
Abstract
Background
Hyperandrogenaemia in polycystic ovary syndrome (PCOS) represents a composite of raised serum concentrations of testosterone, androstenedione, dehydroepiandrosterone (DHEA) and DHEA sulphate (DHEAS). In patients with PCOS, testosterone and androstenedione are primarily derived from the ovaries and DHEAS is a metabolite predominantly from the adrenals. It has been shown that atorvastatin reduces testosterone concentrations in patients with PCOS. The objective was to study the effect of atorvastatin on serum androstenedione and DHEAS concentrations in patients with PCOS.
Methods
A randomized, double-blind, placebo-controlled study was performed. Forty medication-naive patients with PCOs were randomized to either atorvastatin 20mg daily or placebo for three months. Subsequently, a three-month extension study for all patients was undertaken with metformin 1500 mg daily. The main outcome measures were change in androstenedione and DHEAS concentrations.
Results
The mean (SD) baseline androstenedione (5.7 [0.8] versus 5.6 [1.3] nmol/L; P = 0.69) and DHEAS (7.1 [1.0] versus 7.2 [1.2] μmol/L; P = 0.72) concentrations were comparable between two groups. There was a significant reduction of androstenedione (5.7 [0.8] versus 4.7 [0.7] nmol/L; P = 0.03) and DHEAS (7.1 [1.0] versus 6.0 [0.9] μmol/L; P = 0.02) with three months of atorvastatin while there were no significant changes with placebo. Three months' treatment with metformin maintained the reduction of androstenedione and DHEAS concentrations with atorvastatin compared with baseline. There were no changes in either DHEAS or androstenedione concentrations in the initial placebo group after 12 weeks of metformin.
Conclusions
Twelve weeks of atorvastatin significantly reduced both DHEAS and androstenedione contributing to the total reduction of androgen concentrations and indicating that the reduction of the hyperandrogenaemia could be partly due to the action of atorvastatin at both the ovary and the adrenal gland in PCOS.
Introduction
Polycystic ovary syndrome (PCOS) is a heterogeneous disorder characterized by chronic ovulatory dysfunction and hyperandrogenism affecting more than 10% of Caucasian women of reproductive age. 1–3 Androgen excess is considered to be the central defect in PCOS patients; 2 yet it is triggered by other factors, with obesity and insulin resistance being frequently involved. 4 In women, androgens are produced by the adrenal glands and the ovaries, as well as by conversion of less potent androgens to more potent androgens in the periphery. Women with PCOS have serum concentrations of testosterone, androstenedione, dehydroepiandrosterone (DHEA) and DHEA sulphate (DHEAS) that are significantly elevated compared with ovulatory, non-hirsute women. 5 In patients with PCOS, androstenedione is secreted primarily by the ovaries and to a lesser degree the adrenals. This pattern differs from that in normal premenopausal women who have about equal androstenedione and testosterone production from the ovaries and the adrenals. 6 In patients with PCOS, more than 95% of DHEAS is from the adrenal gland and the rest from the ovary, whereas approximately 60% of testosterone is produced by the ovary, 35% from peripheral conversion from androstenedione and 5% from the adrenal gland.
In non-PCOS populations, statins has been shown to reduce inflammation and cardiovascular events. 7,8 Although several lipid-lowering drugs exist and may be used, 9,10 only statins have been adequately studied in women with PCOS and have been shown to effectively lower LDL-cholesterol (LDL-C) concentrations. Several studies have shown that in women with PCOS, statins diminish insulin resistance and inflammation 11,12 and improve brachial artery conductance during reactive hyperaemia. 13,14 Statins also inhibit ovarian theca-interstitial cell proliferation and steroidogenesis in vitro 15,16 and this inhibition is shown to be independent of cholesterol availability. 17 Statins, in addition, have been shown to reduce total testosterone concentrations in patients with PCOS. 11,12,18–20 This study was performed to investigate the effect of atorvastatin on androstenedione and DHEAS concentrations in patients with PCOS.
Materials and methods
A randomized, double-blind, placebo-controlled study was undertaken using atorvastatin 20 mg daily 12 at a tertiary care centre in UK. The diagnosis of PCOS was based on all three diagnostic criteria of the Rotterdam consensus, namely clinical and biochemical evidence of hyperandrogenaemia (Ferriman-Gallwey score >8; free androgen index >8, respectively), oligomenorrhea or amenorrhea and polycystic ovaries on transvaginal ultrasound. 3 Subjects had no concurrent illness, and were not on any prescription or over-the-counter medication that was likely to affect insulin sensitivity, lipids or ovarian function including hormonal contraceptives for the preceding six months. None of the patients had statin therapy in the past. Subjects were not planning to conceive and were using barrier contraception. Subjects were advised not to change their lifestyle, including physical activity or dietary habits, during the study period. Non-classical 21-hydroxylase deficiency, hyperprolactinaemia, Cushing's disease and androgen-secreting tumours were excluded by appropriate tests. Forty-four patients were screened before the study, and two patients were excluded due to use of oral contraceptives within the previous six months and two patients due to use of metformin in the previous six months. Forty subjects who fulfilled both inclusion and exclusion criteria were randomly assigned to the atorvastatin or the placebo group based on a computer-generated randomization list. Each randomization number corresponded with one of the two possible interventions, and labelling was done by personnel not involved in the trial. Compliance with treatment was calculated by counting the returned medications. Thirty-seven patients completed the study. Two patients from the placebo group and one patient from the atorvastatin group dropped out of the study within four weeks due to non-compliance. 12 Immediately after stopping the trial medication, 37 patients (19 patients from the atorvastatin group and 18 patients from the placebo group), who completed the study, were given metformin 500 mg three times daily for three months. 21 A flow chart describing the progress of patients through the study is shown in Figure 1. The study was conducted during January 2006–December 2007. The study was completed after the last patient's last study visit. The main outcome measures were changes in DHEAS and androstenedione concentrations. All patients gave informed consent. The study was approved by the South Humber Research Ethics committee.
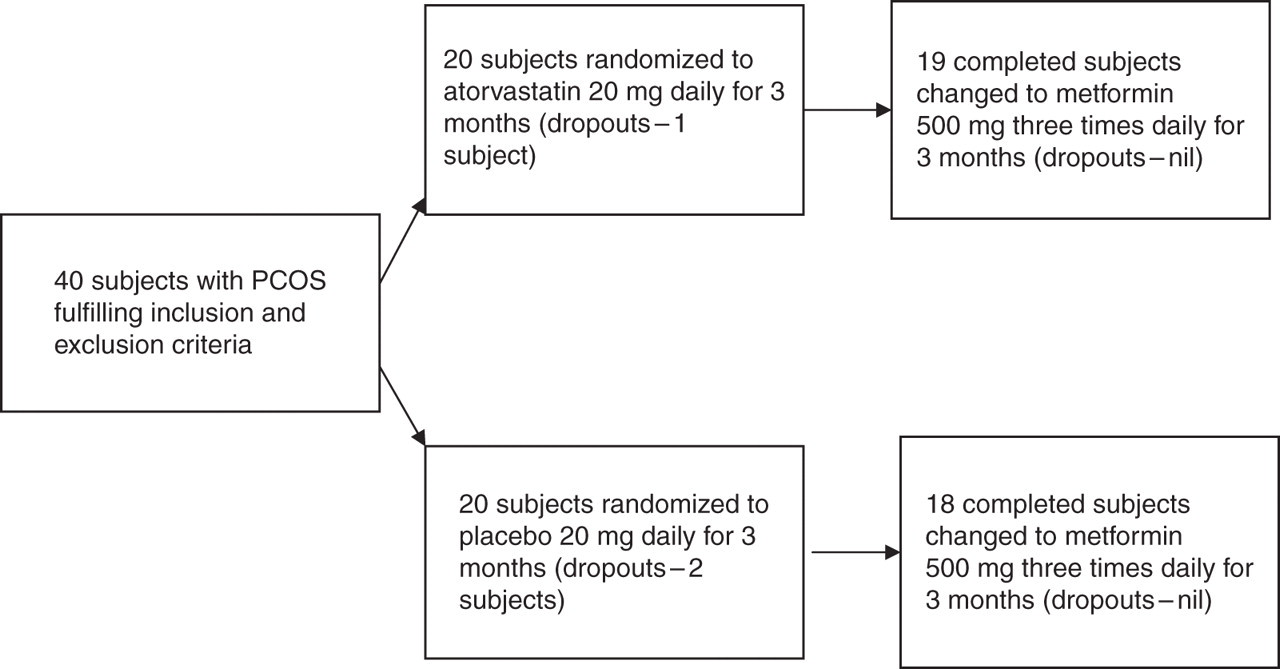
A flow chart describing the progress of patients through the study. PCOS, polycystic ovary syndrome
Blood samples were taken after an overnight fast and serum was stored frozen at −80°C pending analysis. Compliance was monitored by counting returned medication.
Serum androstendione was measured by liquid chromatography-tandem mass spectrometry on an Acquity UPLC system coupled to a Quattro Premier XE mass spectrometer (Waters, Manchester, UK). Samples and standards (androstenedione 0.1–36 nmol/L; QMX Laboratories, Essex, UK) were supplemented with deuterated internal standard (d5-testosterone) before undergoing an ether extraction. After samples were dried down and reconstituted in 50:50 (v/v) mobile phase A/B, 35 μL was injected into the high-performance liquid chromatography column. Samples were separated on a Synergi 4 μm Hydro-RP column, 50 × 3 mm (Phenomenex, Cheshire, UK), with mobile phases A (water + 2 mmol/L ammonium acetate and 0.1% formic acid) and B (methanol + 2 mmol/L ammonium acetate and 0.1% formic acid) using the following program: flow rate 0.6 mL/min, 0–2 min 30% A 70% B, 2–2.5 min gradient to 2% A 98% B, 2.5–3 min gradient to 30% A 70% B. Androstenedione was detected using the transition m/z 287.2 > 97.1 (internal standard m/z 294.2 > 100.1) and the concentration of androstendione in serum samples was calculated using MassLynx software (Waters). The % coefficient of variation (%CV) of the assay was determined to be 5.97% at 8.7 nmol/L and 7.3% at 27.0 nmol/L. DHEAS was measured according to the manufacturer's instructions by competitive immunoassay on the Immulite 2000 analyser (Siemens Diagnostics, Surrey, UK). The %CV of the assay was determined to be 7.8% at 3.6 and 10.2 nmol/L. Assays used for measuring total testosterone, sex hormone-binding globulin, total cholesterol, LDL-C, triglycerides and insulin are described elsewhere. 12
Statistical analysis
The sample size was based on the study on the known effect of atorvastatin on high-sensitivity C-reactive protein (CRP) in patients with impaired fasting glucose, 22 with the assumption that a similar effect would occur in those patients with PCOS. Powered specifically for CRP, the minimum difference worth detecting/observed difference was 32.7%, estimated within-group SD was 11.1; therefore, for 90% power and a significance level of 5%, a sample size of 16 per group was calculated. Adjusting for a possible 20% dropout rate meant a total of 40 patients needed to be recruited.
The paired t-test was used to compare changes from baseline for the biochemical data and clinical observations within groups. The Wilcoxon signed-rank test was applied to biochemical data that violated the assumptions of normality when tested using the Kolmogorov–Smirnov test. The effect of treatment was evaluated by first computing the percentage change from baseline in all variables studied and then the percent change seen for each variable in both groups was compared, thus negating the differences in the baseline values of the two groups. Between-group comparison of percent changes was performed using independent samples t-test. For all analysis, a two-tailed P ≤ 0.05 was considered to indicate statistical significance. Statistical analysis was performed using SPSS for Windows NT, Version 14.0 (SPSS Inc, Chicago, IL, USA).
Results
The mean (SD) age of the patients was 27.7 (1.4) y. The baseline parameters are described in Table 1. None of the subjects developed significant side-effects in the course of the study. None of them developed symptoms of muscle toxicity, and liver function tests and creatine kinase remained normal throughout the study.
Comparison of baseline parameters of atorvastatin and placebo group
DHEAS, dehydroepiandrosterone sulphate
There was a significant reduction of DHEAS (7.1 [1.0] versus 6.0 [0.9] nmol/L; P = 0.02) (Figure 2) and androstenedione (5.7 [0.8] versus 4.7 [0.7] nmol/L; P = 0.03) (Figure 3) concentrations within the atorvastatin treatment group after three months. This was reflected in the atorvastatin compared with placebo after three months that showed that the DHEAS (6.0 [0.9] versus 6.9 [0.7] nmol/L; P ≤ 0.01) and androstenedione (4.7 [0.7] versus 6.3 [3.2] nmol/L; P ≤ 0.01) concentrations were significantly lower compared with placebo. The 15% reduction in DHEAS and 17% reduction in androstenedione were significantly higher than the comparative reduction in the placebo group.
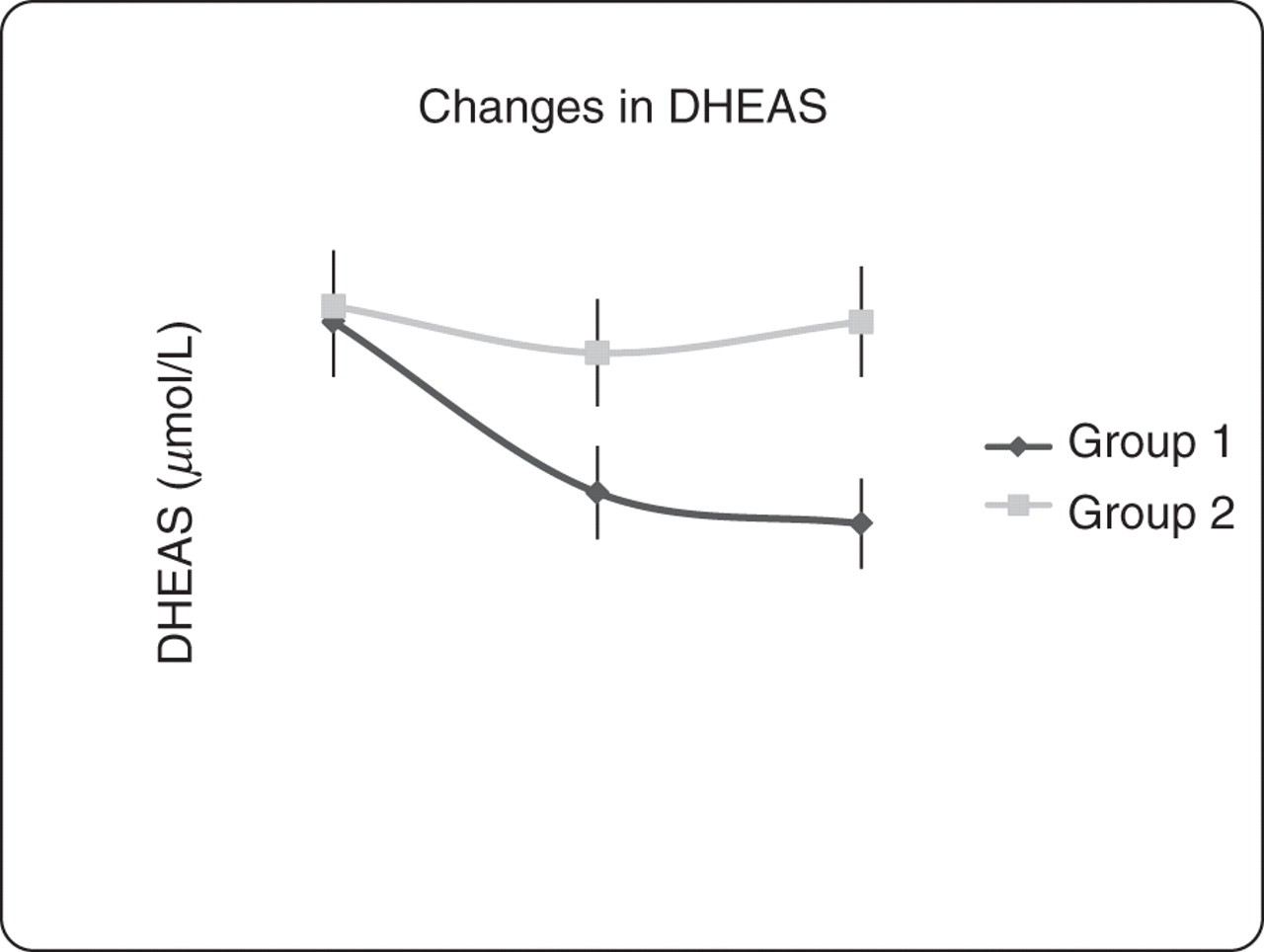
Changes in DHEAS. Group 1 – atorvastatin for 12 weeks followed by metformin for 12 weeks. Group 2 – placebo for 12 weeks followed by metformin for 12 weeks. Visit 1 (V1) – baseline; Visit 2 (V2) – 12 weeks from baseline on either atorvastatin or placebo; Visit 3 (V3) – 24 weeks from baseline (12 weeks from visit 2 on metformin 1.5 g daily). Comparison between V1, V2, V3 in each group was done using paired t-test. P values for changes in DHEAS in Group 1: V1–V2 = 0.02; V2–V3 = 0.12; V1–V3 < 0.01; P value < 0.01 for percent difference between both groups using unpaired t-test between V1 and V3. P values for changes in DHEAS in Group 2: V1–V2 = 0.54; V2–V3 = 0.28; V1–V3 = 0.49. DHEAS, dehydroepiandrosterone sulphate
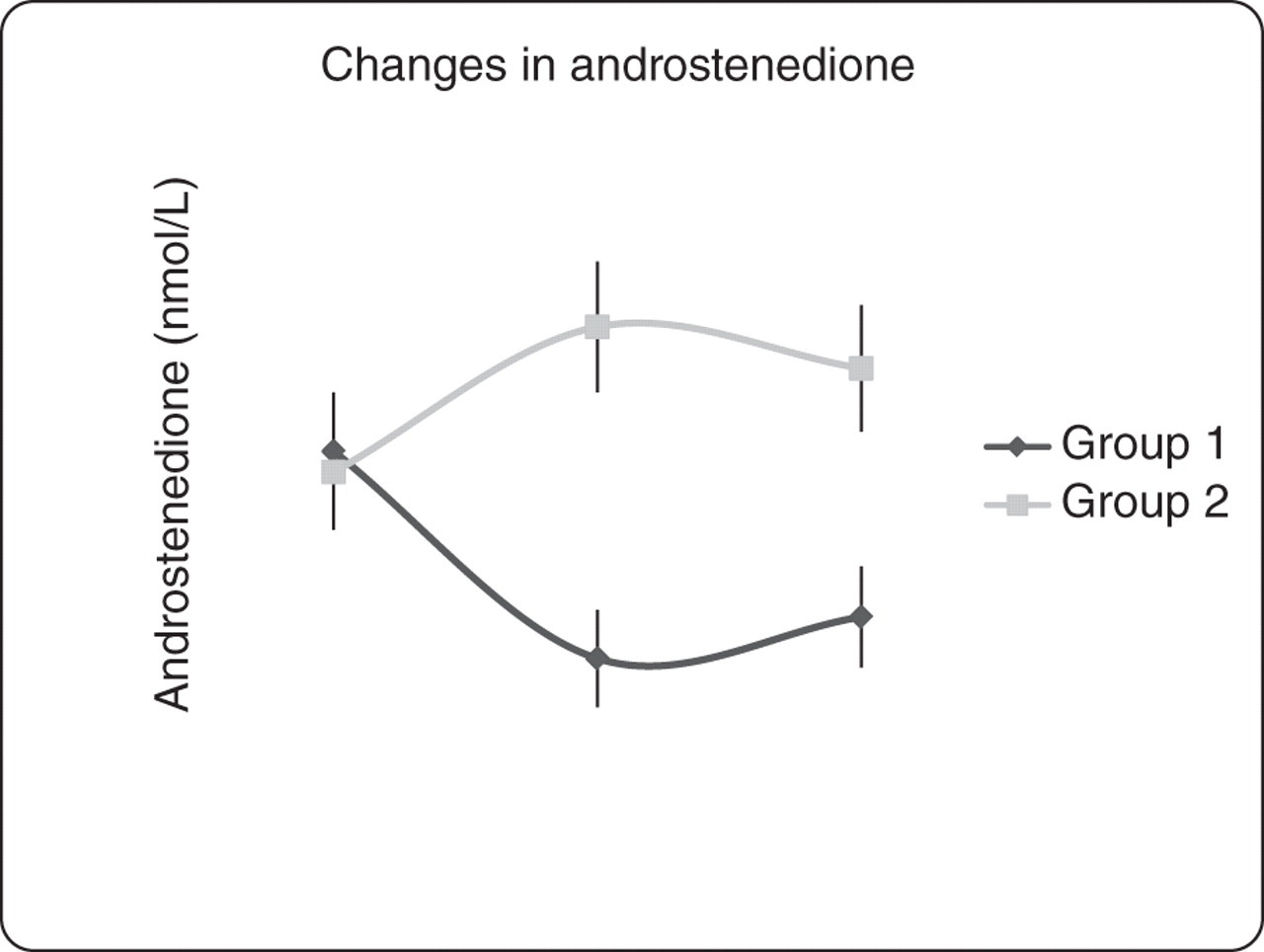
Changes in androstenedione. Group 1 – atorvastatin for 12 weeks followed by metformin for 12 weeks. Group 2 – placebo for 12 weeks followed by metformin for 12 weeks. Visit 1 (V1) – baseline; Visit 2 (V2) – 12 weeks from baseline on either atorvastatin or placebo; Visit 3 (V3) – 24 weeks from baseline (12 weeks from visit 2 on metformin 1.5 g daily). Comparison between V1, V2, V3 in each group was done using paired t-test. P values for changes in androstenedione in Group 1: V1–V2 = 0.03; V2–V3 = 0.12; V1–V3 = 0.02; P value = 0.03 for percentage difference between both groups using unpaired t-test between V1–V3. P values for changes in androstenedione in Group 2: V1–V2 = 0.62; V2–V3 = 0.64; V1–V3 = 0.62
Three months' treatment with metformin maintained the reduction of androstenedione (5.7 [0.8] baseline versus 4.9 [1.2] nmol/L for atorvastatin-treated; P = 0.02) and DHEAS (7.1 [1.0] baseline versus 5.8 [1.2] μmol/L for atorvastatin-treated; P < 0.01) with atorvastatin compared with baseline. There were no significant changes in either androstenedione or DHEAS concentrations in the placebo group after 12 weeks of metformin.
The changes in total testosterone, free androgen index (FAI), homeostatic model assessment-insulin resistance (HOMA-IR), total cholesterol, LDL-C and triglycerides are described elsewhere. 12 There was no correlation between the reduction of DHEAS concentrations with the reduction in testosterone concentrations (r = 0.22, P = 0.32), FAI (r = 32, P = 0.12), total cholesterol (r = 0.24, P = 0.33), LDL-C (r = 0.28, P = 0.15), triglycerides (r = 0.18, P = 0.44) or HOMA-IR (r = 0.32, P = 0.11). There was also no correlation between the reduction of androstenedione concentrations with changes in testosterone (r = 0.12, P = 0.44), FAI (r = 0.20, P = 0.24), total cholesterol (r = 0.28, P = 0.56), LDL-C (r = 0.18, P = 0.52), triglycerides (r = 0.32, P = 0.10), HOMA-IR (r = 0.24, P = 0.12) or DHEAS (r = 0.17, P = 0.32).
Discussion
Atorvastatin treatment for 12 weeks significantly reduced androstenedione and DHEAS concentrations in patients with PCOS, with these parameters being maintained by three months of metformin therapy. This suggests that the reduction in hyperandrogenaemia seen was in part through the reduction of these metabolites and that the mechanism of atorvastatin is through a direct effect on steroidogenesis in both the ovary and the adrenal gland.
In another randomized, double-blind, placebo-controlled study of 20 patients with PCOS having high LDL-C using atorvastatin 40 mg daily for six weeks, there was no significant reduction in total testosterone or insulin resistance, whereas there was significant reduction in androstenedione and DHEAS. 13 On the contrary, in our study using atorvastatin 20 mg daily for 12 weeks, there was a significant reduction in total testosterone, DHEAS and androstenedione. There was also no correlation with changes of testosterone concentrations with changes in androstenedione or DHEAS concentrations. This implies that the mechanisms of inhibitory effect of atorvastatin on these three androgens are different and independent from each other.
There was a 17% reduction in androstenedione concentrations with three months of atorvastatin therapy in this study. It has been previously shown in vitro that lovastatin inhibits androstenedione production by porcine ovarian theca cells at the level of the 17α-hydroxylase:C-17,20-lyase complex suggesting that preformed intracellular cholesterol, rather than that synthesized de novo, is supplying steroidogenic substrate in these cells. 23
In this study, there was a 15% reduction in DHEAS concentrations with 12 weeks of atorvastatin. The trend towards reduction in DHEAS related to acquired LDL-C insufficiency was previously reported in chronically ill patients. 24 A significant reduction in DHEAS concentrations after simvastatin at doses up to 40 mg was reported in children with familial hypercholesterolaemia. 25 In addition, it has also been shown in patients with type 2 diabetes that there is a dose-dependent reduction in serum DHEAS concentrations with atorvastatin. 26 Serum concentration of DHEAS is a good marker of adrenal androgen hypersecretion. Since DHEAS has a long serum half-life, with minimal pulsatile or diurnal variation, a single measurement of serum DHEAS correlates well with integrated measures of DHEAS secretion. Small amounts of DHEA and DHEAS are converted to androstenedione and then to testosterone (and to oestrogen) in both the adrenal glands and peripheral tissues. In this study, 12 weeks of atorvastatin reduced DHEAS concentrations, suggesting that the mechanism of action of atorvastatin in reducing hyperandrogenaemia in women with PCOS may partly involve suppressing adrenal androgen production along with suppressing testosterone production, which is mainly by ovaries. However, there was no correlation between reduction of testosterone concentrations and suppression of DHEAS in this group, suggesting that atorvastatin may affect both adrenal and ovarian androgen production.
There was no correlation between improvement of insulin resistance and reduction in DHEAS or androstenedione concentrations. In a double-blind, randomized, placebo-controlled study, troglitazone improved the insulin resistance-related hyperinsulinaemia of PCOS with a decrease in DHEAS concentrations. 27 However, metformin, one of the commonly used insulin sensitizers, did not have any effect in basal DHEAS concentrations in patients with PCOS. 28 It is possible that the effect of thiazolidinediones observed on steroid concentrations may be the result of direct inhibition of steroid biosynthesis by these drugs. 29 Troglitazone acts partly through PPARα and there is some evidence that statins activate PPARα as well through inhibition of the Rho-signalling pathway. 30 Another potential mechanism might be that statins could have an effect on DHEA sulphotransferase (SULT2A1) enzyme. DHEAS is activated to DHEA by steroid sulphatase, and DHEA is inactivated to DHEAS by SULT2A1. Statins might also have an effect on ovarian CYP17 activity, the enzyme responsibile for DHEA biosynthesis.
Although ovulatory function was not measured, there was no change in cycle length before and after treatment with atorvastatin (52 ± 12 versus 50 ± 6 d, P value – 0.52) or placebo (55 ± 8 versus 52 ± 10 d, P value – 0.43). 12 On a cautionary note, statins are considered to be potentially teratogenic; hence, it is recommended that their use should be restricted to women who are either not sexually active or using reliable contraception. 31 All the participants in the study were not planning to conceive and were using barrier contraception. Interestingly, a small, observational trial on women taking statins during the first trimester of pregnancy was reassuring, and suggested that the risk of statin-induced teratogenicity, if any, was small. 32 While there was a significant reduction in serum testosterone, free androgen index, androstenedione and DHEAS, we did not document any changes in hirsutism, although the time frame of the study was too short to measure this clinical parameter.
In conclusion, this study has shown that atorvastatin for 12 weeks reduces androstenedione and DHEAS concentrations in patients with PCOS. This suggests that the mechanism of action of atorvastatin in reducing hyperandrogenaemia in patients with PCOS could partly be due to suppression of these androgens in addition to reduction in testosterone concentrations.
DECLARATIONS