
Abstract
Background
Familial hypercholesterolaemia (FH) is an inherited disorder characterized by increased serum low-density lipoprotein (LDL)-cholesterol concentrations and premature atherosclerotic cardiovascular disease. The majority of people with FH are currently undiagnosed. We sought to determine the ability of a community laboratory to screen for individuals with potential FH.
Methods
Serum LDL-cholesterol concentrations issued by a private community laboratory in Western Australia were reviewed over a one-year period (1 May 2010 to 31 April 2011). We assessed the prevalence of possible FH based on LDL-cholesterol thresholds employed by the Make Early Diagnosis-Prevent Early Death (MED-PED), the Simon Broome Registry and the Dutch Lipid Clinic Network criteria.
Results
During this period, 84,823 people had 99,467 serum LDL-cholesterol measurements, with 91.8% requested by general practitioners. A secondary cause of hypercholesterolaemia was identified in 8.3% of subjects with an LDL-cholesterol ≥5.0 mmol/L. The prevalence of FH based on an LDL-cholesterol ≥6.5 mmol/L, the 99.75th percentile, was 1:398 in this sample population; similarly, the MED-PED LDL-cholesterol criteria gave a prevalence of 1:482.
Conclusions
The community laboratory is well placed to screen opportunistically for subjects with potential FH. This may be achieved using either the MED-PED criteria or a serum LDL-cholesterol cut-off point of ≥6.5 mmol/L, irrespective of age. Further investigation is required to determine the most effective method of identifying these individuals and, thereby, ensuring referral to a specialist lipid clinic.
Introduction
Familial hypercholesterolaemia (FH) is a co-dominantly inherited condition characterized by increased low-density lipoprotein (LDL)-cholesterol, xanthomata and premature atherosclerotic cardiovascular disease (CVD). 1–4 Lipid-lowering drugs decrease atherosclerosis progression and reduce the risk of premature cardiovascular events in FH. Although FH fulfils the World Health Organization criteria for systematic screening, few countries, to date, have implemented screening programmes. 5,6 As such, the vast majority of people with FH in Australia are currently undiagnosed, and those who are diagnosed (∼20%), are often inadequately treated. 7,8
Although a variety of screening options for FH are available, cascade screening – testing relatives of FH patients – is the most cost-effective approach to identify people with FH. 6,9 However, the current challenge is to detect the initial individual (the ‘index case’) in families with FH. 10 Currently, there are no internationally agreed diagnostic criteria for FH. Three main criteria exist: the Dutch Lipid Clinic Network (DLCN) criteria, the Simon Broome Registry criteria and the Make Early Diagnosis-Prevent Early Death (MED-PED) criteria. 11–13 All these criteria use cholesterol concentrations (LDL-cholesterol and/or total cholesterol), although cholesterol alone is usually not adequate to appropriately diagnose FH. Moreover, considerable overlap exists between LDL-cholesterol concentrations in FH patients and the general population. 14
Community laboratories perform large volumes of cholesterol testing, usually requested by general practitioners. We sought to determine the ability of a community laboratory to opportunistically screen for individuals at high risk for FH.
Methods
Serum LDL-cholesterol concentrations were reviewed over a one-year period (1 May 2010 to 30 April 2011) from St John of God Pathology, a private community laboratory in Western Australia providing services for ∼500,000 people. All serum LDL-cholesterol requests were included, with no exclusion criteria. This study protocol was approved by the Royal Perth Hospital Human Research Ethics Committee, and used anonymous data. We sought to determine the prevalence of possible FH based on LDL-cholesterol thresholds employed by the three commonly used diagnostic criteria: the MED-PED, the Simon Broome Registry and the DLCN criteria. 11–13
Potential secondary causes of hypercholesterolaemia (hypothyroidism [thyroid-stimulating hormone, TSH >4.0 mU/L], mixed hyperlipidaemia [triglyceride >4.0 mmol/L], nephrotic syndrome [proteinuria >3g/L and serum albumin <30 g/L] and cholestasis [alkaline phosphatase, ALP >135 U/L and γ–glutamyltransferase, GGT >55 U/L in men or >38 U/L in women]) were sought within ±30 days of the LDL-cholesterol result. To estimate the prevalence of altered glucose homeostasis, fasting serum glucose and glycated haemoglobin (HbA1c) were also sought within ±30 days of the serum LDL-cholesterol result. Diabetes was defined as a serum glucose ≥7.0 mmol/L or an HbA1c ≥6.5% (48 mmol/mol).
Total cholesterol, triglyceride and high-density lipoprotein (HDL)-cholesterol analyses were performed with enzymatic, colorimetric assays using Siemens reagents on a Siemens Dimension RXL chemistry analyser (Siemens Healthcare Diagnostics, Tarrytown, NY, USA). LDL-cholesterol was calculated according to the Friedewald equation. 15 For lipid assays, the inter- and intra-assay % coefficients of variation (%CVs) were <5%. TSH was performed on the Siemens Advia Centaur XP (Siemens Healthcare Diagnostics). ALP, albumin and GGT were measured on the Siemens Dimension RXL. HbA1c was measured on the Primus Ultra, using boronate affinity high-performance liquid chromatography (Trinity Biotech, Kansas City, MO, USA).
The laboratory database was searched with Crystal Reports Software version 11.0.0.1282 (Business Objects, SAP AG, Walldorf, Germany) and Microsoft Access 2003. Statistical analysis was performed using Microsoft Excel 2003 and simple interactive statistical analysis. 16 If more than one serum LDL-cholesterol was performed in this period, prevalence data were calculated based on the highest concentration.
Results
Over the one-year period, 99,467 serum LDL-cholesterol results were reported on 84,823 people. General practitioners requested 91.8% and cardiologists requested 3.2%, with the remaining 5.0% requested by other specialists. The serum LDL-cholesterol distribution is shown in Figure 1. The median and mean serum LDL-cholesterol concentrations were 3.0 and 3.1 mmol/L, respectively. The 95th, 99th and 99.75th percentiles for serum LDL-cholesterol were 4.8, 5.7 and 6.5 mmol/L, respectively.
Plasma LDL-cholesterol distribution in a community laboratory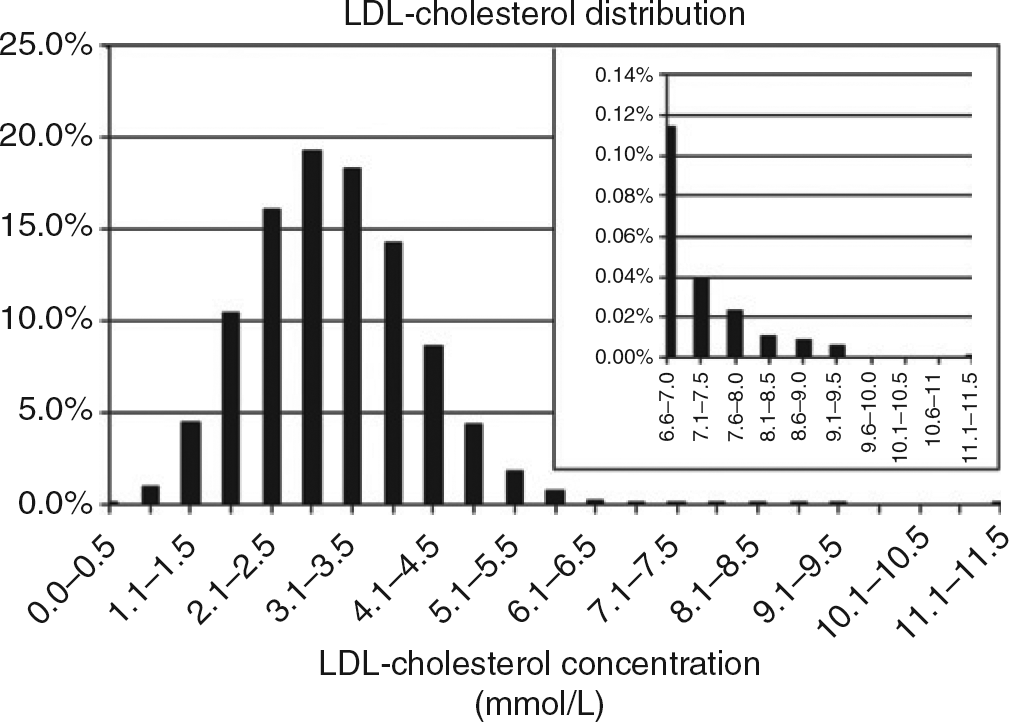
There were 43,455 (51.2%) LDL-cholesterol measurements performed in women (mean age 56 ± 15 y; range 3–101 y) and 41,386 (48.8%) in men (mean age 56 ± 15 y; range 3–99 y). In the 213 subjects with an LDL-cholesterol ≥6.5 mmol/L, there was a female predominance (144 women [mean age 55 ± 12 y; range 17–86 y] versus 69 men [mean age 51 ± 13 y, range 19–80 y]).
Potential FH prevalence based on MED-PED criteria
FH, familial hypercholesterolaemia; MED-PED, Make Early Diagnosis-Prevent Early Death
Potential prevalence of FH based on the LDL-cholesterol thresholds employed by the DLCN criteria
FH, familial hypercholesterolaemia; DLCN, Dutch Lipid Clinic Network
Potential FH prevalence based on LDL-cholesterol cut-off points
FH, familial hypercholesterolaemia
A potential secondary cause of hypercholesterolaemia was identified in 260 people (8.3%) with an LDL-cholesterol ≥5.0 mmol/L and in 25 people (11.7%) with an LDL-cholesterol ≥6.5 mmol/L. A fasting glucose or HbA1c was available on 74,391 (74.8%) of requests within ±30 days of the serum LDL-cholesterol result. In subjects with a LDL-cholesterol ≥6.5 mmol/L, a fasting glucose ≥7.0 mmol/L was present in 6.6% and an HbA1c ≥6.5% (48 mmol/mol) in 5.6% of subjects, with one or both of these conditions present in 8.5%.
Discussion
Our findings demonstrate that given the large number of serum LDL-cholesterol measurements requested in the community, primarily by general practitioners, the community laboratory is well placed to screen opportunistically for subjects with potential FH. Previous studies have suggested that individuals with a serum LDL-cholesterol ≥6.5 mmol/L have a high likelihood of FH. 17,18 Over a one-year period, we found 213 subjects with an LDL-cholesterol ≥6.5 mmol/L, equating to a prevalence of 1:398 in this sample population. FH is conventionally considered to have a population prevalence of 1:500 in Australia. 10 Thus, a serum LDL-cholesterol cut-off point ≥6.5 mmol/L, irrespective of the subject's age, gives a result close to the estimated prevalence of FH. However, exactly how many of these subjects will be confirmed to have FH after specialist review, remains to be determined.
The Simon Broome criteria rely on clinical features and a serum LDL-cholesterol of >4.9 mmol/L to diagnose FH in adults. However, our data suggest that this LDL-cholesterol threshold lacks specificity for FH, since an LDL-cholesterol >4.9 mmol/L yielded a prevalence of FH in this sample population of 1:27 people, almost 20 times that predicted in an unselected community sample.
The age-adjusted serum LDL-cholesterol criteria employed by MED-PED identified 176 subjects with possible FH, equating to a prevalence of 1:482 in this sample population, very similar to the predicted population prevalence. Hence, the MED-PED criteria could be applied in a community laboratory to detect FH, although this would require specialized laboratory software to identify these subjects. A benefit of applying the MED-PED criteria is their ability to ascertain individuals at a younger age. The MED-PED criteria identified 25 subjects aged <30 years at high risk for FH; 18 of whom would not have been detected using an LDL-cholesterol threshold of ≥6.5 mmol/L.
The multiple LDL-cholesterol categories employed by the DLCN could be used to raise the likelihood of FH in a graded manner. However, the lower LDL-cholesterol categories would lack specificity. The LDL-cholesterol category of 6.5–8.4 mmol/L had a prevalence of 1:428 in this sample population, although it would also be important to include subjects with LDL-cholesterol of ≥8.5 mmol/L. Selecting an LDL-cholesterol cut-off point ≥6.5 mmol/L was more efficient and gave a prevalence of 1:398 in this sample population.
Our community laboratory provides diagnostic services for ∼500,000 people. Thus, ∼17% of this population had a serum LDL-cholesterol measured during the one-year period of study. Based on a population prevalence for FH of 1:500, we would predict ∼1,000 people to have FH in this sample population. A serum LDL-cholesterol cut-off point of ≥6.5 mmol/L identified 213 subjects who were likely to have FH, ∼20% of the predicted FH in this sample population. Our findings emphasize the potential of a community laboratory in the detection of FH.
The mean age of our sample population was 56 y, with 12.8% aged less than 40 y, 4.4% aged less than 30 y and 0.9% aged less than 20 y, suggesting that routine CVD screening is occurring. Although younger adults and children are under-represented in our population, these subjects would be identified during the cascade screening process of relatives of index cases. The detection of index cases is one of the major challenges in FH. 10
The findings of our study should be generally applicable given the large community population, the lack of exclusion criteria and the fact that 92% of requests were from general practitioners. Furthermore, this community laboratory sample would appear representative of the general Australian population in that the 95th percentile for LDL-cholesterol of 4.8 mmol/L was very similar to the age- and gender-specific 95th percentiles from the AusDiab study (men 4.43 mmol/L and women 4.74 mmol/L), and that diabetes was not over-represented (G F Watts, personal communication). Potential secondary causes of hypercholesterolaemia were identified in a minority of subjects (8%), indicating that an LDL-cholesterol cut-off point alone could be applicable for detecting FH.
There are some limitations to using a community laboratory to screening for FH, as this represents a form of opportunistic screening of subjects referred for LDL-cholesterol testing, rather than the systematic screening of a population. Due to the large number of LDL-cholesterol measurements performed by this community laboratory, LDL-cholesterol is calculated rather than measured directly, which would exclude some, but not all patients with familial combined hyperlipidaemia. However, it could also exclude some subjects with FH and elevated triglyceride concentrations for another reason. 19 Given the considerable overlap in LDL-cholesterol concentrations of people with FH and the normal population, any LDL-cholesterol threshold suggesting high risk for FH is likely to have reduced sensitivity. 14 Subjects with lower LDL-cholesterol concentrations may be detected via cascade screening.
The practicalities and logistics of how the community laboratory can play an active role in highlighting potential index cases with FH remain to be elucidated. In the context of a high volume automated laboratory, identifying patients with an LDL-cholesterol of ≥6.5 mmol/L would be achievable with most laboratory information systems. The prevalence of LDL-cholesterol of ≥6.5 mmol/L (the 99.75th percentile) is such that it is possible for each case to be reviewed by a chemical pathologist, enabling individualized interpretation and advice on further testing and referral pathways. The interaction between the chemical pathologist and the requesting doctor will be a central aspect of this process, although this also requires further study to ensure it is performed in an efficient and effective manner. 20 Moreover, the best method of ensuring that subjects so identified are referred to a specialist lipid clinic remains to be determined. It is essential that any proposed system is able to be implemented in the context of a high volume, rapid turnaround laboratory, without necessitating large amounts of staff time.
Conclusions
We have shown that the community laboratory has the ability to screen opportunistically for subjects with potential FH. However, the proportion of these subjects who are subsequently confirmed to have FH after specialist review remains to be determined. Secondary causes were present in only a minority of cases, suggesting that a serum LDL-cholesterol cut-off point alone would be applicable for detecting FH. Further investigation is required to determine the most effective method of identifying these people and ensuring that they are referred for specialist review.
DECLARATIONS