
Abstract
Background
There is growing epidemiological evidence linking serum 25 hydroxy-vitamin D (25(OH)D) concentrations to outcome in cardiovascular and other diseases. We have studied patients with acute myocardial infarction (AMI) to determine if they exhibit an acute phase reaction affecting 25(OH)D.
Methods
Patients (n= 32) with first AMI who had been treated with primary percutaneous coronary intervention within 12 h of symptom onset had venous blood samples taken two days, one week, one month and three months after presentation. Samples were analysed for troponin I, C-reactive protein (CRP) and 25(OH)D.
Results
All patients had significant rises in troponin confirming the myocardial damage and CRP, both of which resolved by 28 days. In contrast, 25(OH)D remained unchanged throughout the 90-day observation period with a median concentration of 46 nmol/L.
Conclusion
Serum 25(OH)D does not change after AMI and is likely to be a reliable marker of vitamin D status in patients with cardiovascular disease.
Introduction
There is growing epidemiological evidence linking serum 25 hydroxy-vitamin D (25(OH)D) concentrations to outcome in cardiovascular and other diseases. In particular, vitamin D deficiency is related to poor prognosis in coronary heart disease (CHD) and heart failure. 1 It has been proposed that lifestyle difference may be a predisposing cause; however, since atheroma is an inflammatory state, it is important to ascertain whether low 25(OH)D concentrations are part of the acute phase reaction. Vitamin D has a complex role in inflammation. Vitamin D itself appears to modulate the acute phase reaction as assessed by body temperature and C-reactive protein (CRP). 2 Inflammation itself then affects vitamin D since its major binding protein (Gc globulin) is increased by IL-6 and decreased by transforming growth factor beta in vitro. 3 Further, following tissue damage, Gc globulin binds to actin, which is then cleared by the reticulo-endothelial system. 4
Extensive evidence links acute myocardial infarction (AMI) with local and systemic inflammation. Inflammation is both a precursor of coronary plaque rupture, which leads to AMI as well as a consequence of acute infarction. While the correlation between several inflammatory markers such as CRP and AMI has been established, 25(OH)D has not been correlated with AMI.
The aim of this study was to determine the relationship, in the short to medium term, between 25(OH)D levels and the inflammatory response in a series of patients presenting with a first AMI. The patients were recruited as part of an existing cardiac magnetic resonance imaging (MRI) study.
Methods
We prospectively enrolled 48 patients with first presentation acute ST elevation myocardial infarction who were treated successfully with primary percutaneous coronary intervention (PPCI) within 12 h of symptom onset. Exclusion criteria included previous coronary re-vascularization (by either percutaneous coronary intervention or coronary artery bypass graft surgery), previous myocardial infarction, severe renal failure (defined as an estimated glomerular filtration rate <30 mL/min/1.73 m2) and any contraindication to MRI. No data were collected in relation to vitamin D supplementation. The study was approved by the institutional Research Ethics Committee and all participants gave written informed consent.
Venous blood samples were collected from each patient at two days, one week, one month and three months after index presentation. The blood was collected in serum separator tubes containing separating gel and clot activator. The samples were centrifuged within 30 min of collection. The separated serum was stored at −80°C. All of the samples were analysed as a single batch at the end of the study.
Troponin was measured with the Advia TnI-Ultra assay (Siemens Healthcare Diagnostics, Surrey, UK). The 99th centile value of healthy adults for this assay is 45 ng/L and the inter-assay coefficient of variation (CV) was 10% at 45 ng/L. CRP was measured by immunoturbidimetry on a Siemens Advia 2400. The intra-assay CV was 5% at 1.1 mg/L. Serum 25(OH)D2 and 25(OH)D3 were analysed by tandem mass spectrometry after protein precipitation. The inter-assay CV was <10% at all concentrations ranging from 13 to 80 nmol/L. 25(OH)D2 and D3 concentrations were summed and reported as 25(OH)D.
Analysis was performed using the Analyse-it add-in package (version 2.22) for Microsoft Excel (Analyse-it, Leeds, UK;
Results
Thirty-two patients were included as they had samples taken at all four times points. There were 27 men (median age 57 y [range 35–73]) and five women (median age 59 y [range 56–64]). One man was South Asian and all others were white Caucasians. The basal 25(OH)D concentration was 45.9 nmol/L (26.4–63.4) (median [25–75 centiles]) and 9 (28%) had a 25(OH)D<30 nmol/L. Patients were recruited through the calendar year: January to March (n= 7) baseline 25(OH)D was 24.6 (21.4) nmol/L (median [interquartile range, IQR]); April to June (n= 10) 25(OH)D was 39.6 (25.8); July to September (n= 9) 25(OH)D was 75.6 (31.2); and October to December (n= 6) 25(OH)D was 45.8 (33.0).
The troponin concentrations at day two were 30,100 (4200 to >50,000) ng/L (median [range]). The concentrations of CRP and 25(OH)D are shown (Figure 1). CRP shows typically high values at day 2 consistent with acute inflammation with a fall over the following weeks. In contrast, there are no differences in the concentrations of 25(OH)D at each time point (analysis of variance [ANOVA], P= 0.80). There was no relationship between CRP and 25(OH)D at any time point (Spearman rank correlation, P>0.4).
Changes in (a) C-reactive protein (CRP) and (b) 25(OH)D at the time points of 2, 7, 28 and 90 days post acute myocardial infarction. Data expressed as box and whisker plots showing 5, 25, 50, 75 and 95 centile values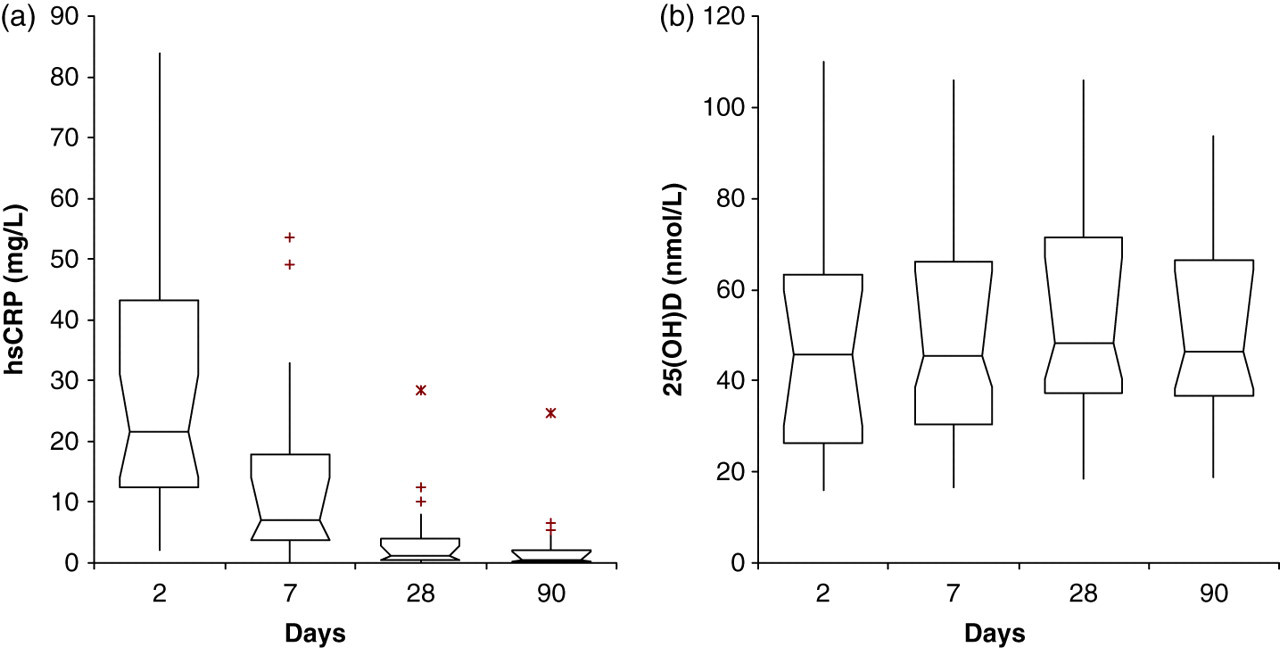
Discussion
In view of the considerable epidemiological evidence showing a relationship between serum 25(OH)D and poor outcomes in a number of varied medical conditions, it is essential to be certain whether 25(OH)D is affected by acute inflammation. Our data clearly show that despite the inflammatory response to AMI indicated by the rise and fall of CRP, there is no change in the levels of serum 25(OH)D.
There have been two conflicting reports of the effect of acute inflammation on circulating 25(OH)D. The first examined the changes in 25(OH)D during the acute phase of a malarial infection. 5 In this series, 14/49 subjects had 25(OH)D measurements made on samples during their acute admission to hospital and subsequently 2–6 weeks later. These subjects showed no change in serum 25(OH)D concentration and the authors proposed that no acute phase response was elicited. However, the undefined period of 2–6 weeks in the malaria study may have been too short to observe a real change in 25(OH)D, which has an elimination half-life of approximately 15 days. 6 A period of two weeks may not have been sufficiently long to demonstrate a fall in 25(OH)D. Moreover, the study by Newens et al. 5 did not report on the inflammatory state at the follow-up measurement.
The second study reported on 33 subjects following knee arthroplasty. 7 The 25(OH)D fell dramatically with a nadir at 1–2 days. There was a small rise to 75% of preoperative values by five days but little further improvement by three months when inflammation as measured by CRP had resolved. This period of follow-up and resolution of inflammation matches our study and represents six elimination half-lives of 25(OH)D which is long enough for a new 25(OH)D equilibrium. Reid et al. 7 excluded the possibility that the fall in 25(OH)D was due to inflammation, fall in vitamin D binding protein and iatrogenic dilution.
In summary, we have shown that there is no fall in 25(OH)D after acute myocardial infarction and that serum measurement may be assumed to be a reliable marker of vitamin D status in patients with cardiovascular disease.
DECLARATIONS