
Abstract
Background
The measurement of human chorionic gonadotropin (hCG) in cerebrospinal fluid (CSF) is useful for the differential diagnosis of suprasellar lesions. However, the concentrations that prove diagnostic for neurohypophyseal germinoma have not been well defined. In addition, the immunoassays used for such measurements are the same as those applied in serum, and few studies have been performed regarding the validation of such techniques in CSF. The present study aims to apply the Elecsys® hCG + β immunoassay from Roche Diagnostics to measure hCG in CSF, as a useful tool in the diagnosis of neurohypophyseal germinomas in children and young adults.
Methods
Validation of the immunoassay involved calculation of the functional sensitivity and reference values for hCG in CSF in 35 controls in the absence of pregnancy, trophoblastic disease or tumour pathology. For the clinical application study, three patients diagnosed with neurohypophyseal germinoma have been reviewed.
Results
The functional sensitivity obtained was 0.4 IU/L. The reference values for hCG in CSF ranged from undetectable values to 0.7 IU/L. The hCG concentrations in CSF in the three studied patients, with confirmed diagnosis of neurohypophyseal germinoma, were 21.1, 32.6 and 23 IU/L, respectively.
Conclusions
The Elecsys® hCG + β immunoassay from Roche Diagnostics can be used to detect hCG in CSF with high precision. According to our results, CSF-hCG concentrations that exceed the established reference interval (undetectable values to 0.7 IU/L) in the presence of suprasellar lesions and hypophyseal stalk thickening must be considered pathological, establishing the need to exclude the presence of germinoma.
Introduction
Suprasellar germinal cell tumours form part of the differential diagnosis of suprasellar lesions in children and young adults. 1,2 Since these tumours often affect the neurohypophysis (neurohypophyseal germinomas), they can be confused with tuberoinfundibular hypophysitis, and other suprasellar lesions, thus adversely affecting or delaying correct treatment. 3–10 The determination of serum human chorionic gonadotropin (hCG) may be of help in the differential diagnosis of these lesions when the tumour contains syncytiotrophoblastic cells able to secrete the hormone, although occasionally, the serum concentrations may be very low and hard to interpret. 11–13 It has been considered that the presence of hCG in cerebrospinal fluid (CSF) represents a strong indicator of the presence of a cerebral germinoma, 14–17 but the diagnostic threshold concentrations for neurohypophyseal germinoma are not definitively established, although some authors have suggested diagnostic concentrations above 50 IU/L. 18,19 HCG is present in different molecular forms in biological fluids and in germinal cell tumours, a hCG variant may be the principal circulating hCG form. It is, therefore, important to select a hCG immunoassay method, which is able to measure the clinically relevant hCG variants for diagnosis and monitoring of germinal cell tumours. 20–22 In addition, to our knowledge, the existing immunoassays of the hormone have been validated mainly for application in serum, and few studies have been performed regarding the validation of such techniques in CSF. 14 Because matrix effects can influence test results when alternative sample types are used, CSF should be validated for the assay before clinical use. 14 So, we validated the Elecsys® hCG + β immunoassay from Roche Diagnostics to measure hCG in CSF and calculated reference values for hCG in CSF. Moreover, to demonstrate its clinical applicability, we presented three young patients with neurohypophyseal germinomas in whose the determination of a detectable CSF-hCG was determinant for a correct diagnosis.
Design and subjects
Validation of Elecsys® hCG + β immunoassay from Roche Diagnostics in CSF
The Elecsys® hCG + β immunoassay from Roche Diagnostics (Modular E-170; Mannheim, Germany) is a sandwich-type electrochemiluminescence technique, which was evaluated for use on the fully automated random-access immunoanalyser Elecsys 2010. The assay is calibrated against the Fourth International Standard for hCG from the National Institute for Biological Standards and Control, code 75/589. 20 The measuring range is 0.1–10,000 IU/L. According to the package insert, normal values for serum hCG are less than 2 IU/L for men and to 1 IU/L for premenopausal women. It has been validated in serum and plasma by the manufacturer, with an analytical sensitivity of 0.1 IU/L and a functional sensitivity of 0.6 IU/L. The within- and between-series coefficients of variation established in our laboratory are 2.92% and 3.77%, respectively. The technique uses two monoclonal antibodies, a biotinylated antibody and a ruthenium chelate-labelled antibody, that are directed to different epitopes of hCG molecule. The specific monoclonal antibodies used by the Elecsys assay measure intact hCG, free β-hCG, nicked forms, hCG missing the carboxyterminal peptide of the β-subunit and β-core hCG. 20 So, the antibodies are directed to an epitope present on intact hCG and the free β fraction, and therefore can detect the two separate entities, thus making it adequate for measuring hCG + β in clinical practice. 22,23
Analytical validation of the mentioned method for application in CSF has been developed in two stages. First, calculation was made of the functional sensitivity for CSF, defined as the smallest analyte concentration with a between-series coefficient of variation of 20%. 24 To this effect we processed a CSF pooled sample with low but detectable hCG values and performed four serial dilutions with a pooled CSF from controls whose concentrations were undetectable, which were aliquoted and processed during 10 days in order to establish the lowest reportable limit for the test. The results were interpolated on a plot of the between-series coefficient of variation versus the mean concentration of hCG in CSF for each dilution made. The calculation was performed by the equation obtained by regression potential. In turn, we determined the reference values for hCG in CSF.
Controls
Thirty-five samples were studied from the emergency laboratory corresponding to subjects in the absence of pregnancy, trophoblastic disease or tumour pathology (16♀, 19♂), with ages between 2 and 81 y. The reasons for lumbar punction in these patients were fever of unknown origin, cognitive deterioration or cephalea. All subjects gave informed consent to their CSF being used in this study. CSF samples with normal values for glucose and proteins were used in the absence of cellular elements or xanthochromia. These samples were frozen at −20°C and thawed and processed together as a single analytical batch once all samples had been collected at the end of the study.
Patients
The study involved three patients (1♀, 2♂) between 11 and 23 y of age, diagnosed in our centre with neurohypophyseal germinoma on the basis of the histopathological findings or complete response to treatment with chemotherapy and radiotherapy.
Results
Validation of the Elecsys® hCG + β immunoassay from Roche Diagnostics in CSF
The Elecsys® hCG + β immunoassay from Roche Diagnostics yielded a functional sensitivity of 0.4 IU/L in CSF (Figure 1). Mean concentrations of controls was 0.3 IU/L. The reference values for a 95% confidence interval ranged from undetectable values to 0.7 IU/L, following a normal distribution by a Kolmogorov–Smirnov test, and showing a maximum value of 0.8 IU/L.
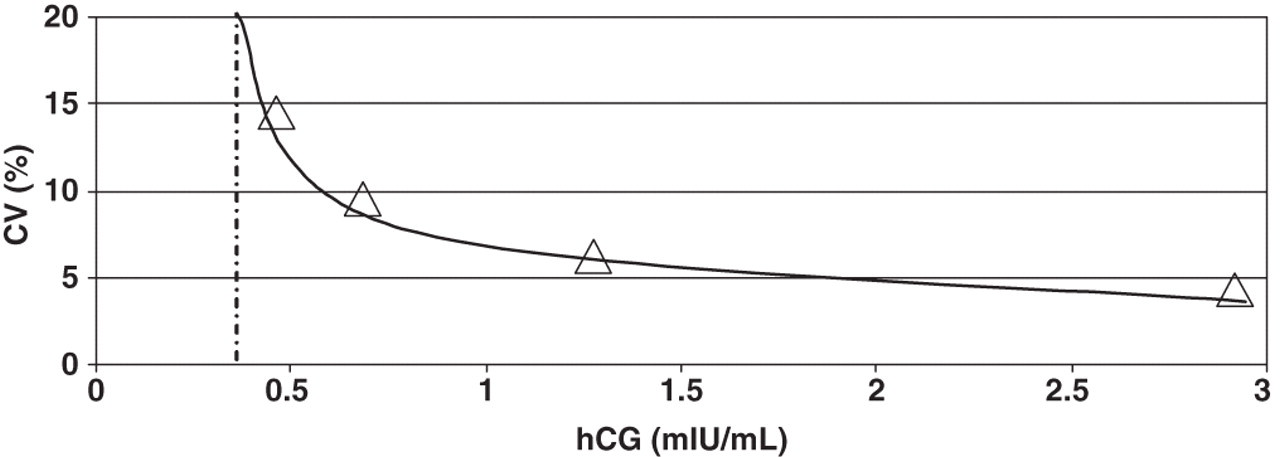
Functional sensitivity of Elecsys® hCG + β immunoassay from Roche Diagnostics in CSF. Representation of the coefficient of variation (CV) with respect to the mean concentration of hCG in CSF corresponding to four aliquots of a CSF sample diluted and processed during 10 consecutive days. CSF, cerebrospinal fluid; HCG, human chorionic gonadotropin
Description of the cases
The clinical characteristics, complementary tests and patient course are reported in Table 1.
Clinical characteristics of the patients and complementary tests 25
MRI, hypophyseal magnetic resonance imaging; PRL, prolactin; hCG, human chorionic gonadotropin; CSF, cerebrospinal fluid; TS, transsphenoidal; RT, radiotherapy; QT, chemotherapy
Discussion
Germinal cell tumours account for less than 5% of all intracranial neoplasms in children and young adults. 26 Although the most commonly affected location is the pineal gland, up to 40% of all lesions are found in the suprasellar region. Among the suprasellar germinal cell tumours, the most common lesions are germinomas. These tumours are more common in the second decade of life, without difference in gender distribution. 1
Neurohypophyseal germinomas may be pure or contain syncytiotrophoblastic giant cells. The latter may secrete hCG, reaching serum concentrations of between 0.1 and 2000 IU/L. 12,13 When the serum hCG concentrations are low, evaluation of the hormone in CSF may be of help in establishing the diagnosis, since this parameter is more sensitive as an indicator of tumour presence. 14–17 Although the definitive diagnosis is determined by the histopathological findings, a biopsy in some cases is not possible, due to inaccessibility of the tumour (as in our first patient), or may prove erroneous (as in our third patient). The differential diagnosis in children with non-specific MRI evidence of an isolated lesion with stalk thickening fundamentally must be distinguished from tuberoinfundibular lymphocytic hypophysitis. Both disorders, i.e. tuberoinfundibular lymphocytic hypophysitis and occult germinoma, cannot be easily distinguished by histology, as occurred in our third patient, and there exists a clinical need for a test, such as measurement of hCG in CSF, that can do it. 3–10
It has been considered that an hCG concentration in CSF of >50 IU/L represents a strong indicator of the presence of a germinoma. 18,19 Although this is the threshold recommended by the SIOP CNS GCT 96 protocol, there are few comparable studies in the literature and hardly any that suggest CSF reference intervals. In our patients, CSF concentrations that are much lower but still greater than expected under normal conditions are diagnostic of cerebral germinoma. For this purpose validated immunoassays are needed for measurement of the hormone in CSF, offering sufficient sensitivity to define the threshold above which the hCG concentration may be regarded as anomalous. The use of the functional sensitivity limit as the lowest detection limit is a conservative approach to ensure that any hCG result reported is not merely assay ‘noise’. 16 Further, the 20% between-run coefficient of variation approximates the maximum imprecision required for diagnostic testing. 16 Since the functional sensitivity calculated in our study (0.4 IU/L) lies within the established reference interval from undetectable values to 0.7 IU/L, the studied immunoanalytical technique is able to precisely quantify hCG within that interval. Shi et al. 27 determinated medical reference values for different tumour markers in CSF in 110 patients excluding primary tumours and meningeal carcinomatosis using the Roche E170 modular immunoassay analyzer, and their medical reference values for hCG were <0.769 IU/L, coinciding with our results. Moreover, Ferguson et al. validated the Advia Centaur® method for measurement of hCG in CSF. They created a CSF pool by combining CSF leftover samples from 50 patients and the limit of detection was evaluated by measuring hCG in the CSF pool 15 times. The minimum detection limit was determined to be 4.7 IU/L, with a coefficient of variation of 9.7%. They concluded that any detectable hCG in CSF is abnormal. 14 However, this assumption is hypothetical as the authors do not test any patients to confirm its recommendation. Moreover, the Centaur assay does appear to preferentially recognize free β hCG and not detect β-core hCG, making this particular immunoassay less than optimal for use in measuring hCG as a tumour marker. 14,20,28 In relation to laboratory provision, the National Academy of Clinical Biochemistry and the European Group on tumours markers guidelines emphasize that both intact hCG and its free β-subunit should be recognized by hCG assays used in oncology and that good baseline stability is essential for hCG because treatment may be instituted on the basis of relatively small increases in marker concentrations. 23
In our case, we reported three patients with germinoma properly established, so the diagnostic sensitivity of a concentration of hCG in CSF above the upper limit established in our laboratory is 100%. Obviously, three patients are too few to determine the accuracy of a determinated analytical method, but these patients are extremely infrequent. Unfortunately, we have not measured the concentration of hCG in CSF in patients with other suprasellar lesions, so we cannot establish the specificity of the determination of hCG in CSF in the diagnosis of neurohypophyseal germinoma. Even so, the demonstration that CSF-hCG concentrations much lower than previously established are pathological, suggest the need to include the determination of hCG in CSF in all suprasellar lesion and the establishment of validated reference values for each method and laboratory.
Katagami et al. 18 also considered that a CSF/serum hCG ratio of ≥2 represents a strong indicator of the presence of a germinoma. Our patients had CSF/serum hCG ratios of 2.6, 3 and 3.2, respectively, and this abnormal ratio helped confirm the presence of a CNS tumour. The mechanism of hCG crossing the blood–brain barrier is not known, but may be diffusion across the capillary endothelium. An increased CSF-hCG implies a primary CNS source of the hCG or CNS involvement by a peripheral hCG-producing tumour. The magnitude of the serum/CSF ratio has been suggested previously to detect the presence of cerebral metastases in patients with peripheral hCG-producing tumours. 29 In the presence of brain metastases, the CSF concentration of hCG is disproportionately increased and the ratio serum/CSF is reportedly usually less than 40. In the case of brain metastases from peripheral hCG-producing tumours, therefore, one has to consider serum/CSF ratios rather than CSF concentration alone to distinguish an intracranial source of the tumour. 30
The determination of hCG (intact hormone, free β-fraction or both) in serum or CSF is a sensitive indicator not only in the diagnosis of neurohypophyseal germinomas but also in monitoring treatment response and recurrence. 17,19,31 The level of hCG in the CSF of patients with malignant germ cell tumours is higher than that in serum and can be used as a sensitive marker in the follow-up of these tumours. Hence, the CSF levels should be monitored in marker-producing germ cell tumours before and after each treatment course if the serum concentration is not elevated. 17
In conclusion, the hCG + β immunoassay from Roche Diagnostics is sufficiently sensitive in determining hCG in CSF. In children and young adults with suprasellar lesions and hypophyseal stalk thickening, the hCG concentrations in CSF and serum must be measured in order to help exclude the possibility of germinoma. CSF concentrations of hCG that exceed the established reference interval, the presence of suprasellar lesions and hypophyseal stalk thickening must be considered pathological and highly suspicious of germinoma.
DECLARATIONS