
Abstract
Background
Some familial amyloidotic polyneuropathy (FAP) patients show the post-transplant progression of the clinical symptoms. Although the presence of recipient-derived cells in transplanted livers has been reported, no studies investigating the functional significance of this post-transplant chimerism in transplanted FAP patients were performed. The aims of this study were to evaluate amyloidogenic transthyretin (ATTR) production of recipient-derived cells and the relationship between the protein from recipient-derived cells and the progression of FAP symptoms after liver transplantation (LT).
Methods
Seven FAP ATTR Val30Met patients who underwent LT were included in this study. In one male patient with sex-mismatched donor, fluorescence in situ hybridization (FISH) method was performed on a liver biopsy sample using DNA probes for visualizing X and Y chromosomes to detect the recipient-derived cells. In three patients including the FISH-analysed patient, ATTR mRNA expression in transplanted livers was evaluated by the polymerase chain reaction (PCR)–restriction fragment length polymorphism method and realtime quantitative reverse transcription–PCR. In five of the seven patients, ATTR in serum protein expression was measured by mass spectrometry.
Results
One FAP patient has 3.1% recipient-derived cells in the transplanted liver. The ATTR mRNA was not expressed in any of the three transplanted livers. The ATTR was not detected in any sera of the sampled patients.
Conclusion
Although the FAP patient had recipient-derived cells in the transplanted liver, the recipient-derived cells did not contribute to the production of ATTR in our specific case. The effect of recipient-derived cells on the post-transplant progression of FAP symptoms may be negligible.
Introduction
Familial amyloidotic polyneuropathy (FAP) is a disease, inherited in an autosomal dominant fashion, that is caused by mutant transthyretin (TTR). 1,2 The disease is characterized by sensory-dominant peripheral neuropathy, as well as symptoms in the gastrointestinal tract, heart, eyes, kidneys and autonomic nervous system. 3–6 More than 90 amyloidogenic transthyretin (ATTR) mutations leading to FAP have been reported. 7 Of those, Val30Met is the most common type mutation. TTR is produced by the liver, retinal pigment epithelium, choroid plexus and alpha cells of the pancreas. Because the liver synthesizes more than 90% of serum TTR, 8,9 liver transplantation (LT) has been performed to treat FAP since 1990. LT is now considered as a promising therapy to halt the progression of clinical symptoms in FAP. 9,10 However, it was reported that some FAP patients showed progression of FAP symptoms even after LT, 11–14 while the mechanism remains to be elucidated.
There is a possibility that the recipient-derived cells in transplanted liver have impact on the progression of FAP symptoms after LT. The presence of microchimerism was reported in transplanted livers and in other transplanted organs. 15–17 Chimerism is defined as cell migration from the host to the transplanted organ. The mechanism of microchimerism was reported to be transdifferentiation and/or cell fusion of bone marrow cells. 18–20 Many reports have been published on the presence of microchimerism in transplanted liver. 21,22 It was reported that transplanted livers have recipient-derived cells and these cells play a role in liver regeneration. 21–23 In FAP cases, if transplanted liver has recipient-derived cells in FAP patients, these cells have a possibility to produce ATTR, which may cause the progression of FAP symptoms. However, there have been no studies investigating recipient-derived cells in FAP patients.
The aims of this study were to evaluate the protein production of recipient-derived cells and the impact of recipient-derived cells on the progression of FAP symptoms after LT. We evaluated recipient-derived cells in transplanted FAP patients by fluorescent in situ hybridization (FISH). We also evaluated the serum ATTR concentration and ATTR mRNA expression in transplanted liver in FAP patients.
Patients and methods
We performed a retrospective study of seven Japanese FAP ATTR Val30Met patients in Kumamoto University Hospital who underwent LT from 1994 to 2008 (Table 1). All FAP patients in this study had a definite diagnosis of FAP on the basis of genetic investigations and clinical manifestations of FAP. All patients had standard immunosuppression with tacrolimus or cyclosporine and corticosteroids with or without mycophenolate mofetil (Table 1). We evaluated preoperative factors, graft types and the changes of clinical manifestations after LT by retrospective analysis of medical charts (Table 1). The patient who has sex-mismatched donor and shows the typical progression would be an ideal and a suitable case to evaluate the effect of recipient-derived cells. Especially, Patient 4 was the ideal and suitable case. Therefore, we focused on Patient 4. Two frozen autopsy samples of Patient 1 and Patient 2 and one frozen biopsy sample of Patient 4 were used to evaluate the ATTR mRNA expression in the transplanted livers. In three patients including the FISH-analysed one, the expression of ATTR Val30Met mRNA in transplanted livers was evaluated using the polymerase chain reaction–restriction fragment length polymorphism (PCR–RFLP) method and realtime quantitative reverse transcription–polymerase chain reaction (RT–PCR) method. In five of the seven patients, ATTR in sera was measured by using matrix-assisted laser desorption ionization/time-of-flight mass spectrometry (MALDI/TOF-MS).
Characteristics of transplanted FAP patients
mBMI, modified body mass index; M, male; F, female; MMF, mycophenolate mofetil; FK, tacrolimus; CsA, cyclosporine
*The dosage of prednisolone was gradually reduced and discontinued after liver transplantation
The ethical committee at Kumamoto University School of Medicine approved this study and informed consent was obtained from patients after explanation about this study.
Fluorescent in situ hybridization
The biopsied liver of Patient 4 at seven years after LT was analysed. FISH was performed in Nihon Gene Research Laboratories. Formalin-fixed paraffin-embedded sections were sectioned at 6 μm. The sections were prepared for FISH by the NaSCN incubation, denaturation and proteinase K digestion steps, one after the other. After the last formamide denaturation, the slides were dehydrated in graded ethyl alcohols and air-dried. FISH was performed on pretreated slides using spectrum green-labelled DXZ1 probe (Vysis, Downers Grove, IL, USA) and spectrum red-labelled DYZ1 probe (Vysis) for labelling X and Y chromosomes. Probe-applied, covered and sealed slides were denatured on hot plate and hybridized overnight at 37°C using a hybrid incubation chamber (Vysis). DAPI was performed for nuclear counter-staining.
Determination of TTR using MALDI/TOF-MS
We examined the presence of ATTR Val30Met in sera of five post-transplanted FAP patients. Fifty microlitres of test serum were mixed with 10 μL of 2.7 mmol/L dithiothreitol and 20 μL of an anti-TTR polyclonal antibody (DAKO, Glostrup, Denmark). TTR in the serum was isolated as described by Ando et al. 24,25 All experiments were performed using a Bruker Reflex mass spectrometer (Bruker Franzen Analytik GmbH, Bremen, Germany), operated at a wavelength of 337 nm. The isolated TTR was assayed as described previously. 26
Isolation of RNA and reverse transcription
Total RNA was extracted from each frozen samples using the RNeasy Mini Kit Isolation System (Qiagen, Hilden, Germany) according to the manufacturer's protocol. RNA was quantified by spectrophotometric analysis using the NanoDrop ND-1000 spectophotometer (NanoDrop Technologies, Wilmington, DE, USA). The RNA was reverse-transcribed into complementary DNA (cDNA) by one cycle at 37°C for 15 min followed by one cycle at 85°C for five seconds using PrimeScript RT reagent kit (Takara Bio, Shiga, Japan).
Polymerase chain reaction–restriction fragment length polymorphism
The generated cDNA was used as the template in realtime PCR reactions. PCR primers were designed to amplify the Val30Met mutation in exon 2 of the TTR gene. Primers were: forward 5′ CATTCTTGGCAGGATGGCTTC 3′ and reverse 5′ CTCCCAGGTGTCATCAGCAG 3′. The PCR conditions were five minutes at 98°C; 35 cycles of 94°C for 30 s, 55°C for 30 s and 72°C for one minute; followed by seven minutes at 72°C. The PCR product of 199 bp was digested with 5 U NsiI restriction enzyme (New England Biolabs, Hitchin, UK) that recognized mutation site at 37°C for two hours. PCR products were then separated on 3.5% NuSieve GTG agarose gel (BMA Products, Rockland, ME, USA) by electropheresis in 1× TBE buffer, approximately two hours at 50 V. The expected PCR products are visualized using SYBR SafeTM DNA Gel Stain (Invitrogen, Carlsbad, CA, USA). PCR products were evaluated using microchip electrophoresis system (Cosmo-I SV1210; Hitachi Electronics Engineering, Tokyo, Japan) too. Measurement was according to the manufacturer's manual.
Real-time quantitative RT–PCR
The generated cDNA was used as the template in realtime PCR reactions. Realtime PCR primers were designed to amplify the Val30Met mutation of the TTR gene. Primers were: forward 5′ CTCTGATGGTCAAAGTTCTAGATGCT 3′ and reverse 5′ GTGTCATCAGCAGCCTTTCTG 3′. We used FAM-labelled TaqMan probe and VIC-labelled TaqMan probe to detect the Val30Met TTR gene and wild-type TTR gene, respectively. Val30Met TTR-specific FAM-labelled TaqMan probe was 5′ FAM-AATGTGGCCATGCAT 3′. Wild-type TTR-specific VIC-labelled TaqMan probe was 5′ VIC–CAATGTGGCCGTGCAT 3′. The realtime PCR conditions were two minutes at 50°C, 10 min at 95°C; 40 cycles of 95°C for 15 s, 65°C for one minute. Realtime RT–PCR was performed with TaqMan Genotyping Master Mix (Applied Biosystems, Foster City, CA, USA) according to the manufacturer's protocol. Realtime PCR for wild-type and Val30Met TTR mRNA was validated on the Applied Biosystems 7500 RealTime PCR system according to the manufacturer's instructions. 50:50, 90:10, 98:2, 99.6:0.4, 99.92:0.08 and 100:0 of wild-type TTR genes and ATTR Val30Met genes served as standards for analyses of TTR mRNA expression ratio in transplanted liver.
Results
Clinical outcome
Table 1 presents preoperative factors, graft types and the changes of clinical manifestations after LT. Patient 1 and Patient 2 received whole liver grafts from deceased donors. Patient 1 showed the progression of cardiac symptoms even after LT. He underwent pacemaker implantation eight years after LT due to complete atrioventricular block. In addition, although the ocular manifestation was not observed before LT, he developed mild degree of vitreous opacity in his right eye 12 y after LT. He did not show the progression of neuropathy after LT and died of hypokalaemia-induced pulseless ventricular tachycardia caused by alcoholism 13.8 y after LT. Patient 2 showed the progression of cardiac symptom too. She underwent pacemaker implantation five years after LT due to heart failure. Because the progression of vitreous opacity and glaucoma was observed, she underwent trabeculectomys seven and eight years after LT and vitrectomy nine years after LT. She did not show the progression of neuropathy after LT and died of severe congestive heart failure with cardiac liver cirrhosis 9.2 y after LT. Patients 3, 5, 6 and 7 did not show the progression of FAP symptoms. Patient 4 received the right lobe graft from the living donor and underwent liver biopsy seven years after LT. The donor was his daughter without pregnancy history. He showed the granular sparkling echo and circumferential ventricular wall thickening with echocardiography four years after LT and developed symptoms of heart failure. He underwent pacemaker implantation five years after LT due to trifascicular block. He underwent liver biopsy to check his liver, because he had ascites and pleural effusion seven years after LT. The transplanted liver was almost normal according to the results of biopsy. These results showed that the cardiac amyloidosis caused the ascites and pleural effusion and cardiac symptoms progressed after LT. He showed the progression of neuropathy and deterioration in nerve conduction velocity gradually after LT. In addition, because he also exhibited the progression of vitreous opacity, he underwent anterior vitrectomy of his right eye three years after LT and vitrectomy of his left eye four years after LT.
Recipient-derived cells in liver allograft
FISH analysis was performed in Patient 4 with sex-mismatched donor to evaluate the ratio of recipient-derived cells in transplanted liver. There were 31 cells that had XY signals out of 1000 cells in his transplanted liver, indicating that his transplanted liver had 3.1% recipient-derived cells seven years after LT (Figure 1).
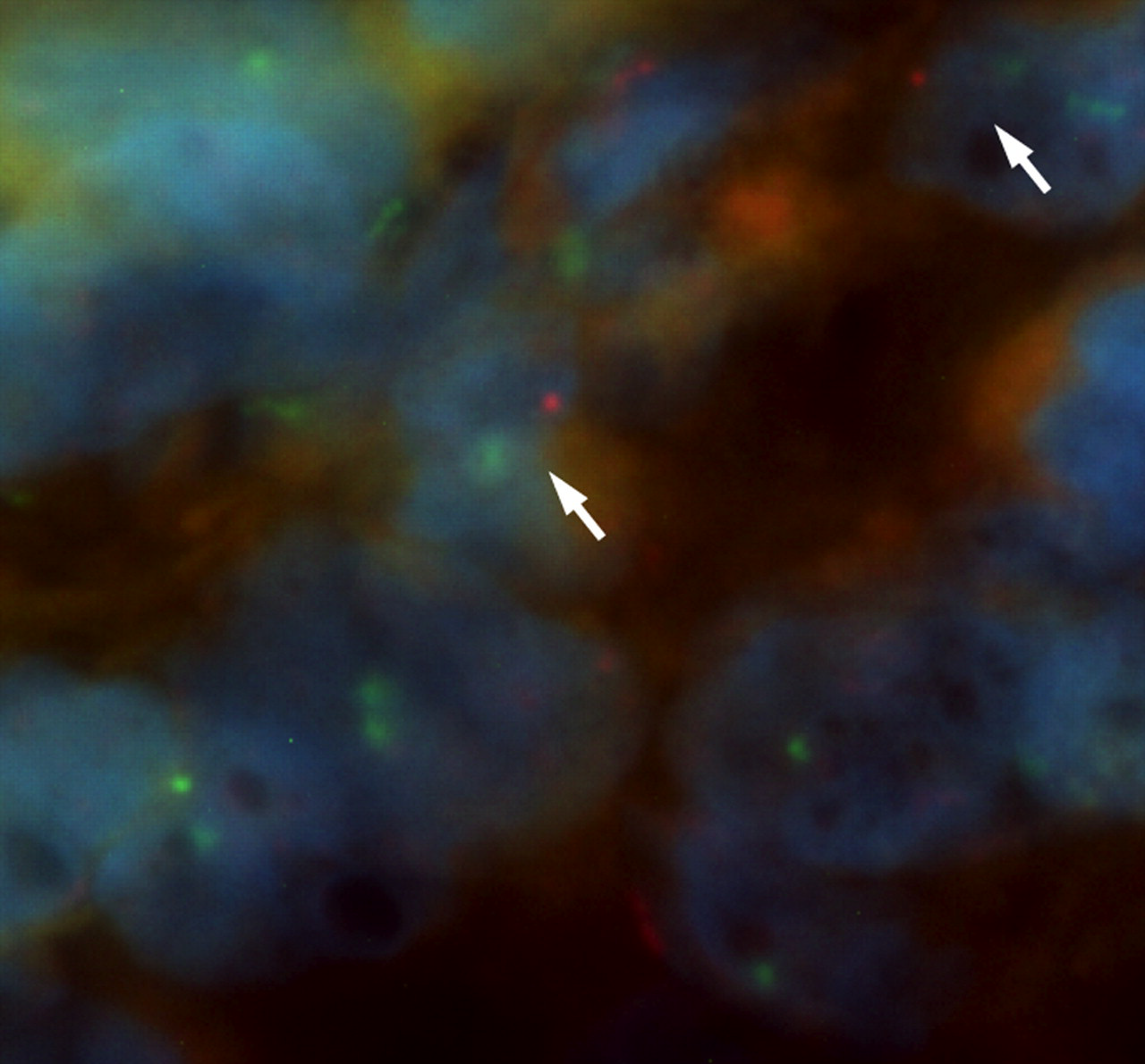
Presence of recipient-derived cells is confirmed in the liver biopsy sample of male familial amyloidotic polyneuropathy recipient with sex-mismatched donor. Nuclear red spots were interpreted as Y chromosomal signal and green spots as X chromosomal signals. Recipient-derived cells (arrow) were detected in the transplanted liver. See online for colour version
Serum ATTR in FAP patients after LT
TTR in sera of five transplanted FAP patients was measured by MALDI/TOF-MS to evaluate the serum ATTR after LT. The results of a FAP patient before LT, as a positive control, and Patient 4 were shown in Figure 2. While the peak of approximately 13,761 kDa of wild-type TTR was detected, the peak of ATTR Val30Met was not detected in Patient 4. Other transplanted FAP patients did not exhibit the peak of ATTR Val30Met.
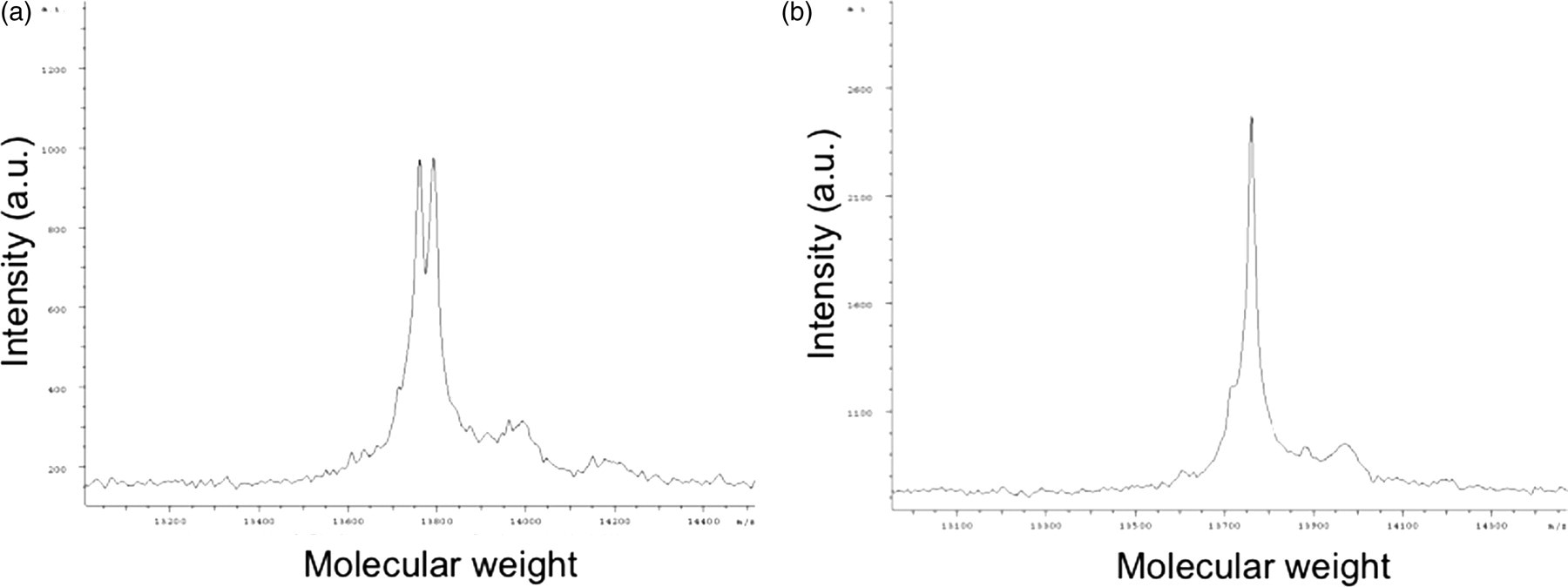
Analysis of TTR forms by MALDI/TOF-MS in the serum of FAP patients. (a) A FAP patient before LT as a positive control. The peaks of 13,761 and 13,792 kDa were free forms of wild-type TTR and ATTR Val30Met, respectively. (b) Patient 4 after LT. The peak of 13,761 kDa was free form of wild-type TTR. The peak of ATTR was not detected. TTR, transthyretin; MALDI/TOF-MS, matrix-assisted laser desorption ionization/time-of-flight mass spectrometry; FAP, familial amyloidotic polyneuropathy; LT, liver transplantation; ATTR, amyloidogenic transthyretin
ATTR Val30Met mRNA expression in transplanted livers
ATTR mRNA concentrations in transplanted livers were evaluated by using PCR–RFLP and realtime quantitative RT–PCR to elucidate the ATTR expression of recipient-derived hepatocytes. In three transplanted livers, PCR–RFLP analysis revealed wild-type TTR mRNA expression, but not ATTR Val30Met mRNA expression in transplanted livers.
ATTR mRNA expression in transplanted livers was evaluated by using realtime quantitative RT–PCR to elucidate the ATTR production of recipient-derived hepatocytes more sensitively. Delta threshold cycle (Ct) value was calculated by taking Ct of wild-type TTR from that of Val30Met ATTR in realtime quantitative RT–PCR. The chart of standard curve that has delta Ct scale and logarithmic scale of mixing ratio was made. The approximation of standard curve was expressed as follows: Y = −15.35 ln(X) + 33.218. Using purified wild-type and ATTR Val30Met DNAs, we verified approximately 0.1% ATTR Val30Met mRNA expression at the lowest level. However, in three transplanted livers, ratio of ATTR mRNA expression was calculated by the approximation (Table 2, see the Supplemental Figure 1 at
ATTR Val30Met mRNA expression
BD, below the detectable level
Discussion
The results of this study indicate that the transplanted liver had recipient-derived cells that did not produce ATTR. Although the progression of FAP symptoms after LT has been reported, 11–14 the effect of recipient-derived cells on the progression of FAP have not been reported until now. If recipient-derived cells have some effects on the progression, we need to consider the way of inhibition for the recipient-derived cells. Therefore, we enrolled FAP patients with or without progression of symptoms in our study.
In this study, the presence of recipient-derived cells in transplanted liver was first confirmed in the FAP patient by using FISH analysis, indicating that microchimerism occurred in the FAP patient after LT. Although FISH analysis was performed in only one FAP patient, the presence of recipient-derived cells was also confirmed with almost the equal frequency of previous reports in other diseases. 21,22 However, despite the presence of recipient-derived cells, our results showed that ATTR mRNA was not expressed in the transplanted liver and serum ATTR could not be detected. Previous studies reported that hepatocyte transdifferentiation from recipient bone marrow stem cells was rare, 27–30 suggesting that the recipient-derived cells in the transplanted liver may be too immature to synthesize TTR. In addition, previous studies have also shown that the recipient-derived cells transdifferentiated into cholangiocytes or vein endothelium cells in transplanted livers, 21,30–33 implying that the recipient-derived cells may transdifferentiate into non-hepatocytes. Because the sample was limited in this study, further investigation will be needed to identify the type of recipient-derived cells by multiple methods such as immunohistochemical staining for hepatocyte marker. Taken together, in the view of microchimerism, values of LT for FAP patients were revalidated by showing that recipient-derived cells did not produce ATTR in our cases. However, because transplanted liver actually had recipient-derived cells in FAP patients, it still remains possible that these recipient-derived cells may have impact on the progression of FAP symptom in some FAP patients. Furthermore, the transplanted FAP patient who showed the progression and had sex-mismatched donor was very rare. We need to analyse FAP patients in more number hereafter.
Although it has been reported that some FAP patients showed progression of FAP symptoms even after LT, the mechanism remains to be elucidated. In this study, our data did not confirm the effect of recipient-derived cells on the progression of FAP. It is well documented that TTR was produced by different organs, such as retinal pigment epithelium, choroid plexus and alpha cells of the pancreas. Even though ATTR concentrations were not detectable in our study, the trace amount of ATTR from extrahepatic organs may contribute to the progression of FAP symptoms after LT. In addition, because the part of amyloid deposits in some organs has been proven to be derived from the wild-type TTR, the TTR may have some impact on the progression of FAP symptoms after LT. Further investigations will be needed to clarify the detail mechanism of the progression of FAP symptoms after LT.
Another interesting finding in this study is that LT in FAP has possibility to be a unique and natural human model to evaluate the recipient-derived transdifferentiated hepatocytes by detecting ATTR gene or protein functionally, because only recipient-derived hepatocytes can express ATTR gene. Previously, the presence of recipient-derived hepatocytes was usually shown by sex-mismatch analysis. 21,22 FISH and immunohistochemical staining methods on transplanted tissues in sex-mismatched individuals cannot fully evaluate the function of recipient-derived cells. It is well documented that not only albumin but also TTR is produced by differentiated hepatocytes. If recipient-derived cells transdifferentiate to hepatocytes in heterozygous FAP patients, these recipient-derived hepatocytes should produce both wild-type TTR and ATTR. We could not detect the expression of ATTR Val30Met in this study. This result may imply that the recipient-derived cells did not transdifferentiate to hepatocytes in our cases. Although we need to study in more transplanted FAP patients, we might provide a new tool to evaluate functional chimerism in transplanted livers. However, because our data do not exclude the possibility that ATTR mRNA expression and serum ATTR protein concentrations were too low to be detected, we need to evaluate ATTR expression by a more sensitive method such as radioimmunoassay procedure. 34
In conclusion, although it was confirmed that the FAP patient had recipient-derived cells in the transplanted liver in our series, the recipient-derived cells did not contribute to the production of ATTR. Although the case volume was small, our study suggests that microchimerism do not have effect on the progression of FAP symptoms after LT in our cases. Our results provide one milestone into LT in FAP patients.
DECLARATIONS