl esters >10% of total plasma vitamin A. 32 This early accumulation, associated with elevation in liver enzymes activity, occurs even before the appearance of clinical symptoms of liver damage and thus can be an early indicator of potential vitamin A toxicity. 33
We found no effects of vitamin A on anthropometric variables in study groups. Several previous studies reported that vitamin A represses obesity.11,12 However, these studies were in animal models and the inconsistency of their results with the present study may stem from this point.
It is worth noting that even after intervention, all of our biochemical parameters were in their physiological ranges. Besides, a decrease in HDL-C was seen in the placebo group, suggesting that other metabolic or environmental factors such as change in season may contribute in the alteration in glucose or lipid metabolism during intervention.
In summary, we have demonstrated that four-month treatment with 25,000 IU/d retinyl palmitate induced a physiologically mild and clinically insignificant change in serum lipids and liver enzymes. However, considering the other information about possible side-effects of excess vitamin A on cardiovascular disease, diabetes and serum lipid concentrations, use of vitamin A supplement in this dose and duration should be used with caution in further investigations.
Declarations
Footnotes
Acknowledgements
We are grateful for the supply of vitamin A and placebo softgels from Zahravi Pharmaceutical Inc., Tabriz, Iran. We thank all the participants in this study.