
Abstract
Background
A few smaller studies have reported that the prolactin concentration is elevated in connection with heart failure. As heart failure is combined with disturbances of several biological systems any or all of which may also influence prolactin concentrations, we wanted to evaluate the relation of prolactin to prognosis in elderly patients.
Methods
A total of 462 elderly patients from a primary health-care centre, all with symptoms of heart failure, were included. In addition to clinical examination including echocardiography, concentrations of prolactin, macroprolactin, C-reactive protein, thyroid-stimulating hormone and N-terminal pro B-type natriuretric peptide (NT-proBNP) were measured. Patients were then followed for 10 y, and all incidents of cardiovascular mortality were registered.
Results
After excluding patients with macroprolactin, hyperprolactinaemia was found in 3.7% of the patients. There were no differences in prolactin concentrations or in the frequency of macroprolactin between patients with heart failure and those with normal cardiac function, defined as left ventricular ejection fraction of at least 50%. No significant correlation could be found between NT-proBNP and prolactin. Neither could any association be found between cardiovascular mortality and prolactin concentration during 10 y of follow-up.
Conclusions
Prolactin concentrations were not associated with cardiovascular mortality or any clinical or biochemical marker of heart failure. Macroprolactin was found in similar frequency among patients with and without heart failure, and showed no correlation with mortality risk.
Introduction
There is increasing evidence that prolactin is involved in the modulation of the immune system, regulation of electrolyte–water balance and haemostasis.
1,2
There are also indications of a relation between prolactin and cardiovascular disease. Prolactin concentrations are increased in patients with acute coronary syndromes
3
and may also have a direct activating effect on platelets by increasing the stimulatory effect of ADP.
4
However, heart failure (HF) by itself is associated with increased risk for thromboembolism through mechanisms involving disturbed blood flow, defects in endothelial function and increased concentrations of beta-thromboglobulin, fibrinogen and
Methods
The design of the study has previously been described in detail. 14 All patients contacted the primary health centre because of symptoms (tiredness, dyspnoea, peripheral oedema or multiple symptoms). A cardiologist visited the health centre and scrutinized records of patients with the above-listed symptoms. Patients, for whom HF could not be excluded, were invited to participate in the study. A new record was created and a clinical examination was carried out for each patient. The New York Heart Association (NYHA) functional class was evaluated, where class I indicates no limitations at physical activity, class II indicates slight limitation at physical activity, class III indicates limitation of physical activity and finally class IV indicates symptoms of dyspnoea already at rest. Doppler echocardiography was performed and blood samples were taken. During follow-up, all patient mortality was registered and no patients were lost during follow-up. Cardiovascular mortality was defined as death caused by HF, and/or fatal arrhythmia, sudden death, ischaemic heart disease or cerebrovascular disease. As the project had an observational design, no changes in medical therapy were made unless the treating physician decided that. The final study population consisted of 462 patients (240 men, mean age: 71.8 y and 222 women, mean age: 73.4 y). Blood sampling from 112 healthy blood donors (59 men, age range: 21–69 y and 53 women, age range: 19–67 y) was also performed in order to analyse prolactin and macroprolactin in a healthy population without medications. On several occasions, during a four-month period, all registered blood donors coming for blood donation at the university hospital in Linköping were asked to participate in the study.
Echocardiography
Doppler echocardiographic examinations (Accuson XP-128c) were performed on 448 of the 462 patients, with the patient in the supine left position. Both M-mode and 2D methodology were used. Values for systolic function, 15 expressed as ejection fraction (EF), 16,17 were categorized into four classes with interclass limits 30%, 40% and 50%. A semi-quantitative method of assessment was used. Normal systolic function was defined as EF ≥50%. Severely impaired systolic function was defined as EF < 30%.
Laboratory analyses
Blood samples were drawn before noon while the patients were fasting, in a sitting position and after resting for 30 min. Samples for the analysis of N-terminal pro B-type natriuretric peptide (NT-proBNP) were collected in prechilled plastic tubes containing EDTA (Terumo EDTA K-3), placed on ice and centrifuged at 3000
Prolactin
Prolactin was analysed on Elecsys 2010 (Roche Diagnostics, Mannheim, Germany). The method is based on immunochemical detection using two monoclonal prolactin-specific antibodies. The calibrator consisted of recombinant prolactin from Escherichia coli, traceable to the third International Reference Preparation (IRP) WHO reference standard 84/500. After this study was performed, a new prolactin method (Prolactin II) was developed for Elecsys with lower reactivity against macroprolactin. The coefficients of variation (CV) for this method, as measured by internal controls on two concentrations during a three-month period, were 6.4% (concentration: 180 mU/L) and 5.8% (concentration: 1050 mU/L). Results >510 mU/L were regarded as hyperprolactinaemia. Because all women were of postmenopausal age, the same reference interval was used for men and women.
18
Precipitation with polyethylene glycol (PEG) was performed mainly according to Olukoga and Kane
19
following a protocol recommended by Roche.
20
All patients' samples having prolactin concentration greater than 200 mU/L were further treated with 25% PEG v:v 1:1 to precipitate macroprolactin (n = 254). The concentration of 200 mU/L was chosen arbitrarily on the basis of low probability of macroprolactinaemia and to avoid misclassification because of high imprecision at low concentrations. The samples were centrifuged at 1800
NT-proBNP
In the study, the Elecsys 2010 (Roche Diagnostics) NT-proBNP assay, first described by Karl, was used. 21 This assay utilizes two polyclonal antibodies directed against amino acids, 1–21 and 39–50, and electrochemiluminescence detection. The analytical range was 0.6–4130 pmol/L (5–35.000 ng/L). Total CV was 4.8% for a concentration of 26 pmol/L (217 ng/L, n = 70) and 2.1% for a concentration of 503 pmol/L (4261 ng/L). According to the European Society of Cardiology Guidelines for the diagnosis and treatment of HF, the diagnosis is unlikely with a plasma concentration of NT-proBNP <400 ng/L (116 pmol/L). 22
Other laboratory analyses
C-reactive protein (CRP) was measured by a turbidimetric high-sensitivity method with antibodies from Siemens Medical Solutions Diagnostics AB (wrCRP) on Advia 1650 (Bayer, Leverkusen, Germany). The limit of detection was 0.1 mg/L.
Thyroid-stimulating hormone (TSH) was measured by an immunochemical method on AutoDELFIA automatic immunoassay system (PerkinElmer, Turku, Finland). The reference range is 0.4–4.0 mU/L.
Statistics
The Mann-Whitney U test was used to examine the significance of difference between groups. Correlation between different parameters was examined by calculating Spearman rank order correlation coefficient (r). To compare groups with different levels of EF, the Kruskal–Wallis analysis of variance test was used. Chi-square test was used to compare the frequency of hyperprolactinaemia and macroprolactinaemia between groups. Multiple regression analysis was used to identify if a predictive power of the dependent variable could be found. Cox proportional hazard regression analyses as well as a Kaplan–Meier analysis were used to analyse the risk of mortality during the follow-up period. Clinical variables known to influence the risk of mortality in an elderly population were included in the multivariate settings used. A P value less than 0.05 was considered statistically significant. All data were analysed using generally available statistical analysis software packages (Statistica v. 8.0, Statsoft Inc, Tulsa, OK, USA).
Results
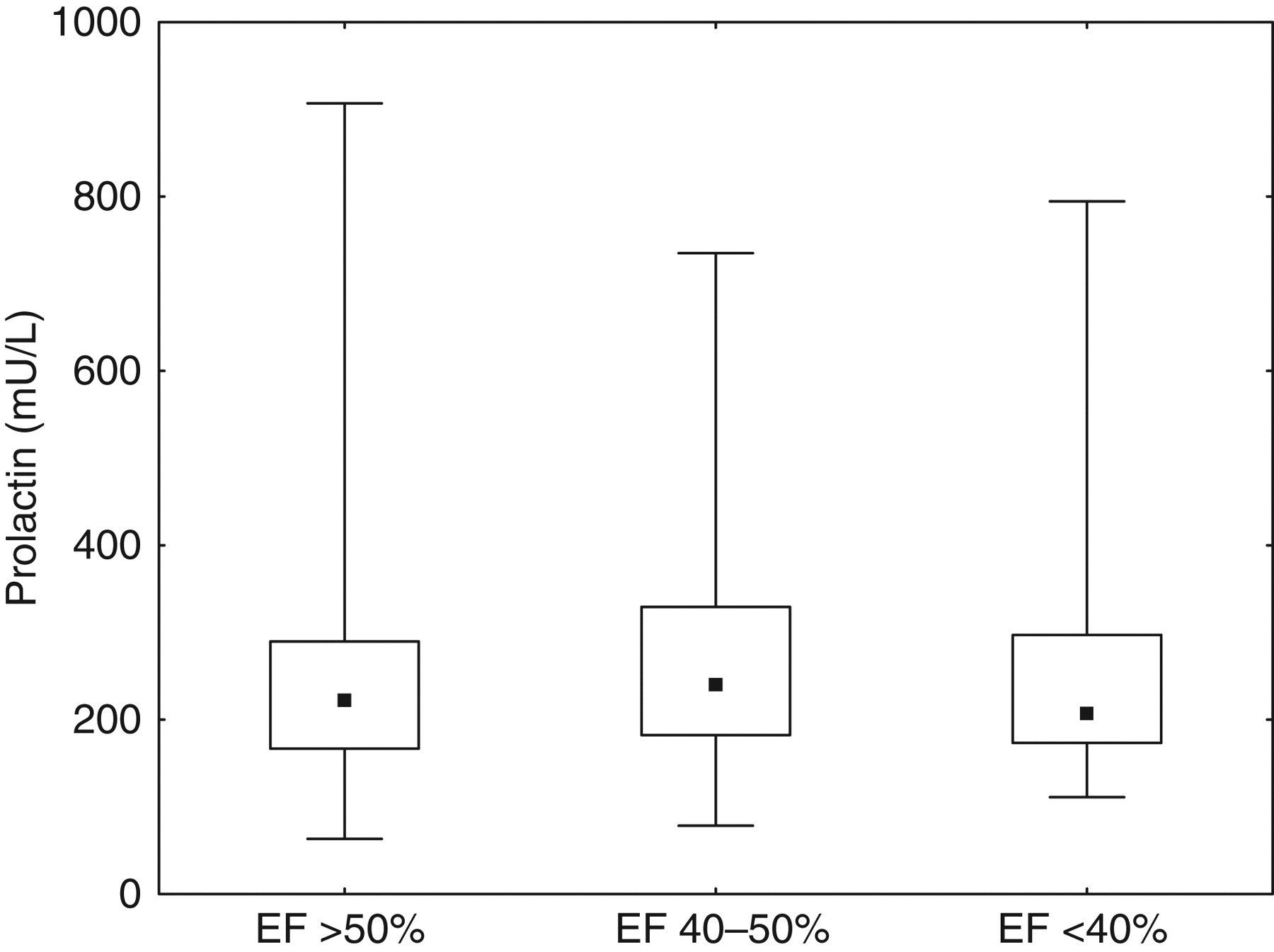
Basal characteristics of the study population are demonstrated in Table 1. When left ventricular EF was determined by echocardiography examination, 23% (n = 108) of the patients were found to have decreased EF (<50%) and 12% with EF less than 40%. The main interest was focused on prolactin. It was measured in samples from all patients in the study population. Initially, patients with true or inconclusive macroprolactinaemia were excluded from the next evaluation of the material. After this exclusion, the total frequency of the occurrence of hyperprolactinaemia defined as prolactin >510 mU/L was 3.7%. No significant difference in the frequency of hyperprolactinaemia between patients with normal EF (>50%) and patients with moderately or severely impaired EF (chi-square: 1.67, P = 0.20) was found. Serum prolactin showed no correlation with NT-proBNP (r = 0.05, P = 0.29, Figure 1). In addition, no significant differences in the prolactin concentration between the group of patients with normal EF and the two groups with impaired EF were found (Figure 2). A number of other parameters were assessed and analysed concerning the influence of other factors on prolactin concentrations (Tables 2 and 3). First groups for each parameter were compared by the Mann-Whitney U test (Table 2). Smokers as a group had lower prolactin values than non-smokers (P < 0.01). The median difference, however, was small (30 mU/L). Values of NT-proBNP, CRP and TSH were divided into quartiles. A significant difference between groups was found for CRP, but with a median difference of only 16 mU/L (P < 0.05). There was no significant correlation between CRP and prolactin (r = 0.093, P = 0.056). A multivariate setting was analysed as well (Table 3).
Correlation between prolactin and NT-proBNP. Extreme values are not shown in the figure. NT-proBNP, N-terminal pro B-type natriuretric peptide Box plots showing the distribution of prolactin in groups of patients with normal or decreased left-ventricular ejection fraction (EF). The point label indicates the median. The boxes indicate the 25th to the 75th percentiles and the bars indicate range (one extreme prolactin value was excluded) Basal characteristics of the study population BMI, body mass index; NYHA, New York Heart Association; EF, ejection fraction by echocardiography; SD, standard deviation; NT-proBNP, N-terminal pro B-type natriuretric peptide; CRP, C-reactive protein; TSH, thyroid-stimulating hormone Difference in prolactin concentration, comparing two groups per variable EF, ejection fraction; NT-proBNP, N-terminal pro B-type natriuretric peptide; TSH, thyroid-stimulating hormone; CRP, C-reactive protein *P < 0.05 Multiple regression analysis using prolactin as dependent variable against selected clinical independent variables BMI, body mass index; EF, ejection fraction; HT, hypertension; IHD, ischaemic heart disease; NYHA, New York Heart Association functional class; CRP, C-reactive protein; NT-proBNP, N-terminal pro B-type natriuretric peptide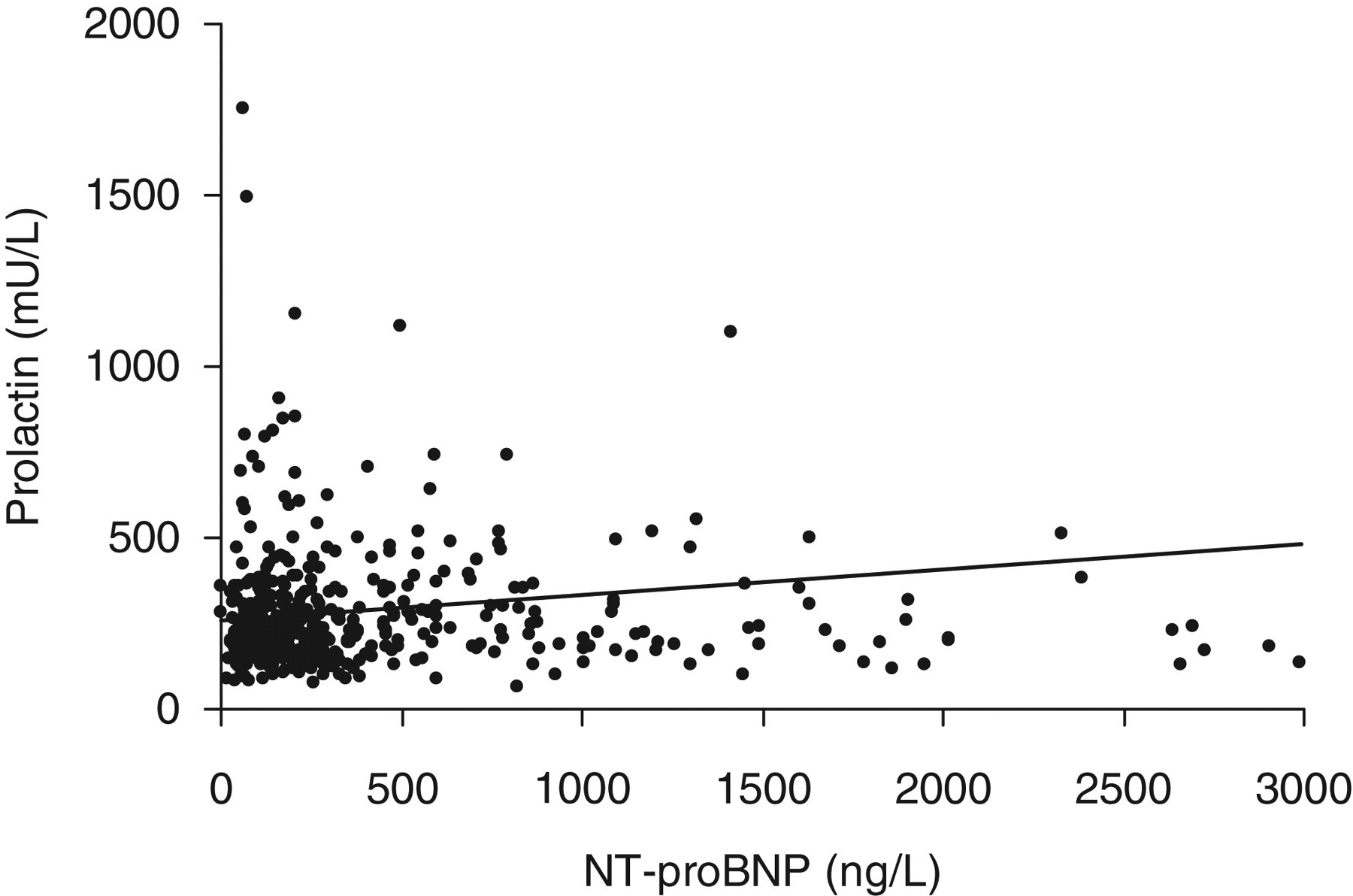
Macroprolactin
After PEG precipitation 3.0% (n = 14) of the samples had a recovery of prolactin less than 40%, indicating true macroprolactinaemia. There was no significant difference between gender (men: 3.3%, women: 2.7%). Additionally 3.5% (n = 16) of the patients had recoveries between 40% and 60%, which were regarded as inconclusive results. Most of the samples indicating true macroprolactinaemia showed prolactin values above the upper reference limit (12 out of 14 samples). There were no significant differences in the frequency of macroprolactinaemia between the group of patients with normal EF and the patients with decreased EF (chi-square: 1.48, P = 0.22). To compare the frequency of macroprolactin in HF patients with the occurrence in a healthy population, samples from 112 healthy blood donors were also analysed. All blood donors were normoprolactinaemic and all samples precipitated with PEG showed recoveries of more than 40%, thus indicating a lower frequency of macroprolactin than in the patient group. However, 1.8% (n = 2) of the samples had a recovery between 40% and 60% after PEG precipitation. The difference between groups was almost significant (chi-square: 3.48, P = 0.06).
Cardiovascular mortality
After 10 y of follow-up, 114 patients had died of cardiovascular causes. Cardiovascular mortality was not correlated with hyperprolactinaemia (macroprolactin excluded), odds ratio 1.15 (95% confidence interval 0.36–3.69) nor macroprolactinaemia, odds ratio 0.77 (95% confidence interval 0.30–1.94). A Kaplan–Meier analysis evaluating the fourth versus the first quartile of plasma concentration of prolactin, followed over 10 y, is presented in Figure 3. No significant differences between the groups could be seen. In the Cox proportional hazard regression analysis including some clinical variables known to potentially influence the risk of cardiovascular events, no predictive power of prolactin, either in the fourth quartile (Table 4) or in the first quartile (data not shown) against the other three quartiles could be demonstrated.
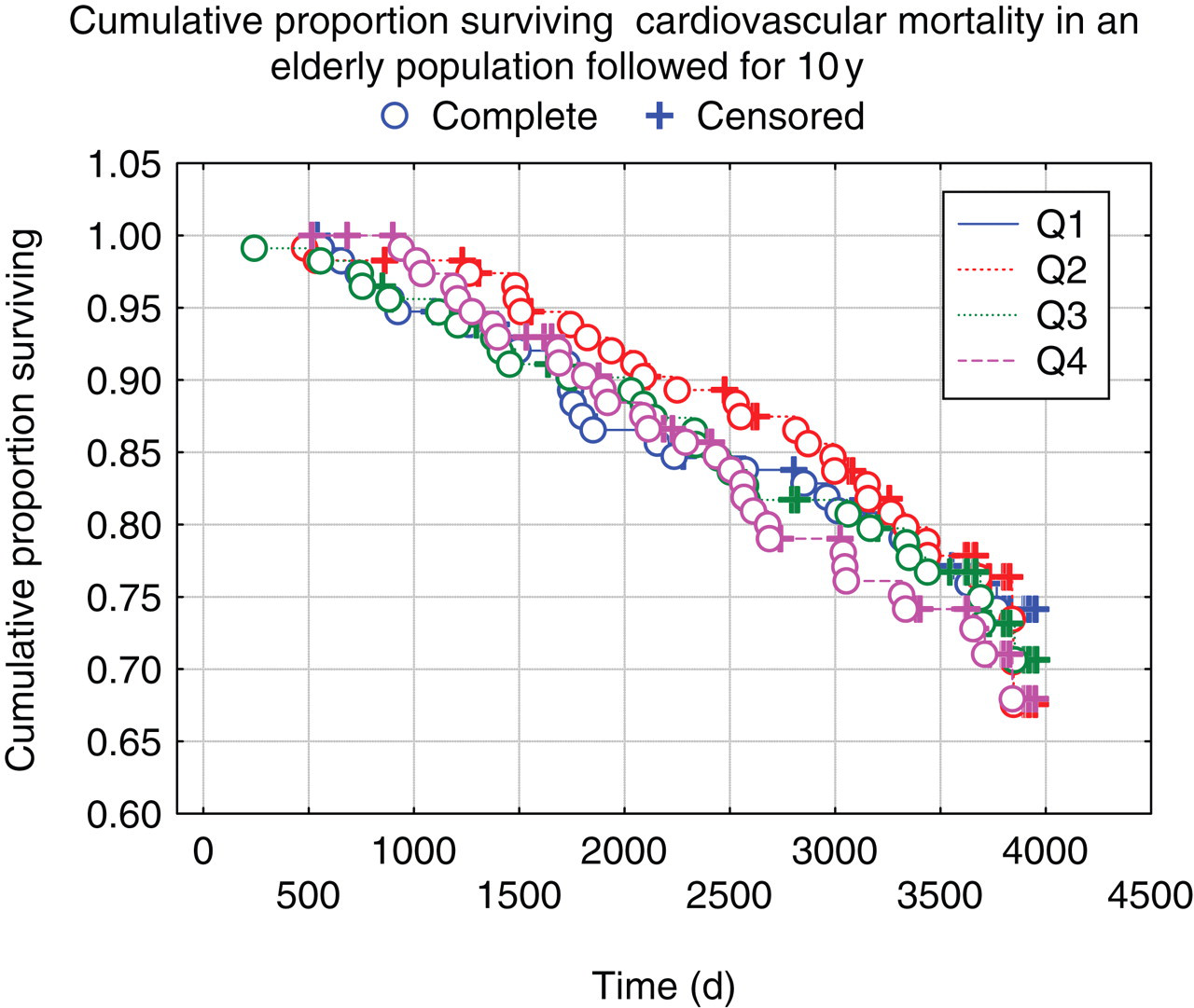
Kaplan–Meier analysis of the four quartiles of prolactin (Q1–Q4) concerning cardiovascular mortality in an elderly population followed during 10 y. Please see online for colour version
Multivariate Cox proportional hazard regression analysis concerning cardiovascular mortality in an elderly population followed during 10 y
EF, ejection fraction; IHD, ischaemic heart disease; NYHA, New York Heart Association functional class; CRP, C-reactive protein; NT-proBNP, N-terminal pro B-type natriuretric peptide
Discussion
Prolactin is a hormone with several biological functions. Specifically, effects on renal regulation of sodium reabsorption, blood volume 23,24 and interactions with platelet activation 4,25 may have implications in ischaemic heart disease and HF. Earlier reports have claimed an increased frequency of hyperprolactinaemia among patients with HF. 7,8 However, the number of patients in these two studies was small (55 in one, 27 in the other), and the patient ages and aetiology of HF differed from our study. A larger study with patients suffering from HF was therefore needed. We analysed prolactin in a group of 462 elderly patients suffering from symptoms associated with HF. In this population, no changes in prolactin were connected to HF. Neither echocardiographic measurements nor plasma concentration of NT-proBNP showed any significant correlation with prolactin concentration in blood. In addition, the frequency of hyperprolactinaemia was not different from patients without HF according to echocardiography. Wallaschofski et al. found normal prolactin values in a group of patients with chronic HF (n = 50), together with a lack of correlation between prolactin and EF. 26 Limas et al. found a higher frequency of hyperprolactinaemia than in our study, 25% compared with 6.7%. 7 In contrast to our study, the patients were younger (48 ± 7 y) but were similarly under medical treatment during sampling. After excluding patients with macroprolactin, only 3.7% of the patients in our study showed hyperprolactinaemia. In the other three studies, 7,8,26 patients with macroprolactinaemia were not excluded and it is not clear to what extent the methods used are susceptible to this interference. Macroprolactin may have led to false conclusions. The patients in these other studies had mainly severely impaired heart function (EF less than 35%), in contrast to this study, where most patients suffered from mild to moderate HF. Although both Opalinska et al. 8 and Limas et al. 7 found a significant correlation between prolactin and EF, the correlations showed opposite directions., The former study found increased prolactin with decreased EF, whereas in the latter study there was significant higher EF in the group of patients with hyperprolactinaemia compared with those with HF and normoprolactinaemia. In addition, the other studies have not corrected for other clinical variables, as for example, smoking or thyroid status, which may cause confounding effects. Because our study was based on elderly patients from primary health care, other diagnoses such as diabetes and hypertension were relatively common. A number of parameters with possible correlation to prolactin were therefore included in the statistics. Although no significant differences were found for gender, diabetes or thyroid status, the prolactin concentration was significantly lower in smokers than in non-smokers. This relationship has also been encountered in previous studies. 27,28 Macroprolactin comprises a complex of prolactin and immunoglobulin. Most evidence points towards macroprolactin having no biological effect in vivo. 11–13 One explanation of this is low bioavailability caused by the large size of macroprolactin. However, it has not been evaluated whether macroprolactin may exert effects on cells present within the blood vessels. In this elderly population, 3.0% of the individuals were found to have macroprolactin. The frequency of macroprolactin was found to be higher in this group compared with a group of younger healthy blood donators. However, no association of macroprolactin and HF was found in the patient group. This indicates that the presence of macroprolactin may simply be related to increased age. In a previous study, using the same type of immunoassay (dissociation enhanced lanthanide fluorescent immunoassay [DELFIA]) as in our study, a healthy population consisting of 380 women and 280 men (ages 20–65 y) were screened for macroprolactinaemia. 29 Only one woman was found to have macroprolactinaemia. However, these authors only examined the presence of macroprolactin in serum with prolactin values above 1000 mU/L, whereas in this study, all samples with prolactin above 200 mU/L were examined by PEG-precipitation. Recently, Hattori et al. 30 found a frequency of macroprolactin of 3.7% in a group of 1330 hospital workers, which is similar to our patient group. They also found that macroprolactinaemia was more frequent in elderly subjects.
In this study, we focused on patients with HF mainly caused by atherosclerotic heart disease. This is a group of patients having increased risk for thromboembolic events and cardiovascular death. However, there was no correlation between prolactin and cardiovascular mortality after 10 y follow-up, either in the patient group with HF or in the group without HF. Furthermore, in our study, the presence of macroprolactin was not correlated to cardiovascular mortality risk, supporting the view that macroprolactin has little or no pathophysiological role. 11,12,31 In summary, these findings indicate that the secretion of prolactin to blood is mainly unaffected by changes in the haemodynamic and biochemical disturbances associated with mild-to-moderate HF. Prolactin concentrations were not found to be usable in making prognoses, and prolactin was not associated with cardiovascular mortality. Furthermore, macroprolactin was found in similar frequency among patients with and without HF, and showed no correlation with mortality risk.
DECLARATIONS