
Abstract
Background
Urinary C-peptide creatinine ratio (UCPCR) is a non-invasive and convenient way of assessing endogenous insulin production. Adjusting for urine creatinine levels allows for differences in urine concentration. Creatinine excretion is known to be higher in men due to gender differences in muscle mass. We investigated the impact of gender on UCPCR.
Methods
One hundred and seventy-six subjects underwent a mixed meal tolerance test (MMTT). We looked at the relationship between UCPCR on urine C-peptide and creatinine excretion rates using timed post-meal urine samples. A further 415 subjects had two-hour post-meal UCPCR measurements in order to derive gender-specific percentiles for different diabetes subgroups and controls.
Results
UCPCR was 1.48-fold higher in women (n= 78) than men (n= 98), median (interquartile range [IQR]): 1.88 (0.49–3.49) men versus 2.88 (1.58–4.91) nmol mmol−1 women, P= 0.01. This reflects a gender difference in creatinine excretion rates (11.5 [8.3–13.7] men versus 8.2 [5.6–9.1] women μmol min−1 P < 0.001). C-peptide excretion rate was similar in men and women (19.8 [5.2–37.0] versus 22.1 [7.4–40.5] pmol min−1, P = 0.7). UCPCR was higher in women in all subgroups defined by diabetes classification and treatment, except long-term type 1 diabetes in whom C-peptide secretion was minimal.
Conclusions
Gender affects UCPCR, with higher values found in women. This results from lower urine creatinine reflecting gender differences in muscle mass. This necessitates gender-specific ranges for accurate interpretation of UCPCR results.
Introduction
Urinary C-peptide creatinine ratio (UCPCR) is a novel convenient way to evaluate endogenous insulin secretion. UCPCR is calculated by dividing urinary C-peptide by creatinine concentration to account for variations in urinary concentration. It enables the use of a spot urine sample rather than a timed collection. C-peptide is a polypeptide secreted in equimolar quantities with insulin following enzymatic cleavage of pro-insulin in the B-cell. 1 C-peptide can be measured in insulin-treated patients and varies throughout the day depending on the extent of stimulation of insulin secretion. C-peptide is metabolized and excreted predominantly by the kidneys, with 5–10% excreted unchanged in the urine, offering the potential for urinary measurements. 2,3
UCPCR is highly correlated to stimulated serum C-peptide during a mixed meal tolerance test (MMTT) in type 1 and both insulin- and tablet-treated type 2 diabetes. 3–5 UCPCR has been shown to be reproducible and stable for 72 h at room temperature in boric acid preservative. 6 The main advantage of UCPCR over serum C-peptide is convenience. UCPCR can be collected in the patient's own home and posted directly for analysis, avoiding the need to attend hospital. Potential applications include differentiation between diabetes subtypes, hence assisting treatment decisions. 7
Creatinine excretion rate is fairly constant throughout the day, but is influenced by changes in gender, age and race. 8 Creatinine is a breakdown product of creatine phosphate in muscle and chiefly filtered out of the blood by the kidneys with little or no tubular reabsorption. Factors affecting its excretion arise directly through differences in muscle mass and resulting creatinine production.
When measuring the albumin creatinine ratio (ACR), there are gender-specific thresholds for microalbuminuria in patients with diabetes. These are 2.5 mg mmol−1 in men and 3.5 mg mmol−1 in women. 9,10 This gender difference is determined by creatinine, with significantly higher levels of urine creatinine in men but no significant gender differences in urine albumin concentration. 11 UCPCR uses creatinine concentration in a similar manner and could be expected to be higher in women due to lower urinary creatinine excretion rates.
The aim of this work was to determine if there were gender differences in UCPCR and whether this reflected differences in C-peptide or creatinine excretion rates.
Research design and methods
Our study was conducted in two stages. First, we quantified any gender difference in UCPCR and assessed if this reflected differences in timed excretion of urinary C-peptide or urinary creatinine. The second stage was to determine the impact of any gender difference on subgroups differentiated by diabetes diagnosis and treatment.
Quantifying the gender difference in UCPCR
Study population
One hundred and seventy-six patients (>99% Caucasian) with normal renal function (estimated glomerular filtration rate [eGFR] ≥ 60 mL/min/1.73 m2) were recruited (type 1 diabetes n= 58, type 2 diabetes n= 69 and non-diabetic controls n= 49).
Mixed meal tolerance urine collection
All individuals underwent a standard MMTT.
12
Patients emptied their bladder prior to the meal stimulus and then gave a sample after 120 min. Urine volume was recorded and C-peptide and creatinine concentrations were measured. This allowed calculation of C-peptide and creatinine excretion rates, as below:


Postprandial UCPCR centiles
Study population
Five hundred and ninety-one subjects (>99% Caucasian) were recruited (type 1 diabetes n = 130, type 2 diabetes n = 335, HNF 1A [hepatocyte nuclear factor 1 alpha] and HNF 4A [hepatocyte nuclear factor 4 alpha] n = 77 and controls n = 49), with eGFR ≥ 30 mL/min/1.73 m2. Type 2 diabetes was classified as diabetes diagnosed at 35 years or over, with over a year to treatment with insulin and a clinical diagnosis of type 2 diabetes. Type 1 was those aged under 35 years at clinical diagnosis of type 1 diabetes. Those within the HNF 1A/4A group had a molecular genetic diagnosis.
Urine collection
UCPCR was collected 120 min after a meal stimulus (MMTT n= 351, home largest meal of the day n= 240). Patients had emptied their bladder immediately prior to the meal and continued their normal treatment regimen.
Materials and methods
C-peptide analysis was undertaken on a routine analyser at the Biochemistry department at the Royal Devon and Exeter NHS Foundation Trust, Exeter, UK, using the Roche Diagnostics (Mannheim, Germany) E170 analyser (intra-assay coefficient of variation [CV] < 3.3%; inter-assay CV < 4.5%, functional sensitivity = 0.003 nmol L−1). The assay is a direct electrochemiluminescence immunoassay for human serum, plasma or urine. It is a two-site immunoassay employing monoclonal antibodies against human C-peptide, calibrated to WHO International Reference Reagent for C-peptide of human insulin for immunoassay (IRR code 84/510). 13
Urine creatinine was analysed on the Roche P800 platform using creatinine Jaffé reagent (standardized against isotope dilution mass spectrometry) to obtain a urine C-peptide creatinine ratio (nmol mmol−1) (intra- and inter-assay CV < 2.3%, functional sensitivity 0.36 mmol L−1). UCPCR was calculated as the ratio of urine C-peptide to creatinine, as previously described. 6
Statistical analysis
All the data were not normally distributed and therefore analysis was non-parametric. Differences between groups were calculated using the Mann-Whitney U test. Regression analysis was used to model the relationship between UCPCR and C-peptide excretion in each gender. Residuals were checked to ensure model assumptions were met, given the data were not normally distributed. The regression line was forced through the origin as zero C-peptide excretion should relate to zero UCPCR. This also enabled direct comparison of the β coefficients for the two genders to calculate the magnitude of any difference.
Results
Quantifying gender differences on UCPCR
The characteristics of the population by gender and diagnosis are listed in Table 1. Women had higher UCPCR values (Figure 1a), median (interquartile range [IQR]): women 2.88 (1.58–4.91) versus men 1.88 (0.49–3.49) nmol mmol−1, P= 0.01. Women had lower creatinine excretion rates (Figure 1b), 8.2 (5.6–9.1) versus men 11.5 (8.3–13.7) μmol min−1, P< 0.001, but similar C-peptide excretion rates (Figure 1c), 22.1 (7.4–40.5) versus men 19.8 (5.2–37.0) pmol min−1, P= 0.7.
The gender differences between (a) urinary C-peptide creatinine ratio (UCPCR), (b) creatinine excretion rates and (c) C-peptide excretion rates. Excretion rates were calculated from timed urine samples. Central horizontal line shows median and box shows interquartile range, Lines represent all values except those 1.5 standard deviations or more from the interquartile range which are represented by circles. P represents the overall differences between men and women as assessed by Mann-Whitney U test The baseline characteristics of the cohort of 176 by gender and general practitioner-classified diagnosis Data presented as median and interquartile range (IQR) HbA1C, glycosylated haemoglobin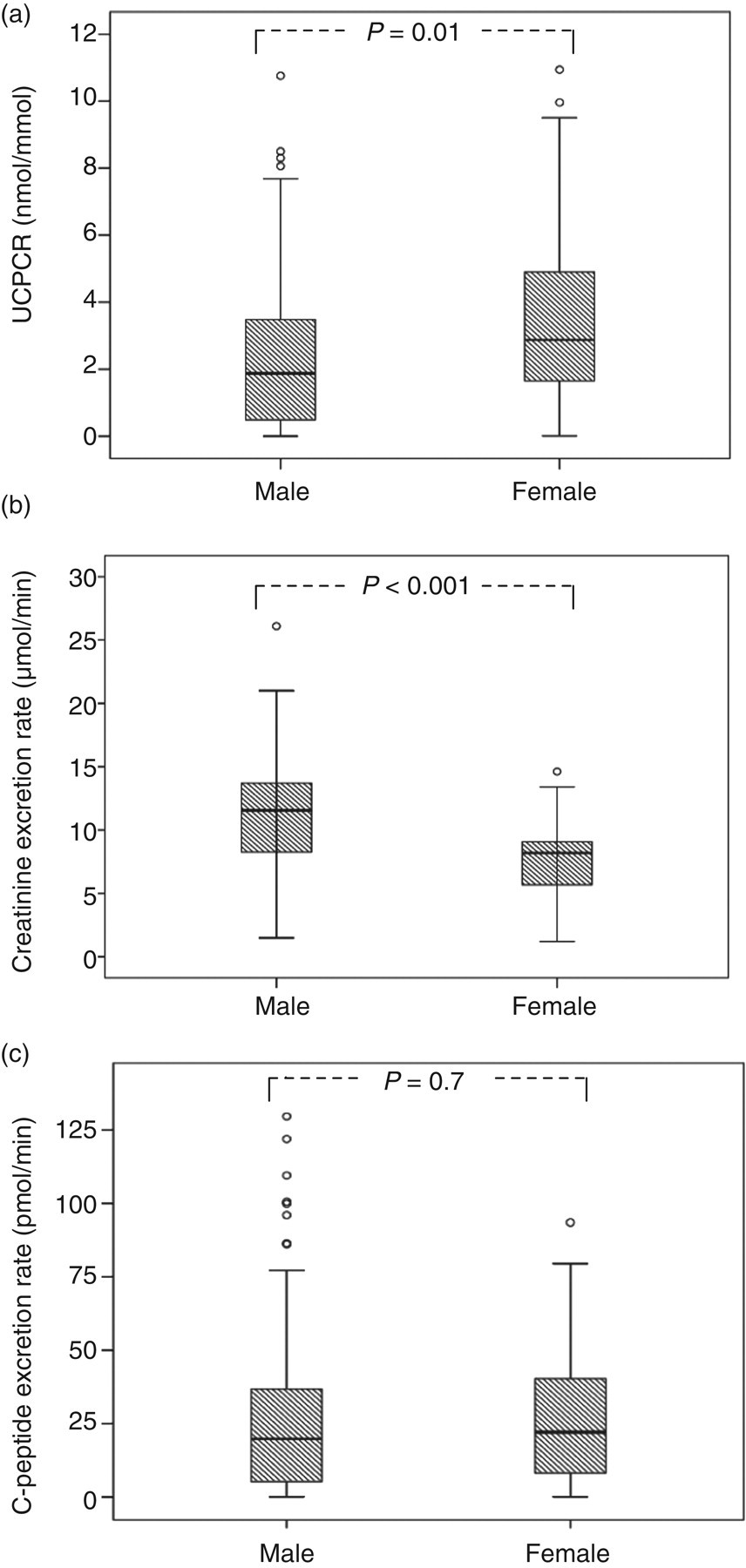
C-peptide excretion is well-correlated with UCPCR (r
2 = 0.81 men, 0.73 women) (Figure 2). Regression analysis showed that in men, C-peptide excretion rate was equivalent to 10.82 times UCPCR (P< 0.001); in women, it was equivalent to 7.31 times UCPCR (P< 0.001), different by a factor of 1.48 (P< 0.001).
The relationship between C-peptide excretion rate and urinary C-peptide creatinine ratio (UCPCR) in men and women. Dotted regression line (r
2= 0.81) and circles represent men, with regression equation UCPCR = 10.82*C-peptide excretion. Solid line (r
2= 0.73) and crosses represent women, with regression equation UCPCR = 7.31*C-peptide excretion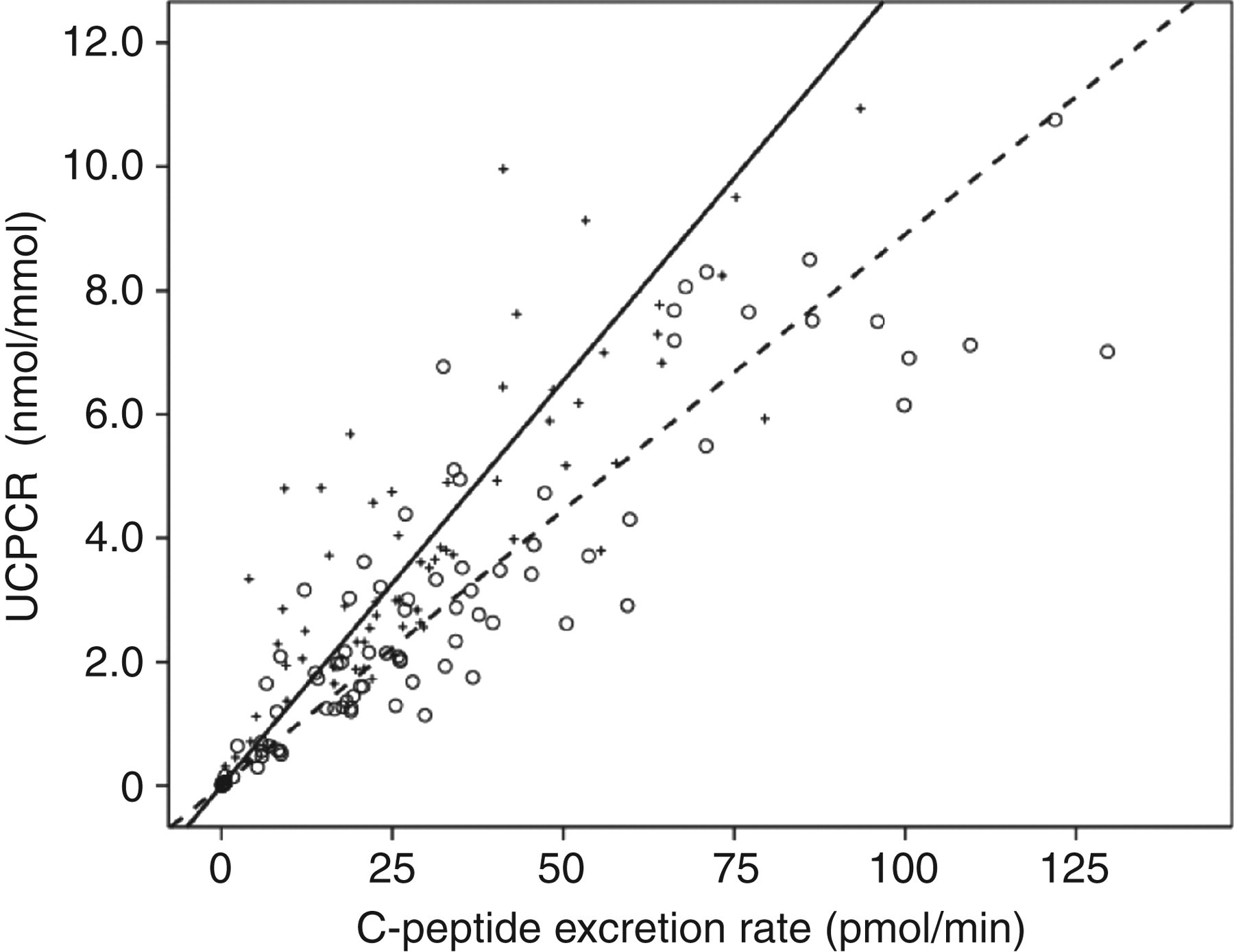
Gender difference by diabetes subtype and treatment
The characteristics of diabetes subtype and treatment groups
Data presented as median and Interquartile range (IQR)
OHA, oral hypoglycaemic agent; HNF, hepatic nuclear factor; BMI, body mass index; HbA1C, glycosylated haemoglobin
Urinary C-peptide creatinine ratios (UCPCR) nmol mmol−1, 25th, 50th and 75th centiles separated for gender, diagnosis and treatment
P represents the overall differences between males and females as assessed by Mann-Whitney U test
OHA, oral hypoglycaemic agent; HNF, hepatic nuclear factor
Discussion
We have demonstrated that UCPCR results are 1.48-fold higher in women than men. This was due to a gender difference in creatinine excretion rates, with higher values in men than women. No sex-specific difference was seen in C-peptide excretion.
Previous research 11,14,15 on the albumin creatinine ratio demonstrated a gender difference in creatinine excretion of a similar magnitude. This difference led to the development of sex-specific cut-offs for significant microalbuminuria in patients with diabetes of 2.5 mg mmol−1 L−1 in men and 3.5 mg mmol−1 L−1 in women. 9,10 The clinical utility of UCPCR means disease- and treatment-specific subgroup ranges are more appropriate.
Having established that gender influences UCPCR through differences in creatinine excretion, we evaluated 591 patients to evaluate the gender influence on disease- and treatment-specific medians and percentiles for UCPCR. This facilitates the potential clinical use of these ranges, allowing a clinician to compare their patients result against a gender-, diagnosis- and treatment-matched population. Female values were consistently higher than male values across all the groups. Participants with type 1 diabetes had the lowest insulin secretion, as would be expected. Those with a duration of less than five years had slightly higher levels. This reflects continued insulin secretion in some patients with type 1 diabetes of short duration. Participants with insulin-treated type 2 diabetes and maturity onset diabetes of the young (MODY) due to mutations in the genes HNF1A and HNF4A that encode hepatic nuclear factors, had lower endogenous insulin secretion than those treated with oral hypoglycaemic agents (OHAs).
This study has limitations; it is known that both race and age affect urine creatinine concentrations as well as gender. 16 In addition to the influence of creatinine, there is decline in beta-cell function with age even in those without diabetes. 17 This means the precise impact of age-related differences on UCPCR will be more complex to evaluate. Our cohort was predominantly Caucasian and further evaluation of gender differences in other ethnic groups remains to be established. In clinical practice, the effects of both age and race on urine creatinine are moderate, and clinically used ACR thresholds for microalbuminuria do not take either of these factors into consideration. 9,10 While only patients with type 2 diabetes on OHAs showed statistical gender difference, in the HNF1A/HNF4A OHA and control groups, the numbers were relatively small and this may explain the lack of statistical difference shown. In addition, the insulin-treated groups had a high percentage of very low and undetectable UCPCR values which would result in any gender difference being minimal.
We excluded individuals with severe renal impairment (eGFR < 30 mL/min/1.73 m2), but this will require further evaluation, particularly with its use in diabetes care. Clinical cut-offs utilizing UCPCR of 0.2 nmol mmol−1 have been proposed as a test to differentiate between HNF1A/HNF4A MODY and type 1 diabetes.7 Increasing male values by 1.48 correctly reclassified one patient with HNF1A/HNF4A but misclassified a patient with type 1 diabetes. This increased the sensitivity from 97% to 99% while decreasing the specificity from 96% to 94% (personal communication, R E Besser, University of Exeter, Exeter, UK). This and the lack of difference in the type 1 diabetes group over five years duration suggests correcting for gender may have little effect on these low thresholds.
Conclusion
We have shown that UCPCR is higher in women as a result of creatinine excretion, likely to be secondary to differences in muscle mass. Adjusting for gender difference should be considered when interpreting UCPCR data and defining clinical thresholds.
DECLARATIONS