
Abstract
We present a rare case of an insulin-like growth factor-2 (IGF-2)-secreting tumour of the thorax. This patient demonstrated the combination of fasting hypoglycaemia and impaired glucose tolerance on oral glucose tolerance testing, which has not been previously described in this condition. A review of the literature of IGF-2-secreting intrathoracic tumours is presented here.
Introduction
Hypoglycaemia associated with non-islet cell tumours is a rare clinical occurrence, which can be due to secretion of insulin-like growth factor type 2 (IGF-2). We report a case of a patient with an incidental finding of an IGF-2-secreting pleural tumour causing hypoglycaemia, who also demonstrated impaired glucose tolerance (IGT) on an oral glucose tolerance test (OGTT).
Case report
A 59-year-old Caucasian woman was referred by her primary care physician for investigation of weight loss and lethargy. She had lost approximately 19% of her baseline weight over 12 months and had noticed a swelling in her neck, which had gradually increased in size over the same time period. She had no significant past medical history. Clinical examination revealed a large goitre. The patient was euthyroid (free T4 17.0 pmol/L [10.3–24.5], thyroid-stimulating hormone [TSH] 0.9 mU/L [0.40–4.00]). The patient underwent computed tomography (CT) scanning of the neck and thorax, which revealed a surprising finding of a large mass occupying most of the right hemithorax and confirmed as encapsulated on magnetic resonance imaging (Figure 1). A CT-guided biopsy was performed and histology confirmed that the mass was a well-differentiated spindle cell neoplasm. While fasting overnight for her investigations, the patient was observed to become confused and disoriented and experienced urinary incontinence. On further questioning, she admitted two episodes of disorientation and lethargy prior to admission to hospital. The patient's family members witnessed three episodes of complete disorientation and confusion, associated with urinary incontinence. All had occurred in the early morning and gradually resolved after eating. There was no loss of consciousness. The patient, however, had minimal recollection of these episodes afterwards.
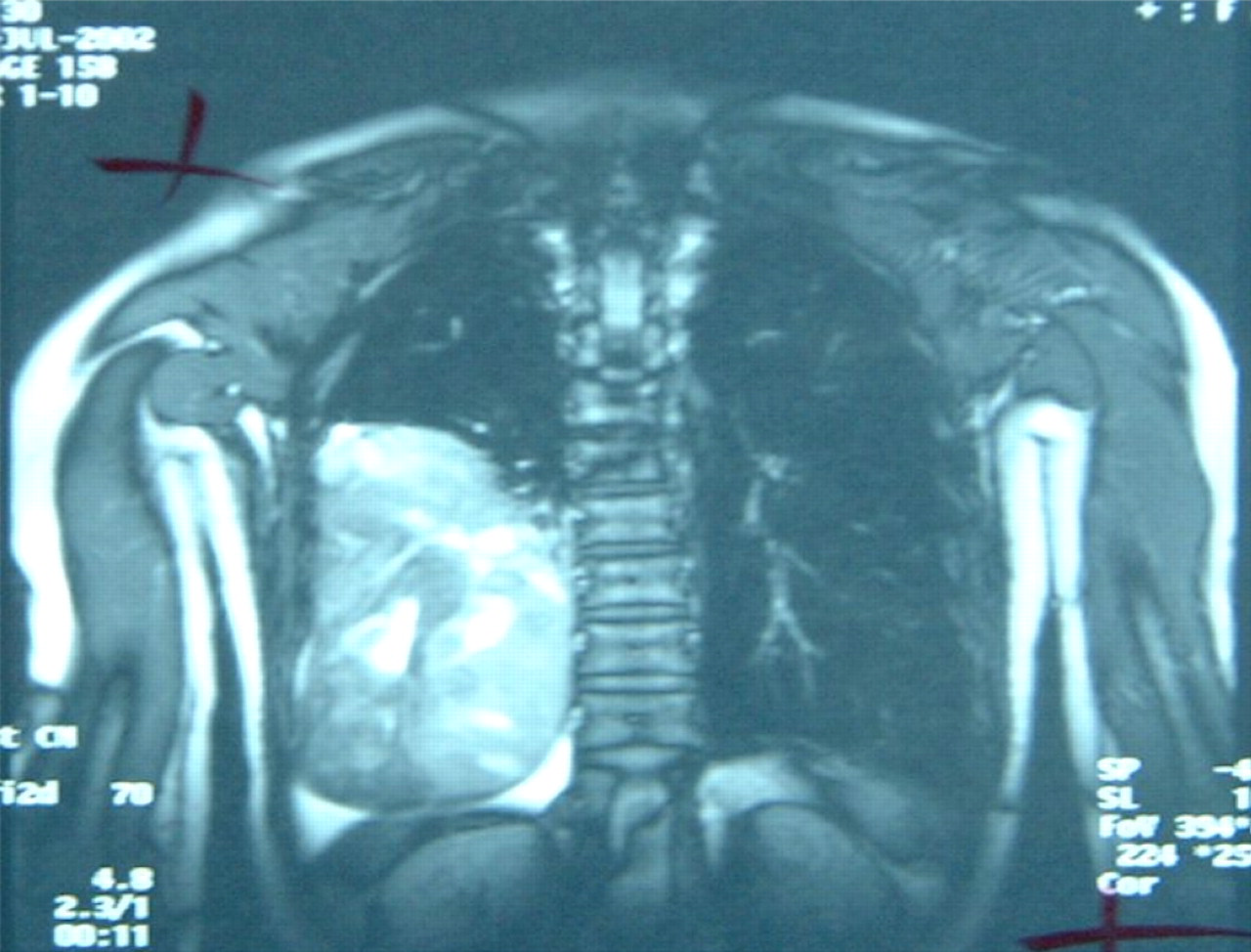
Thoracic magnetic resonance imaging showing a large circumscribed mass in the right hemi-thorax
A differential diagnosis included a seizure disorder but her CT scan brain and electroencephalogram were normal. While fasting for investigation, an early morning episode of confusion was witnessed by the nursing staff. Serial capillary blood glucose measurements performed while fasting overnight revealed early morning readings of 2.0 mmol/L associated with disorientation. On treating the hypoglycaemia with 100 mL of sugar-containing soft drink, the patient's symptoms resolved, but her capillary blood glucose concentrations became elevated (up to 17 mmol/L). During her inpatient stay, a number of elevated postprandial capillary glucose readings were also noted after meals, even in the absence of any treatment for hypoglycaemia.
Following an overnight fast and during a hypoglycaemic episode, blood samples were drawn for the measurement of plasma glucose, serum insulin, C-peptide, cortisol, growth hormone (GH), IGF-1 and IGF-2. The patient's hypoglycaemic episodes were associated with appropriate suppression of insulin and C-peptide. GH concentrations were undetectable while her serum cortisol concentrations peaked at 415 nmol/L (Table 1). IGF-1 concentrations were low, however, with a raised IGF-2 to IGF-1 ratio of more than 30 (reference range of less than 10). An OGTT was also performed due to the elevated postprandial capillary glucose readings and this demonstrated fasting hypoglycaemia at baseline, but the two-hour glucose concentration was 9.8 mmol/L, which was consistent with IGT (see Table 2).
Preoperative fasting tests
IGF-1, insulin-like growth factor 1
Preoperative and postoperative oral glucose tolerance tests
A provisional diagnosis of an IGF-2 secreting neoplasm was made. The patient was referred for a right posterolateral thoracotomy and excision of the right thoracic mass. A tumour weighing 1361 g was resected. Histopathology showed cellular areas consisting of packed spindle cells with very little intervening stroma. There were focal areas of extensive fibrosis and necrosis. Immunocytochemical staining was positive for CD34 and vimentin.
Following resection of the tumour, the patient's blood glucose normalized and her episodes of disorientation resolved. An OGTT repeated postoperatively was normal (see Table 2). The patient has since remained well with no further occurrence of her tumour or her hypoglycaemia.
Discussion
We present a rare case of an IGF-2-secreting tumour of the thorax. This case is remarkable in that the large chest tumour was discovered incidentally, in that she was experiencing significant hypoglycaemic symptoms due to the IGF-2 secretion, which she failed to report initially and in that in addition to having biochemically proven hypoglycaemia, the patient exhibited IGT on OGTT.
The first report of a patient with an intrathoracic tumour and hypoglycaemic symptoms was described by Potter in 1930. 1 Fewer than 20 cases have been described to date in the literature. The pathophysiological mechanism is thought to be that hypoglycaemia is caused by the secretion of IGF-2 by the tumour. Recent evidence suggests that ‘big’ IGF-2, which is the main form of IGF-2 secreted by certain tumours, may play an important role. Both IGF-1 and IGF-2 have approximately 50% amino acid homology to insulin and both, like insulin, have A and B chains connected by disulphide bonds. These structural similarities explain why both IGFs are able to bind to and activate the insulin receptors. The higher molecular weight form of IGF-2 or ‘big’ IGF-2, however, has been shown to be secreted by certain tumours and can cause non-islet cell tumour hypoglycaemia. 2 These variants are capable of binding to IGF and insulin receptors with greater bioavailability as they demonstrate decreased binding to serum-binding proteins. Zapf et al. 3 proposed that secretion of ‘big’ IGF-2 results in suppression of GH, insulin, IGF-1 and certain IGF-binding proteins, resulting in increased bioavailability of free IGF-2 to target tissues.
A unique aspect of this case was the unexpected combination of fasting hypoglycaemia and IGT. Preoperatively, the patient's plasma glucose rose to 9.8 mmol/L at 120 min during the OGTT, satisfying the World Health Organization criteria for a diagnosis of IGT (see Figure 2a). The OGTT was performed because the patient had been noted to be quite hyperglycaemic based on capillary blood glucose readings in response to standard treatment of her symptomatic hypoglycaemia. The patient was also noted to be hyperglycaemic postprandially while in hospital. Postoperatively, her fasting and two-hour plasma glucose concentrations normalized. Although abnormal glucose tolerance in patients with spontaneous hypoglycaemia has been very rarely reported in the past, these were described in subjects with insulinomas. 4,5 To our knowledge, this combination in IGF-2-secreting tumours has not previously been documented. The likely explanation for this curious association is that insulin secretion in response to glucose was impaired or delayed by high circulating IGF-2 concentrations resulting in slower than normal clearance of the glucose load from the blood. This could be due to a direct inhibitory effect of IGF-2 on the beta cells as the IGF-2 receptor has been shown to be present in insulin-secreting cells. 6 Alternatively, it could be a result of an indirect effect of chronic suppression of insulin concentrations in response to hypoglycaemia. Down-regulation of insulin receptors in target tissues could also contribute to these hyperglycaemic events. It is striking that the insulin concentrations achieved during the postoperative OGTT were higher than during the preoperative test, particularly at the 30-min time point (see Figure 2b). This suggests that, in particular, the first phase of insulin release was diminished, reminiscent of the defects seen early in the development of diabetes.
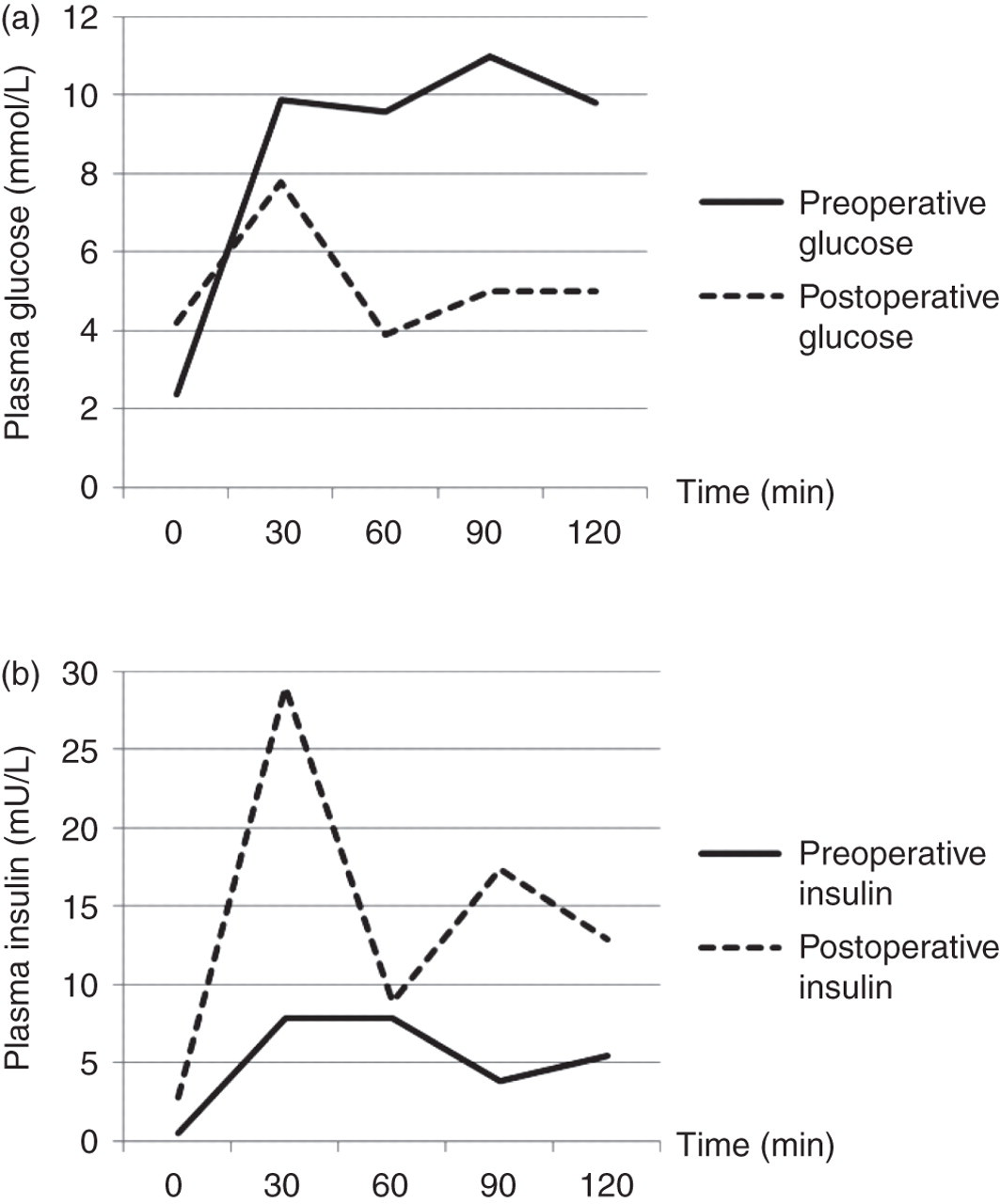
(a) Comparison of preoperative and postoperative plasma glucose during the oral glucose tolerance test. (b) Comparison of preoperative and postoperative insulin during the oral glucose tolerance test
Another unusual feature of this case was that the chest tumour was incidentally found during investigation of a goitre. It is also interesting to note that the early morning symptoms of confusion and disorientation were not reported spontaneously. It is highly likely that the patient's hypoglycaemic episodes were secondary to IGF-2 production by the spindle cell tumour, as the patient was shown to have hypoinsulinaemic hypoglycaemia, suppressed pituitary GH and IGF-1 concentrations with an elevated IGF-2:IGF-1 ratio preoperatively. A review of the literature revealed that in most cases these tumours are solitary fibrous pleural tumours or spindle cell neoplasms. 7 These tumours are usually benign, and histologically stain positive for CD34 and vimentin. Surgical resection of the tumour is curative, as in this case, with total resolution of the patient's hypoglycaemic episodes, strongly suggesting that the hypoglycaemia was due to a factor released by the tumour.
In summary, we present a case of a very rare syndrome of hypoglycaemia due to production of IGF-2 by a spindle cell tumour of the chest. The case is remarkable because in addition to experiencing fasting hypoglycaemia, the patient had hyperglycaemia, and IGT was documented on OGTT preoperatively with reversion to normal glucose tolerance following removal of the tumour. Unusually, the tumour was discovered during work-up for goitre. The biochemical disturbances of plasma glucose that appear polar opposites, fasting hypoglycaemia and IGT are probably both due either directly or indirectly to the excess by IGF-2.
DECLARATIONS