
Abstract
Central pontine myelinolysis (CPM) is a demyelinating disorder, which is associated most commonly with the rapid correction of hyponatraemia and other abrupt changes in physiological osmotic conditions. This includes the treatment of hyperosmolar hyperglycaemia in diabetes mellitus (DM) sufferers. Herein, we report a case of CPM in a 55-y-old patient with new-onset DM who presented with partial focal seizures and a sudden-onset right-sided hemiplegia. Magnetic resonance imaging revealed a lesion in the central pons. The patient responded to glucose control and antiepileptic medication, and achieved a recovery of limb function within 17 d of admission. CPM occurred in this patient before the correction of hyperglycaemic hyperosmolar state, and a disturbance in his initial electrolytes was not found. This report is the first documented case of long-term hyperglycaemic hyperosmolar state leading to CPM, and highlights that CPM can present as an isolated hemiplegia.
Introduction
Central pontine myelinolysis (CPM) is a demyelinating disorder, which mainly affects the central part of the pons. It has been reported to occur in a variety of clinical settings, but most commonly in association with the rapid correction of hyponatraemia and other abrupt changes in osmotic conditions. 1 Treatment of the hyperosmolar hyperglycaemic state (HSS) can cause major shifts in plasma osmolality; this leads to CPM after the concentration of plasma sodium rises quickly owing to the fall in plasma glucose after fluid supplementation and insulin therapy. 2,3
In this paper, we report a case of patient with epilepsia partialis continua and hyperglycaemic hyperosmolar state, who developed CPM before his hyperglycaemic hyperosmolality was corrected. To our knowledge, this clinical scenario has not been reported to date. The disability that resulted from CPM improved dramatically within a short period, and the patient made a complete recovery.
Case history
A 55-y-old man was admitted to our Department of Neurology with recurrent focal seizures and weakness in his right limbs. He had a three-month history of polydipsia, and had felt so thirsty over the preceding month that he had often eaten sugarcane if water was not available. Twenty days earlier, he was presented to his local hospital with a focal seizure. This ictal event consisted of clonic jerking of the right hand with progressive involvement of the upper limb and then the lower limb, which lasted for between one and three minutes; he experienced similar seizures between three and five times a day since then. At the local hospital, he received 0.4 g carbamazepine twice a day after presentation after cranial CT scans showed no abnormalities. Several days later, the seizures occurred more frequently than before, and his right limbs became weak. On the day of admission to our unit, the focal seizures started to occur continuously and he had disturbances in his consciousness with a Glasgow Coma Score (GCS) of 9/15. There was no previous history of diabetes mellitus (DM) or head trauma. Upon examination, his temperature was 38.5°C and his blood pressure was normal.
The neurological examination on admission showed impairment of consciousness with a GCS of 9/15. The focal seizures at this point was characterized by head and eye tonic turning to the right side associated with abduction convulsions of the right limb. His pupils were 3 mm in diameter bilaterally, and their light reflexes were normal. He demonstrated a right-sided hemiplegia; the biceps, triceps and patellar tendon reflexes were all grade 1/4 bilaterally, and grade 0/4 bilaterally at the ankle. The plantar responses were bilaterally flexor.
A magnetic resonance imaging (MRI) scan of the brain showed a hyperintense lesion in the central pontine region on T2-weighted images that were consistent with CPM (Figure 1). The laboratory results were as follows: glucose, 38.65 mmol/L (normal: 3.9–6.0 mmol/L); HbA1c, 17.5% (normal: 4.3–6.3%); serum sodium, 134 mmol/L (normal: 135–145 mmol/L); serum potassium, 4.33 mmol/L (normal: 3.5–5.5 mmol/L); and serum osmolarity, 318 mosm/L (normal: 285–296 mosm/L). Urinalysis revealed glucosuria (3+) and ketonuria (−). Blood gas parameters were normal (pH 7.42; pCO2 43 mmHg), consistent with a hyperosmolar hyperglycaemic state. Tests for human immunodeficiency virus (HIV), antibody (enzyme-linked immunosorbent assay) and a Treponema pallidum particle agglutination assay were negative.
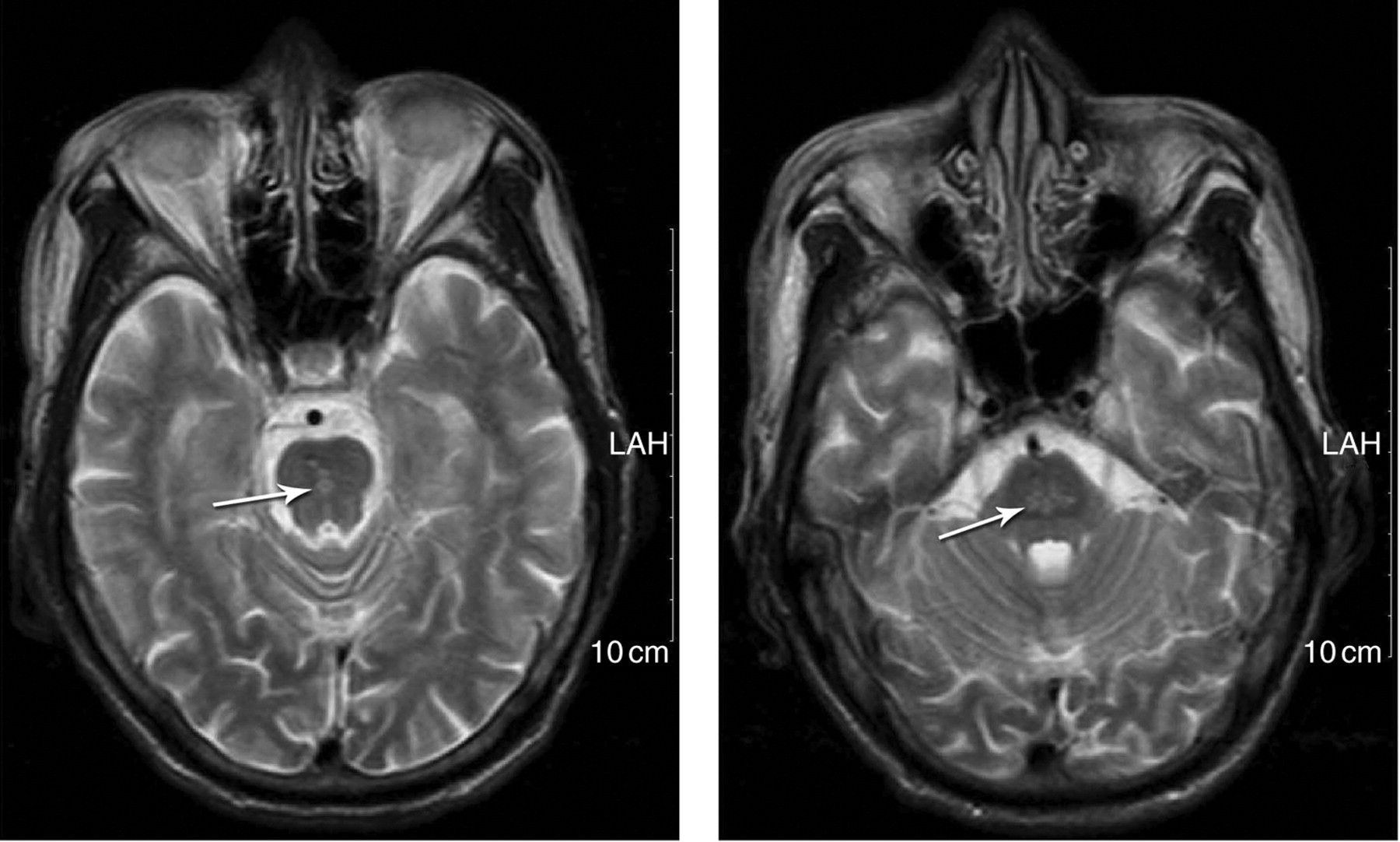
Magnetic resonance imaging scan of the brain on the day of admission (before treatment). The arrowhead shows a hyperintense lesion in the central pontine region on T2-weighted images
The patient was administered antiepileptic medication with midazolam. Simultaneous continuous intravenous infusions of normal saline and insulin were initiated over a five-hour period. During this period, there was a marked drop in his serum glucose by 6.2 mmol/L with a corresponding drop of his serum potassium from 4.33 to 2.92 mmol/L. Serum osmolality also dropped from 318 to 299.5 mosm/L, but his serum sodium remained normal throughout. The intravenous infusion of insulin was stopped and intermittent subcutaneous insulin was initiated. Approximately eight hours after admission, the focal seizure ceased, and the dose of midazolam was gradually reduced and stopped. On the second day after admission, seriological neurological examinations demonstrated that the patient regained consciousness, and his strength was determined to be 0/5 in his right upper limb, 3/5 in his right lower limb and 5/5 in his left limbs; his sensations to touch, temperature, pinprink and vibration were normal. Babinski signs were negative bilaterally, and the cranial nerve examinations were all normal.
Ten days after admission, a repeat MRI scan of the brain showed that the pontine lesion had not changed in size, but the signal of lesion was obscure. There was no enhancement of the pontine region after contrast agent administration on T1-weighted imaging; magnetic resonance angiography of the head and neck was normal. Eleven days after admission, the right-sided muscle strength began to improve, and neurological examination demonstrated a power of 2/5 in his right upper limb and 4/5 in his right lower limb. Twelve days after admission, his muscle strength was 3/5 in his right upper limb and 4/5 in his right lower limb. Five days later, the muscle strengh in all muscle groups of his right limbs were 5/5.
He was discharged following additional treatment and advice for managing his DM with subcutaneous insulin injections. He remained free of seizures during the six-month follow-up period without antiepileptic drugs, and his serum glucose concentration was stabilized and normalized. A repeat MRI of the brain at six months after hospital discharge showed disappearance of the pontine lesion on T2-weighted imaging (Figure 2).
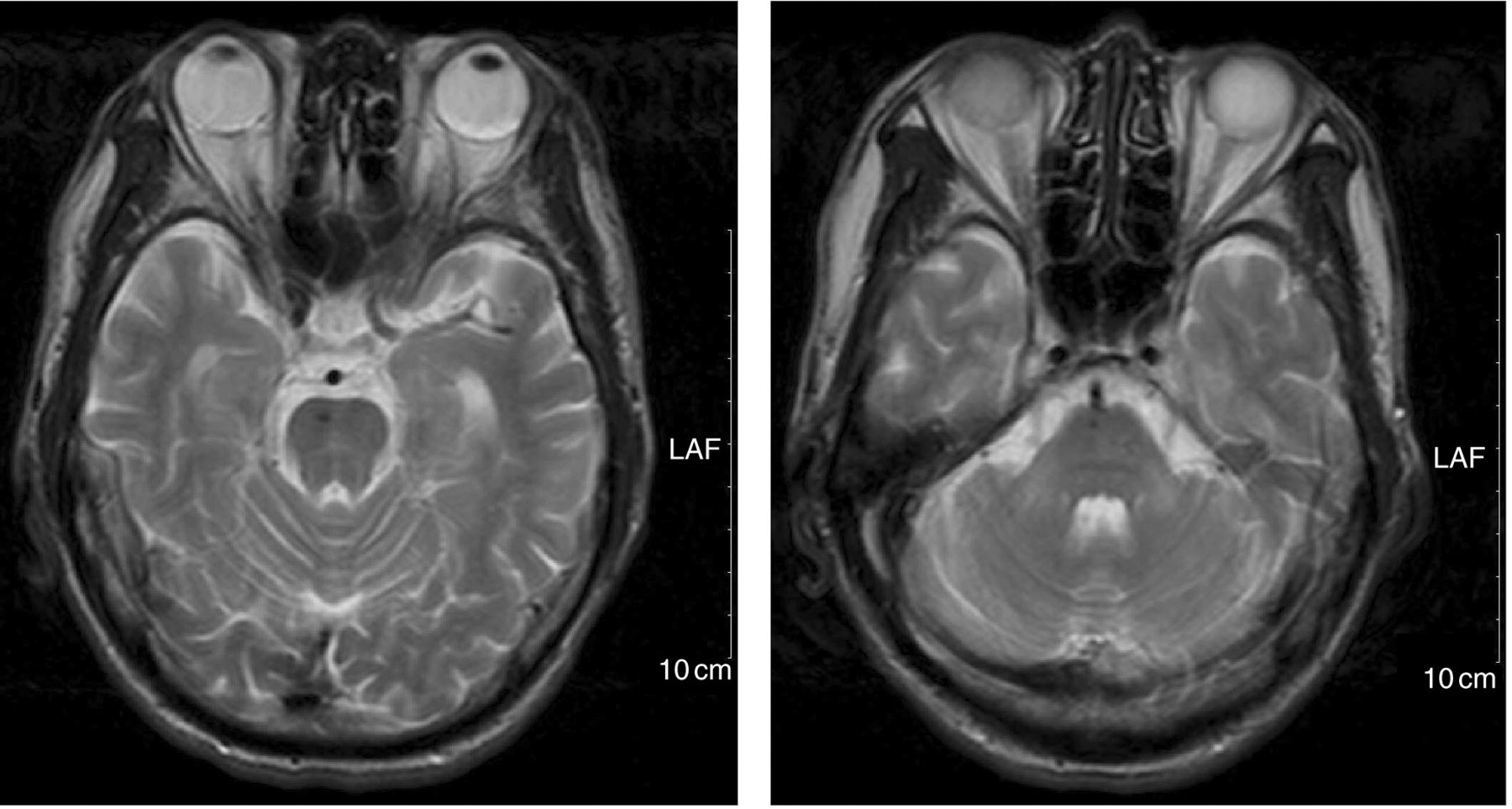
A repeat magnetic resonance imaging of the brain at six months after hospital discharge. The pontine lesion on T2-weighted imaging shows almost disappearance
Discussion
This case report describes one patient with new-onset partial epilepsy and a hyperglycaemic hyperosmolar state who developed acute right-sided hemiplegia. MRI confirmed a central lesion of the pons, which was consistent with CPM.
To date, studies on the aetiology of CPM have focused on its association with the overly rapid correction of hyponatraemia, 4 which mostly occurs in patients who are alcoholics, malnourished, have used diuretics for prolonged periods, have undergone liver transplantation 5 or who have other causes of rapid changes in their physiological osmotic parameters. 6 A further three cases of CPM that developed in association with a hyperosmolar hyperglycaemic state have been reported. 2,3,7 The onset of CPM in all of these three reports occurred after the correction of hyperglycaemic hyperosmolality and was correlated with striking increases of plasma sodium or rapid changes of serum osmolarity during this treatment period. There are obvious differences between the present case and these reports: CPM occurred in our patient before the correction of the hyperglycaemic hyperosmolar state, and a disturbance in his initial electrolytes was not found. After his blood glucose and serum osmolarity had normalized, a repeat head MRI showed that the signal of the pontine lesion got obscure, and pontine lesion had not changed in size, although the patient developed low serum potassium and decreased serum hyperosmolarity during the correction of his hyperglycaemia.
Pathologically, CPM is characterized by a symmetrical, non-inflammatory demyelinating lesion. Our case was hyperglycaemic and had an elevated serum osmolality; hyperglycaemia can cause disruption of cerebral autoregulation, endothelial cells and the blood–brain barrier, resulting in plasma leakage and vasogenic oedema. 8,9 Oedema may lead to compression of fibre tracts, which in turn causes demyelination; 10 and endothelial injury leads to the release of myelinotoxic factors from the damaged cells leading to demyelination. The mechanism of how this leads to selective myelinolysis in CPM is unknown. The central pontine area contains an admixture of white and grey fibres that are organized in a tight grid-type arrangement, which makes it particularly susceptible to osmotic demyelination. 3 The basal ganglia, thalamus, geniculate bodies and cortex–white matter junctions also have extensive appositions of grey and white matter and extra-pontine myelinolysis may occur in these areas. 11
The clinical manifestations of CPM are principally a variable, pseudobulbar paralysis because of the involvement of the corticobulbar tracts, which leads to dysphagia, dysarthria, weakness of the tongue and emotional lability. However, the literature demonstrates that multiple other presenting features can occur; quadraparesis due to involvement of the corticospinal tracts, coma and confusion occur if the lesion occurs in the pontine tegmentum and locked-in syndrome may result from a large basis pontis lesion. Bilateral miosis develops if the lesion involves the descending oculosympathetic tracts.
The clinical presentation of our patient was unusual, as the only neurological abnormality was isolated right-hemiplegia, which was worse in his arm compared with his leg. We found only a single previously published case of CPM that presented with an isolated hemiplegia. 12 In our case, partial epileptic seizures developed that increased in frequency before hemiplegia developed in his right limbs; therefore, the hemiplegia should be differentiated from Todd's paralysis. However, Todd's paralysis is transient, and typically lasts only for a period of between 30 min and several days. In our patient, muscle strength began to improve 10 days after epileptic seizures ceased and the serum glucose concentration was normalized. Therefore, we consider that the hemiplegia in our patient resulted from CPM.
Surprisingly, in our case epilepsia partialis continua was the earliest manifestation of hyperglycaemia and led to the diagnosis of DM. Hyperglycaemia may precipitate epilepsia partialis continua by lowering concentrations of gamma aminobutyric acid, which results in a low seizure threshold. 13 Focal seizures in hyperglycaemia are refractory to antiepileptic drugs and respond best to insulin and fluid replacement; 14 in our patient, the frequency of seizures gradually reduced and ultimately stopped after the correction of hyperglycaemia, and no seizures occurred during the six-month follow-up period without the use of any antiepileptic drugs.
The present case has three additional instructive features. Firstly, when a patient presents with partial epilepsy, it is essential to determine the plasma glucose concentrations immediately. Knowledge of this condition enables the seizures to be controlled rapidly and appropriately, and speeds up the diagnosis of DM. Secondly, a long-term hyperglycaemic hyperosmolar state may lead to CPM, which can have severe long-term unfortunate consequences for the patient. Thirdly, the clinical manifestation of CPM can present with only isolated hemiplegia. Of note, hemiplegia in CPM that results from HSS can make a dramatic complete recovery within a short period of time.
DECLARATIONS