
Abstract
Background
There is a need for practical, efficient and effective prognostic markers for patients admitted to the intensive care unit (ICU) with sepsis, to identify patients at highest risk and guide and monitor treatment. Although many biomarkers and scoring systems have been advocated, none have yet achieved this elusive combination. Most ICUs already use blood lactate concentrations to monitor patients but the evidence base for this application is unclear.
Methods
A systematic review of the last five years of evidence of effectiveness of lactate measurement in prediction of outcome in ICUs was performed.
Results
It was found that there is a lack of high-quality evidence, and no specific studies of prognostic accuracy.
Conclusions
The evidence reviewed suggested that whole blood, plasma or serum lactate measurement could not provide specific prognostic information for individual patients. There may be a role for monitoring for normalization of serum
Introduction
There is a need for effective prognostic markers for patients admitted to the intensive care unit (ICU) in order that appropriately aggressive therapy can be directed towards those that need it most. However, it remains the case that no single marker or combination has so far achieved the elusive requirement of clinical reliability, simplicity in everyday use and practicality.
There are a number of clinicopathological prognostic scoring systems such as the Acute Physiology and Chronic Health Evaluation score (APACHE), the Sequential Organ Failure score (SOFA) and the Simplified Acute Physiology score (SAPS). Each of these uses a complex scoring system involving clinical observations and physiological and laboratory measurements to construct a specific risk score for the individual patient. Prognostic scoring systems are complex and time-consuming to construct and require the use of specific software. Another drawback of some of the scoring systems (e.g. APACHE III) is that in more recent iterations, a license fee may be payable to the APACHE III license holder for the right to access and use the derived equation for calculation. In these circumstances, they therefore quickly become prohibitively costly for everyday use.
In addition to scoring systems, a plethora of biomarkers has been proposed, including cytokines, inflammatory proteins, serine proteinases, antiproteinases, matrix metalloproteinases, fibrinolytic enzymes and peptides and thrombolytic markers. All of those that have been evaluated so far have been either ineffective in predicting severity of outcome, or unable to be used in real time because methods of measuring them are not readily available on main laboratory platforms. More recently, a potential role for procalcitonin has been suggested, though recent evidence suggests that this marker may be best used in guiding antibiotic therapy rather than in the diagnosis of bacterial sepsis or prognostication.
There is a widely held view among intensivists in Britain and elsewhere, e.g. the Surviving Sepsis Campaign (
Objectives
There were two main objectives of this study:
To seek out published evidence of whether measurement of lactate at the time of admission in patients in intensive care settings is effective in predicting clinical outcome compared with clinical acumen, clinico-pathological scoring systems or other biochemical markers; To prepare a concise systematic review of the evidence.
Methods
Criteria for selecting studies for this review
The following types of studies were deemed acceptable: randomized controlled trials (RCTs), case-control cohorts and observational cohorts. The last five years of publications were considered to ensure the review was up to date and to avoid problems due to rapidly changing ICU practices and procedures. Studies published between 9 September 2005 and 9 September 2010 were included in the critical evaluations.
Studies with the following types of participants were accepted: those involving adult humans (we concluded that a paediatric review is warranted but should be conducted separately), studies with participants between 18 and 75 years of age and those studies with cohorts that included both male and female participants.
Measurement of
Comparisons were against the following reference tests: APACHE scoring, SOFA scores, SAPS scores, arterial pH and arterial PaO2.
The primary outcome measure was 28-day in-hospital mortality. The secondary outcome measure was multiple organ dysfunction syndrome.
Sources of heterogeneity included variable delay to first measurement and variations in severity of disease and case-mix, and each of these factors was considered during the critical appraisal process.
Search methods for identification of studies
The PubMed, MEDLINE and Embase Databases were searched on 15 September 2010 using the search criteria in Appendix A (please see
Data collection and analysis
All abstracts were reviewed for relevance by the group. Disagreements were resolved by discussion. When the group could not reach a consensus, one person was nominated (CC) to be the final arbiter. There was no meta-analysis.
The full text of all papers identified as relevant was formally reviewed using standard published methods. The quality of the papers was assessed using the Cochrane risk of bias tool (
Results
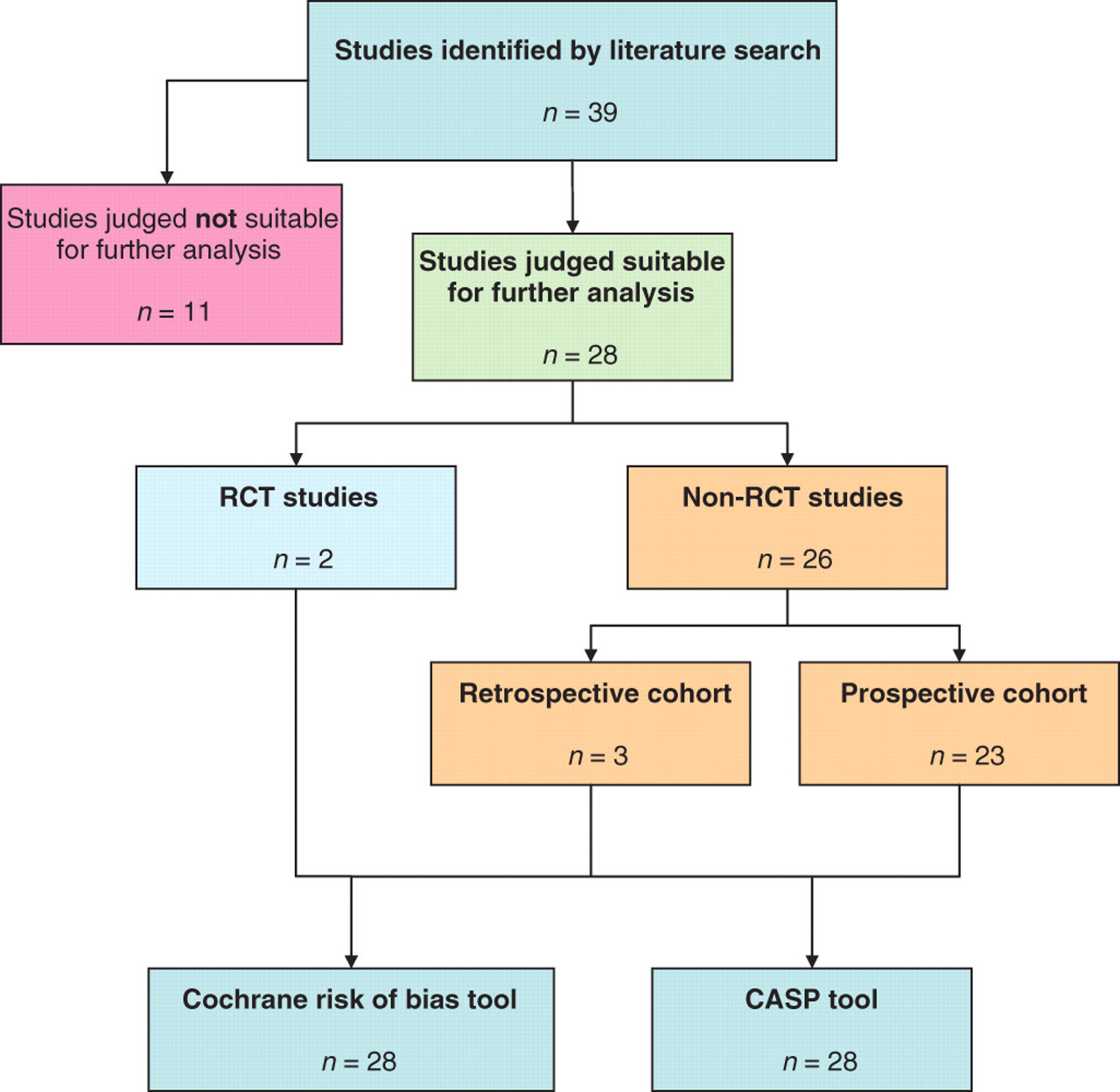
Using the search criteria described in Appendix A, a total of 39 studies 1–39 were identified. The number of studies found and the type of study is summarized in Figure 1.
Summary of literature include in the review
After review of the abstracts for each study, 11 studies
1,2,7,12,17,21,24,29,34–36
were immediately rejected as they were deemed not relevant. The citations for these papers are given in the references, and they are clearly identified. Full text papers of the remaining 28 studies
3–6,8–11,13–16,18–20,22,23,25–28,30–33,37–39
were obtained and reviewed as described. The results of the CASP and Cochrane Risk of Bias appraisals for each study are available in Appendix B, as an online supplementary file (please see
Types of study
There were two RCTs that evaluated diagnostic or prognostic accuracy of lactate measurement. 11,30 The majority 3,4,6,8–10,13,14,16,19,20,22,23,25–28,31,37–39 were prospective cohort trials (23 of 28 studies; 82%). There were three retrospective cohort studies. 15,32,33 Of the 11 papers rejected from further consideration, reasons for rejection included the fact that the study did not cover evaluation of lactate measurement or that the study cohort was recruited in the emergency department not the ICU or that the underlying clinical diagnosis in the study cohort was too narrow and therefore results were not generalizable. In the main, studies used lactate measurements as a comparator test rather than as the reference test.
Analyte and matrix
Twenty six of 28 studies considered
Interpretation
Serum
One study applied ROCC analysis to rate of decline in
The most common recommendation across all studies was to use normalization of serum
Conclusions and recommendations
We found a lack of good-quality studies of the use of admission lactate concentrations as a prognostic marker in the ITU setting. There were few RCTs, and the two RCT studies that we identified were not focused on lactate measurement.
The broad consensus of evidence from the studies that were reviewed was that there is an association between the highest serum
It was concluded that there is insufficient good-quality evidence to suggest that measuring admission serum
However, there was stronger evidence that patients may benefit if goal-directed therapy includes a target to return serum
There were too few studies using
DECLARATIONS