
Abstract
Background
The risk association between the insulin like growth factor-I (IGF-I) system and cardiovascular risk is inconclusive in adults and under-explored in adolescents. We aimed to investigate the associations between serum concentrations of IGF-I and IGF binding protein-3 (IGFBP-3) and cardiovascular risk factors in adolescents.
Methods
This was a cross-sectional, population-based, observational study in a school setting with 2102 Hong Kong Chinese adolescents aged 12–19 years. Serum IGF-I and IGFBP-3 concentrations were measured by chemiluminescence immunoassays. Anthropometric indices and traditional cardiovascular risk factors were assessed.
Results
After excluding participants with abnormal thyroid and liver test results, 765 boys and 877 girls, mean (±SD) age of 15.3 (±2.0) and 15.7 (±2.0) years, respectively, were included in the analysis. Multivariable regression analyses revealed that both IGF-I and IGFBP-3 concentrations were independently associated with waist circumference, fasting insulin and haemoglobin concentrations in boys (all P < 0.05), systolic blood pressure, serum creatinine, fasting insulin and haemoglobin concentrations in girls (all P < 0.05). In girls, IGF-I was also associated with C-reactive protein concentration (P < 0.001) and IGFBP-3 was associated with fasting triglyceride concentration (P < 0.001). Compared with adolescents with the lowest tertile, the top tertile of both IGF-I and IGFBP-3 concentrations were associated with increased odds of having overweight/obesity, top tertiles of insulin and haemoglobin in both boys and girls (P for trend, all <0.05).
Conclusions
The associations between serum IGF-I, IGFBP-3, obesity, cardiovascular risk factors, insulin and haemoglobin suggest that dysregulation of the IGF system may play a linking role for the clustering of cardiovascular risk factors.
Introduction
The metabolic syndrome, a clustering of cardiometabolic risk factors, associated with insulin resistance commonly has obesity as one of its components. 1 The growth hormone (GH)-insulin like growth factor-I (IGF-I) system plays important roles in energy homeostasis and body fat distribution in adults as well as somatic growth in children and adolescents. The effects of IGF-I are tightly regulated by the IGF-binding proteins. Among the IGF-binding proteins, IGF-binding protein-3 (IGFBP-3) is the principal serum carrier protein of circulating IGF-I and regulates the actions of IGF-I at the cellular level. 2 The structural homology between IGF-I and insulin suggest that IGF-I and its binding proteins may play an intrinsic role in glucose homeostasis, and be implicated in the pathogenesis of the metabolic syndrome. Apart from conventional cardiovascular risk factors, it has been suggested that abnormalities of the GH–IGF-I axis are involved in the pathogenesis of cardiovascular disease. Our group has recently reported that IGFBP-3 gene polymorphisms play a role in regulating IGF-I activity and lipid concentrations in adolescents, 3 providing supporting evidence that the IGF system may modify cardiovascular risk factors.
Published studies reporting the risk association of IGF-I and cardiovascular risk in adults are conflicting. While low IGF-I concentrations have been reported to correlate with increased risk of impaired glucose tolerance 4,5 and ischaemic heart disease, 6,7 a non-linear, U-shaped relationship has been demonstrated between IGF-I concentrations and body mass index (BMI) in European women. 8 Recently, a U-shaped relationship has also been reported between metabolic syndrome and IGF-I, as well as IGFBP-3 concentrations in elderly Australian men aged ≥70 years. 9 These inconsistent findings may be related to differences in clinical characteristics of study populations in terms of age, sex, ethnicity and presence of co-morbidities, as well as the associations of cardiovascular risk with nutrition and renal related parameters 10,11 and the associations between IGF system and nutritional status. 12 Adding to this complexity is the modulation of IGF-I activity by IGFBPs, 2 and therefore clarifying associations of circulating IGF-I and IGFBPs will serve to establish whether these biochemical markers are of value in identifying at risk individuals for early screening and intervention.
Despite the growing epidemic of childhood obesity and metabolic syndrome, 13 there is a paucity of data investigating the relationships between the IGF system and cardiovascular risk in the adolescent population. In this cross-sectional survey, we examined the associations between serum IGF-I, IGFBP-3 concentrations and cardiovascular risk factors, both traditional and non-traditional, in Hong Kong Chinese adolescents.
Methods
Subjects
The study was conducted in 2003 and the methodology has been reported previously. 14,15 In brief, from 477 secondary schools in Hong Kong, 53 schools were randomly selected using a computer-generated coding system. Of these, 14 schools participated in the study with the approval of their principals. Only healthy adolescents of Chinese ethnicity without any major medical illness and not on long-term drug treatment were recruited for assessment. Informed written consent was obtained from all participants and their parents.
After an overnight fast of at least eight hours, all participants underwent anthropometric measurements and blood sampling at school by a team of trained research nurses and assistants. Waist circumference (WC), body weight (measured to the nearest 0.1 kg by Tanita physician digital scale; Tanita Corp, Tokyo, Japan) and height (measured to the nearest 0.1 cm using a portable stadiometer) were measured. Blood pressure (BP) was measured after at least five minutes’ rest using a validated electronic device (Omron; Omron Healthcare Inc, Tokyo, Japan).
Laboratory measurements
Blood samples were kept in ice at 0°C before transport to the laboratory. Plasma glucose (hexokinase method), total cholesterol (enzymatic method), triglyceride (TG; enzymatic method without glycerol blanking), high-density lipoprotein cholesterol (HDL-C; direct method using polyethylene glycol [PEG]-modified enzymes and dextran sulphate), and renal and liver function tests including plasma alanine aminotransferase (ALT) concentrations were measured on a Roche Modular Analytics system (Roche Diagnostics GmbH, Mannheim, Germany) using standard reagent kits supplied by the manufacturer. Blood haemoglobin (Hb), white blood cell and platelet counts were measured by an automated cell counter (GEN-S; Beckman Coulter, Miami, FL, USA). Serum concentrations of IGF-I, IGFBP-3, thyrotropin (TSH) and high-sensitivity C-reactive protein (hs-CRP) were measured by an automated chemiluminescent assay system (IMMULITE 2000®; Diagnostic Products Corp, Los Angeles, CA, USA). Free thyroxine (fT4) was measured by an automated analytical chemistry system, Modular Analytics (Roche Diagnostics GmbH), if the TSH concentration was abnormal. Reagent preparation and analyses were performed according to the manufacturers’ instructions. Analytical performance of all assays was within the manufacturers’ specifications. The sensitivity of the hs-CRP and insulin assays were 0.1 mg/L and 2 mIU/L, respectively. Subjects with abnormal TSH and/or fT4 and ALT (>40 IU/L) were excluded from the analysis. This particular ALT cut-off was adopted since previous research in our local population suggested that subjects with even marginally elevated serum ALT activity (i.e. at 0.5 × upper limit of healthy population reference range) might still be associated with significant histological abnormalities in the liver. 16
Low-density lipoprotein cholesterol (LDL-C) concentrations was calculated using the Friedewald formula for TG < 4.5 mmol/L. 17 Insulin resistance (IR) was calculated from the Homeostasis Model Assessment (HOMA) where HOMA-IR = fasting plasma glucose (FPG) (mmol/L) × fasting insulin (μU/mL) ÷ 22.5 and insulin secretion, by HOMA-β = (20 × fasting insulin [μU/mL]) ÷ (FPG [mmol/L]–3.5). 18
Statistical analysis
Data are presented as mean (±SD), median (IQR, interquartile range) or frequency (%) as appropriate. Fasting TG and insulin, HOMA-IR and HOMA-β were natural log-transformed to correct skewness before being subjected to analysis. IGF-I and IGFBP-3 were first regressed with age and the standardized residuals were retained to represent the age-adjusted values.
Univariate association between age-adjusted IGF-I and IGFBP-3 and each of the clinical and laboratory measurements was assessed by Pearson's or Spearman's correlation coefficients. Significant variables were then entered into multivariable linear regression models to delineate factors independently associated with age-adjusted IGF-I and IGFBP-3. To avoid co-linearity during regression analysis, for highly correlated variables, only the one with the smallest univariate P value was selected for multivariable analyses (e.g. systolic BP was selected instead of entering both systolic BP and diastolic BP). The highly skewed hs-CRP and ALT were categorized into two groups according to <75th or ≥75th percentile for boys and girls separately before entering into regression analysis.
Overweight and obesity were defined by BMI greater than Hong Kong local age and gender-specific 85th and 95th percentiles, respectively. 19 The local percentile standards were based on the latest local population survey. 20 Subjects were considered to have clustering of cardiovascular risk factors according to the modified criteria used in the Third National Health and Nutrition Examination Survey 21 : three or more of the following risk factors HDL-C ≤ 1.03 mmol/L, LDL-C ≥ 2.6 mmol/L, TG ≥ 1.24 mmol/L, FPG ≥ 6.1 mmol/L and age-, sex- and height-adjusted systolic or diastolic BP ≥ 90th percentile. The presence of metabolic syndrome was determined using the International Diabetes Federation definition. 22
Using the lowest tertile group as reference, the odds ratio (OR, 95% confidence intervals) of middle and top tertile groups of age-adjusted IGF-I and IGFBP-3 for (i) overweight/obesity; (ii) obesity only; (iii) clustering of cardiovascular risk factors; (iv) metabolic syndrome; (v) fasting insulin concentration in the top tertile; (vi) blood Hb concentration in the top tertile; and (vii) the upper tertile of both fasting insulin and blood Hb concentrations were also estimated. Statistical analyses were performed using SPSS 16.0 (SPSS Inc, Chicago, IL, USA). All statistical tests were two-sided and a P value <0.05 was considered statistically significant.
Results
Table 1 summarizes the clinical and biochemical characteristics of the 1642 participants. After excluding 92 adolescents, 50 with abnormal ALT (defined as >40IU/L) and 42 with abnormal thyroid function tests, 1642 eligible participants were included in the analyses (Figure 1). The mean ages of the participants (765 boys and 877 girls) were 15.3 (±2.0) and 15.7 (±2.0) years, respectively.
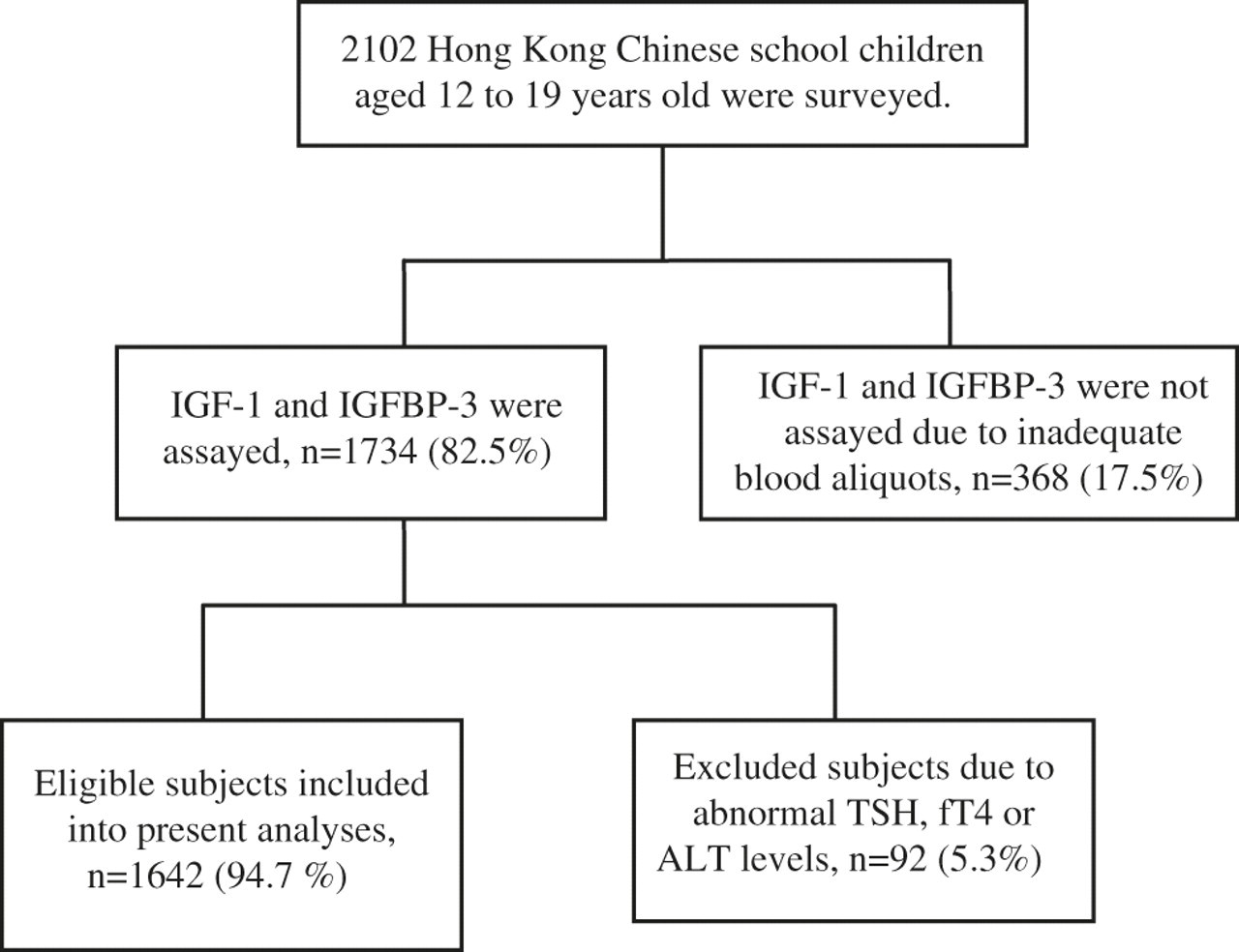
Participant enrollment: from 2102 Hong Kong Chinese school children aged 12–19 years, 1642 were included in the study. IGF, insulin like growth factor-I; IGFBP-3, IGF binding protein-3; ALT, alanine aminotransferase; fT4, free thyroxine; TSH, thyrotropin
Demographic and clinical characteristics of the participants
BP, blood pressure, IGF-I, insulin like growth factor-I; IGFBP-3, IGF binding protein-3; BMI, body mass index; HOMA, Homeostasis Model Assessment; hs-CRP, high-sensitivity C-reactive protein
†Data are presented as median (interquartile range), while all others are presented as mean (standard deviation)
‡Insulin resistance, HOMA-IR = fasting plasma glucose (mmol/L) × fasting insulin (mIU/L) ÷ 22.5; HOMA-β = (20 × fasting insulin [mIU/L]) ÷ (fasting plasma glucose [mmol/L] − 3.5)
In boys, both serum IGF-I and IGFBP-3 concentrations were independently associated with obesity indices (WC), fasting insulin and Hb concentrations (all P < 0.05, Table 2). Similarly, in girls, systolic BP, serum creatinine, fasting insulin and Hb concentrations were independently associated with both serum IGF-I and IGFBP-3 concentrations (all P < 0.05, Table 2). In addition, IGF-I concentration was associated with inflammatory marker (hs-CRP concentration, P < 0.001) and IGFBP-3 concentration was associated with lipid profile (fasting TG concentration, P < 0.001) in girls. Compared with adolescents of the lowest tertile, adolescents with top tertile of IGF-I concentration were associated with about two- to four-fold increased odds of having overweight/obesity, hyperinsulinaemia (top tertiles of insulin) and haemoconcentration (top tertiles of Hb) in both boys and girls (Table 3). Similarly, adolescents with top tertile of IGFBP-3 concentrations when compared with those with lowest tertile of IGFBP-3 had increased odds of having overweight/obesity, clustering of cardiovascular risk factors, and top tertiles of insulin and Hb concentrations (Table 4).
Association between age-adjusted serum IGF-I, IGFBP-3 concentrations and cardiometabolic risk factors
NE, not entered into multiple regression to avoid colinearity; NS, not significant in multivariate analysis; NA, not applicable; BP, blood pressure, IGF−1, insulin like growth factor-I; IGFBP-3, IGF binding protein-3; BMI, body mass index; HOMA, Homeostasis Model Assessment; hs-CRP, high-sensitivity C-reactive protein: Hb, haemoglobin; ALT, alanine aminotransferase; WBC, white blood cells
†Pearson's correlation coefficients, except hs-CRP and ALT, where Spearman's correlation coefficients were calculated instead
‡Multiple linear regression using stepwise entering method for univariately significant independent variables
¶Values were natural log-transformed for analysis
#hs-CRP and ALT were recoded as categorical variables when entering into multiple regression analysis; values below the 75th percentile were grouped as the reference group
Bold values are statistically significant with *P < 0.05; **P < 0.01; ***P < 0.001
Association between age-adjusted serum IGF-I concentration (divided into tertiles) and cardiometabolic measures
NA, not applicable; IGF-1, insulin like growth factor-I; CV, cardiovascular; Hb, haemoglobin
†Clustering of cardiovascular risk factors are defined according to modified criteria of the National Health and Nutrition Examination Survey 20
‡International Diabetes Federation (IDF) definition of metabolic syndrome 22
Bold values are statistically significant with P values <0.05
Association between age-adjusted serum IGFBP-3 concentration (divided into tertiles) and cardiometabolic measures
NA, not applicable; IGFBP-3, IGF binding protein-3; CV, cardiovascular; Hb, haemoglobin
†Clustering of cardiovascular risk factors are defined according to modified criteria of the National Health and Nutrition Examination Survey 20
‡International Diabetes Federation (IDF) definition of metabolic syndrome 22
Bold values are statistically significant with P values <0.05
Discussion
The results of our study support the association between the IGF system and cardiovascular risk factor clustering in Chinese adolescents. We have found an independent association between serum IGF-I, IGFBP-3 and insulin concentrations in both boys and girls after adjusting for potential confounders. Adolescents with the top tertile IGF-I and IGFBP-3 concentrations were at increased risk of having overweight/obesity and hyperinsulinaemia when compared with adolescents with the lowest tertile of IGF-I and IGFBP-3. To our knowledge, this is the first large-scale, community-based study demonstrating such associations in Chinese adolescents. Nevertheless, evidence is available from human and animal as well as from in vitro studies suggesting an association between IGFBP-3, insulin resistance and hyperinsulinaemia. 24 In animal models, transgenic mice overexpressing IGFBP-3 develop insulin resistance as measured by reduced uptake of 2-deoxyglucose in muscle and adipose tissue. 25 IGFBP-3 can be regarded as a growth factor that regulates apoptosis of cells and may influence the peroxisome proliferator activated receptor-γ (PPAR-γ) signalling through its binding to the nuclear transcription factor retinoid X receptor-alpha (RXR-α). 2,26 The IGFBP-3 and RXR ligands are shown to be additive in their effect in inducing apoptosis in prostate cancer cells. 26 Since RXR-α plays a crucial role in the PPAR-γ signalling pathway and PPAR-γ signalling pathway is important in the pathogenesis of insulin resistance, it is plausible that there is cross-talk between growth factors and nuclear receptor ligands in both malignant and metabolic diseases. 26 In adipocytes, IGFBP-3 impacts on glucose uptake and contributes to insulin resistance. 27 It has been postulated that IGFBP-3 may lead to insulin resistance via an IGF-independent mechanism. 27 Although there are many mechanisms which may explain the association between insulin resistance and obesity, such as increased free fatty acid concentration and adipocytokines, 1 the results of our study show that the association between IGF-I, IGFBP-3 and hyperinsulinaemia was independent of obesity in both genders.
The results of our study also suggest a plausible link between IGF-I, IGFBP-3 and clustering of cardiovascular risk factors. This is in keeping with the findings reported in a case-control prospective study in Denmark. 6 In this population-based study involving around 500 middle-aged adults in Denmark, high IGFBP-3 concentrations were shown to predict ischaemic heart disease, independent of obesity. 6 In another study of middle-aged men in Germany, IGFBP-3 was also independently correlated with coronary atherosclerosis as measured by coronary angiography. 28 In addition, we have shown that traditional cardiovascular risk factors, including WC, systolic BP, TG and an inflammatory marker are independently associated with IGF-I and/or IGFBP-3 concentrations. Given the growth-promoting effect of the IGF system, increased cardiovascular risk may be related to the dysregulation of angiogenesis and endothelial dysfunction by the IGF system. 29,30 It has been shown that IGFBP-3 modulates stem cell receptor, regulates the cellular function of haematopoietic stem cells and mediates endothelial precursor cell migration, differentiation and capillary formation in vitro. 29 Overexpression of IGFBP-3 and subsequent high circulating IGFBP-3 concentration may represent a physiological adaptation to ischaemia. It has been shown that IGFBP-3 activates sphingosine kinase in human endothelial cells and may positively regulate angiogenesis through this pathway. 30
In this study, we also found an association between serum IGF-I, IGFBP-3 and blood Hb concentrations in both genders. Compared with adolescents in the lowest tertile of IGF-I and IGFBP-3 concentrations, adolescents with the top tertile IGF-I and IGFBP-3 were associated with an increased odds of having a top tertile Hb concentration. Both the insulin and IGF-I system belong to the family of growth factors which regulate cellular metabolism and somatic growth in mammals. In this regard, both insulin and IGF-I receptors are expressed ubiquitously, including the pleiotropic stem cells in haematopoietic tissues and pancreatic islets. Given the high degree of homology between these two receptors, both insulin and IGF-I can act via their cognate receptors. However, unlike insulin which binds directly to these receptors, the action of IGF-I is modulated by its high-affinity specific-binding proteins, IGFBPs. IGFBP-3, the principal carrier protein of circulating IGF-I, may regulate red cell metabolism and have direct effects on cell growth and apoptosis, independent of IGFs, as demonstrated in a number of cell lines studies including human breast cells, hepatic cells, colonic epithelial cells and mesenchymal chondroprogenitor cells. 31,32 In support of the hypothesis that high circulating levels of IGFBP-3 may regulate erythropoiesis, there are small-scale clinical studies which have demonstrated a positive association between IGFBP-3 and Hb in human subjects ranging from infants to elderly. 33–38
Interestingly, we have found an association between high IGF-I, IGFBP-3 and serum creatinine in girls of this study cohort. This association is unlikely to be due to reduced renal clearance because all subjects recruited in this study were healthy with normal renal function. In adult patients with type 2 diabetes mellitus and metabolic syndrome, renal function has been reported as one of the non-traditional cardiovascular risk factors. 39 The molecular mechanism underlying the association between the IGF system and renal function remains obscure and further studies are required to explore the association.
A strength of this study is the high quality of the data gathered by a team of experienced research nurses in a Hong Kong territory wide survey. Furthermore, the fact that the study was undertaken in young healthy volunteers, minimized the effect of potential confounding factors such as co-morbidities and medications on IGF activity. Several limitations of this study need to be addressed. Firstly, although puberty may affect IGFBP-3 or IGF-I concentrations, 14 the pubertal state of the participants was not assessed in this study due to the practical difficulties of doing so in such a large cohort. Nonetheless, given that the median age of puberty in Hong Kong is 11.4 years and 9.8 years in boys and girls, respectively, 40,41 the majority of our participants (mean age of 15.3 ± 2.0 and 15.7 ± 2.0 years in boys and girls, respectively) were post-pubertal. Secondly, apart from IGFBP-3, other IGFBPs were not measured in this study. Six IGFBPs have been identified as regulating the effects of IGF-I. For instance, IGFBP-1, the acute regulator of IGF-I bioavailability, is associated with insulin resistance and glucose intolerance in an animal model. 23 IGFBP-2, the second most abundant circulating IGFBP and the principal binding protein secreted by differentiating white preadipocytes during adipogenesis, is shown to protect against insulin resistance and the development of obesity in transgenic mice. 42 However, of the six IGFBPs, IGFBP-3 carries more than 80% of circulating IGF-I and thus the measurement of IGFBP-3 is of primary importance in assessing the biological effects of IGF-I.
In conclusion, in this large cohort of Chinese adolescents, we observed close associations between IGF-I, IGFBP-3, cardiometabolic risk factors and haematological parameters. The independent associations between IGF-I, IGFBP-3, hyperinsulinaemia and Hb in both boys and girls suggest that the IGF-I system may play a linking role in this multifaceted syndrome through its growth-promoting effects on multiple tissues and organs.
DECLARATIONS