
Abstract
Background
Difficulties associated with measuring ionized calcium in clinical practice have led to the use of total calcium, with or without adjustment for albumin concentration, as an estimate of calcium metabolism. We examined the correlation between ionized and total/adjusted calcium over a 24-h period in patients with adult growth hormone deficiency (AGHD), a group of patients with previously reported alterations in calcium metabolism.
Methods
Four patients with AGHD were consented to the study. They were hospitalized for 24 h where half-hourly blood samples were collected for ionized calcium, total calcium, albumin and creatinine, before and one month after the commencement of growth hormone replacement. Total calcium concentration was adjusted for serum albumin.
Results
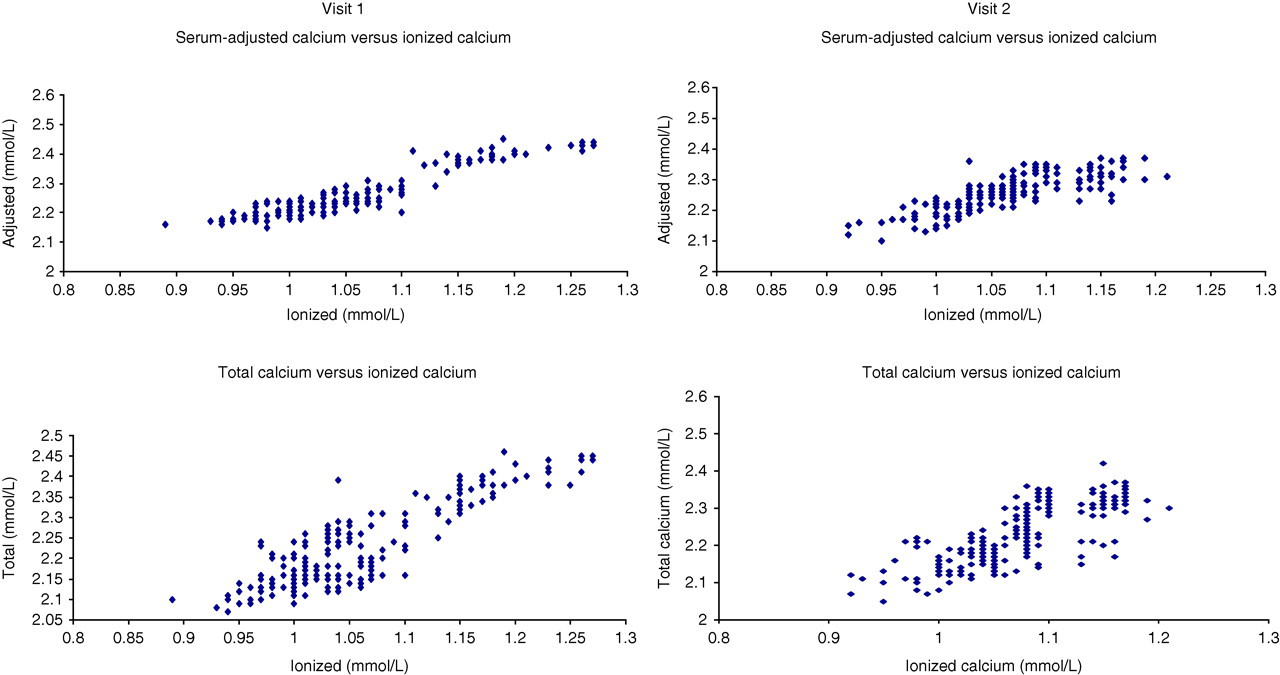
Strong correlations were found between ionized calcium and adjusted calcium (r 2 = 0.840 and 0.766 for visits 1 and 2, respectively, P < 0.001), and between ionized calcium and total calcium (r 2 = 0.828 and 0.731 for visits 1 and 2, respectively, P < 0.001). Correlations remained significant during the day (ionized versus adjusted calcium: r 2 = 0.847 and 0.780 for visits 1 and 2, respectively; ionized versus total calcium: r 2 = 0.860 and 0.792 for visits 1 and 2, respectively, all P < 0.001) and at night (ionized versus adjusted calcium: r 2 = 0.831 and 0.802 for visits 1 and 2, respectively; ionized versus total calcium: r 2 = 0.767 and 0.722 for visits 1 and 2, respectively, all P < 0.001).
Conclusion
The results of our study suggest that total calcium and serum-adjusted calcium can be used in place of ionized calcium as a reliable indicator of calcium metabolism over a 24-h period in patients with AGHD.
Introduction
Ionized calcium is the biologically active form of calcium in the blood. 1 Although research into the ionized fraction of calcium started over 70 y ago, 1 controversy regarding the method of determination and interpretation of ionized calcium results still exists. Different manufacturers of ionized calcium analysers present variable reference ranges and concern has existed regarding the stability of the electrodes used for measuring ionized calcium. 2 As such, total calcium rather than ionized calcium is traditionally measured in routine practice when assessing calcium status of healthy individuals and patients with disorders of calcium regulation. A large proportion of calcium in the blood is bound to protein and therefore adjustment of measured total calcium concentration for variations in protein content may lead to greater accuracy of results. 3 The formulae most commonly used adjust for differences in albumin concentration (serum-adjusted calcium) to avoid false low estimations of calcium concentration in hypoalbuminaemic patients. 4
There have been a number of reports that have studied the relationship between ionized and total or adjusted calcium. 3,5–8 The conclusions of these studies have been conflicting with some revealing good correlation 3,7–8 between ionized and total/adjusted calcium but others showing poor correlation, 5,6 particularly where abnormal calcium metabolism is present, bringing into question the validity of using total/adjusted calcium for the estimation of calcium activity in some patients with chronic disease. The general consensus, however, is that ionized calcium correlates well with measurements of total and adjusted calcium in healthy individuals who have calcium and albumin concentrations within the reference range. 3,7,8
Adult growth hormone deficiency (AGHD) is a condition that has gained recognition since the 1980s. 9 It occurs as a consequence of pituitary or peripituitary disease that diminishes growth hormone (GH) production from the anterior pituitary gland. AGHD is associated with a reduction in the sensitivity of the bone and kidneys to parathormone (PTH), which may result in an increased prevalence of osteoporosis in AGHD 10 as a consequence of reduced PTH target organ sensitivity. Patients with AGHD have a relatively higher PTH concentration and lower serum-adjusted calcium and nephrogenous cyclic AMP concentration (NcAMP, marker of PTH activity at the kidney) than healthy individuals. Conventional treatment of AGHD with recombinant human GH replacement results in an increase in PTH sensitivity within one month of initiation, 11 as evidenced by a reduction in PTH concentration and increase in NcAMP and serum-adjusted calcium. 12 All studies published to date investigating calcium metabolism in AGHD have measured adjusted calcium rather than ionized calcium and there is no published data looking at the relationship between ionized and adjusted calcium in these patients.
The aim of this study was to determine the effect of AGHD on serum ionized calcium concentration before and after GH replacement, throughout a 24-h period, and to investigate whether ionized calcium was correlated to adjusted calcium for the duration of the circadian cycle in this group of patients, thus determining whether adjusted calcium can be used as a reliable indicator of calcium metabolism in patients with AGHD
Patients and methods
Four patients with severe AGHD were recruited to the study. The details of the patients recruited are shown in Table 1. Severe AGHD was defined as a peak GH response of less than 9 mU/L (3 μg/L) to hypoglycaemia (blood glucose <2.2 mmol/L) induced during an insulin stress test. All other pituitary hormones were optimally replaced in all patients, as per standard practice and in accordance with guidelines published by the National Institute for Clinical Excellence. 13 The study was approved by the Royal Liverpool University Hospital Ethics Committee and written informed consent was obtained from each patient.
Patient details
All patients were admitted to the Metabolic Bone Unit of the Royal Liverpool University Hospital at 13:00 h for a period of 25 h. An indwelling venous cannula was inserted in the antecubital fossa of each patient at the time of admission, and blood samples were collected every half hour from 14:00 on the day of admission to 14:00 the following day. Unheparinized blood samples collected for measurement of ionized calcium were analysed immediately. Heparinized blood samples collected for total calcium, albumin and creatinine were centrifuged immediately at 4°C, and serum was separated to be frozen at −70°C for later analysis. Each patient was served with standardized hospital meals at 08:00, 12:00, 18:00 and 22:00. Subjects remained recumbent during 23:00–08:00.
After the initial visit, all patients were initiated on standard GH replacement of 0.2 mg 13 self-injected at 22:00 each night. The study visit was repeated one month following GH replacement.
Biochemistry
Serum calcium, albumin and creatinine were measured on all samples by the standard autoanalyser method (P module, Roche Diagnostics, Lewes, UK). Serum calcium was adjusted for albumin using the formula: serum-adjusted calcium = 0.0103 × (40.4 − serum albumin) + total calcium. Ionized calcium was measured using a Bayer 855 analyser (Bayer Corps, Bucks, UK). The coefficients of variation for ionized calcium were 3.6% at 1.54 mmol/L, 2.3% at 1.17 mmol/L and 2.0% at 0.76 mmol/L.
Statistical analysis
Pearson's correlation (SPSS version 11) was used to determine correlation coefficients between ionized and adjusted calcium concentrations and between ionized and total calcium concentrations in all samples from all patients before (n = 196) and after (n = 196) treatment with GH replacement. Student's t-test for paired data, with Bonferroni's correction to allow for multiple comparisons, was used to analyse the difference in ionized calcium, adjusted calcium and total calcium between the two study visits.
Individual and population-mean cosinor analysis, to determine circadian rhythm parameters of ionized calcium, serum-adjusted calcium and total calcium, were performed using Chronolab 3.0 (Universidade de Vigo, Vigo, Spain), a validated software package for analysing biological time series by least-squares estimation. 14
For all analyses, P < 0.05 was considered significant. Values are expressed as the mean ± standard error of mean, unless otherwise stated.
Sampling a smaller cohort of patients for a 24-h period, rather than a larger number at a single time point allows not only examination of the diurnal rhythm, but also derivation of a 24-h mean for all measurements, thereby eliminating potential errors occurring as a result of single time point sampling of hormones that are secreted in a circadian rhythm. 10 The study size was determined by a power calculation that was based on previous studies performed at our centre. 11,12,15–17 Using the nomogram presented by Altman, 18 the power derived with a minimum of four patients, at a significance concentration of 0.05, was greater than 95%.
Results
There was good correlation both before and after GH replacement between ionized calcium and serum-adjusted calcium (r 2 = 0.840 and 0.766 for visits 1 and 2, respectively, P < 0.001), and between ionized calcium and total calcium (r 2 = 0.828 and 0.731 for visits 1 and 2, respectively, P < 0.001). The correlations between ionized calcium and serum-adjusted calcium/total calcium for individual patients at both study visits are shown in Table 2. Figure 1 shows the scattergrams of the relationship between ionized calcium and serum-adjusted calcium and between ionized calcium and total calcium at each time point throughout the 24-h sampling period for each study visit.
Correlation between mean serum-adjusted calcium/ionized calcium and mean total calcium/ionized calcium
Correlation coefficients between ionized calcium and serum-adjusted calcium/total calcium
Significant correlations between ionized calcium and serum-adjusted calcium remained both at night (22:00–08:00, r 2 = 0.831 and 0.802 for visits 1 and 2, respectively) and during the day (r 2 = 0.847 and 0.780 for visits 1 and 2, respectively). Similarly, correlation between ionized and total calcium was present at both visits during the night (r 2 = 0.767 and 0.722 for visits 1 and 2, respectively) and day (r 2 = 0.860 and 0.792 for visits 1 and 2, respectively).
Cosinor analysis did not reveal significant ionized calcium, serum-adjusted calcium, total calcium or albumin circadian rhythms for any individual patient or across the group. Consistent with studies previously performed at our centre, 24-h mean serum-adjusted calcium concentration increased significantly between visits one and two, following the initiation of GH replacement (2.249 ± 0.006 versus 2.275 ± 0.006 mmol/L, P < 0.001). In keeping with the increase in 24-h mean serum-adjusted calcium, 24-h mean ionized calcium and 24-h mean total calcium also increased significantly between the visits (1.076 ± 0.005 versus 1.113 ± 0.005 mmol/L for ionized calcium, 2.223 ± 0.007 versus 2.246 ± 0.007 mmol/L for total calcium, both P < 0.001). Twenty-four-hour mean PTH decreased significantly between visits one and two (4.34 ± 0.08 versus 4.21 ± 0.07 pmol/L, P < 0.001).
Figure 2 shows the mean ionized calcium, serum-adjusted calcium and total calcium throughout the 24-h sampling period. Between 02:00 and 08:00, there was a significant decrease in mean ionized calcium (1.082 ± 0.005 versus 1.051 ± 0.005 mmol/L, P < 0.001), serum-adjusted calcium (2.256 ± 0.006 versus 2.244 ± 0.006 mmol/L, P < 0.001) and total calcium (2.250 ± 0.006 versus 2.201 ± 0.009 mmol/L, P < 0.001), compared with mean daytime (08:00–22:00) concentrations at visit one. The percentage reduction in mean night-time ionized calcium (2.78 ± 0.54%) and total calcium (2.16 ± 0.49%) concentrations was significantly greater than that seen in the serum-adjusted calcium concentration (0.53 ± 0.46%) (P < 0.001). A significant decrease in the mean night-time (02:00–08:00) concentration of ionized, adjusted and total calcium compared with daytime concentrations persisted at visit two. A significant decrease in mean serum albumin concentration was also seen at night (02:00–08:00) compared with daytime concentrations at both visits (P < 0.001).
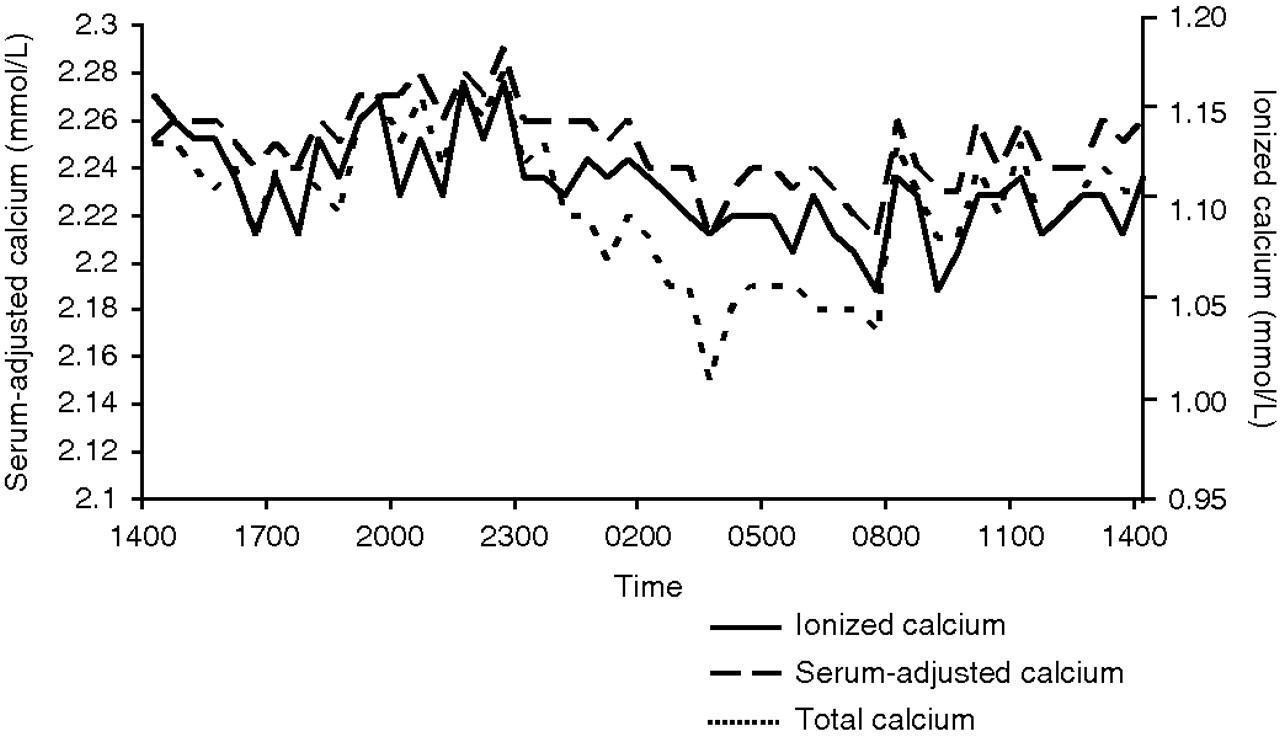
Mean ionized calcium, serum-adjusted calcium and total calcium concentrations during study visit 1
All patients were vitamin D replete with both 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D within the appropriate reference intervals in all patients. Serum albumin and creatinine were within the appropriate reference intervals for all patients at all points during the study. Mean albumin was 38.6 ± 1.22 g/L at visit one and 38.3 ± 1.17 g/L at visit 2. Mean serum creatinine was 72.0 ± 22.3 μmol/L at visit one and 79.1 ± 21.9 μmol/L at visit two. There was no significant difference in mean albumin or creatinine between visits one and two.
Discussion
Our study has shown that ionized calcium measured using the Bayer 855 analyser correlates well with both serum-adjusted calcium and total calcium measured by standard laboratory autoanalysers, in patients with AGHD. Correlation coefficients were marginally higher for serum-adjusted calcium than total calcium. Previous reports studying correlation between ionized calcium and other measures of calcium have been conflicting. 3,5–8 Two previous studies that did not show good correlation between ionized and corrected calcium were performed more than three decades ago, 5,6 at which time it was recognized that electrodes used to measure ionized calcium were less stable than those available currently. 3,8 Therefore, weak correlations between ionized and either total or corrected calcium concentrations observed in previous studies may have been, in part, due to errors in ionized calcium measurement occurring as a consequence of electrode instability. Studies designed to compare the different technologies used to measure ionized calcium have shown that the measured activity of ionized calcium may vary significantly when analysing solutions of differing sodium chloride concentration and protein content, with increased ionic strength and the presence of protein resulting in an increase in the measured activity of ionized calcium. 19 The size of this effect appears to be dependent on the type of technology used with porous frit-restricted junctions showing less variability with changes in protein concentration than selective membrane or open junctions but more variability to changes in ionic strength.
Many previous reports have studied correlations between ionized and adjusted calcium in patients with chronic kidney disease or in critically ill patients in the intensive care setting. 7,20–22 Abnormalities in acid–base balance are common in such patients and it is well recognized that the presence of acidosis has a significant effect on ionized calcium concentrations, causing a significant increase, which may account for the poorer correlations between ionized and adjusted calcium observed in these studies. 23 Disturbance of acid–base homeostasis is not a recognized feature of AGHD and may partly explain why good correlations between ionized and adjusted/total calcium were seen in our study but not in some previous reports. Consistent with our findings, other studies have reported good correlations between ionized and adjusted calcium, where serum albumin has been within the reference range and a large proportion of the study population did not have conditions that were associated with disturbance in acid–base balance. 3,7,8
Patients with AGHD are known to have a lower bone mineral density, with increased risk of osteoporotic fractures, compared with age- and gender-matched healthy controls. 24 Bone turnover is reduced in AGHD and this is thought to occur as a consequence of a reduction in the sensitivity of the kidney and bone to the effect of PTH. 10 GH replacement in AGHD is associated with an increase in target-organ PTH sensitivity, with resultant increased serum calcium and NcAMP and simultaneous reduction in PTH concentration. 12,16,17 The increase in 24-h mean calcium observed after one month of GH replacement in our study is in keeping with previous findings. 12,16,17
GH replacement in AGHD is also associated with changes in the PTH circadian rhythm. 10 In particular, a greater increase in the nocturnal PTH peak and a less sustained afternoon rise in PTH have been reported following GH replacement. In our study, ionized, adjusted or total calcium did not exhibit a circadian rhythm. In keeping with this finding, significant adjusted calcium circadian rhythms have not been identified in any study of AGHD patients to date. 10,11,15–17 Importantly, strong correlations between ionized and adjusted/total calcium were maintained throughout the day and night, validating the use of serum-adjusted calcium as a measurement of calcium metabolism in patients with AGHD, whatever the time of venesection.
A nocturnal reduction in calcium has been described in healthy individuals, 25 but has not previously been reported in patients with AGHD. Several mechanisms may have a role in the reduction of calcium at night. Haemodilution occurring as a consequence of a higher blood volume at night 26 is thought to be important, but the predominant factor is likely to be the reduction in serum albumin that also occurs at night. 25 A proportion of total blood calcium is bound to protein and therefore it can be expected that total calcium concentration decreases at night. The measured activity of ionized calcium has been shown to increase in the presence of protein 19 and therefore again it can be expected that ionized calcium would decrease during the night. The greater effect of albumin concentration on ionized and total calcium may explain the greater reduction in nocturnal ionized and total calcium compared with adjusted calcium observed in our study.
Measuring total calcium with adjustment for albumin has a practical advantage over measuring ionized calcium. Ionized calcium requires immediate analysis and therefore requires the presence of staff trained to venesect the patient and use the analyser. In practice, this is not usually the same person. In addition an ionized calcium analyser must be available for near-patient testing at the time of venesection, which poses logistical problems for many centres and laboratories. Measuring total calcium and albumin allows the transport of samples to the laboratory with appropriate storage for later analysis at a convenient time. The results of our study have shown good correlation between ionized calcium and adjusted calcium and thus support the use of adjusted calcium as an accurate measurement of calcium metabolism in patients with AGHD. The results of the study should be replicable on analysers that use cresophthalein complexone and bromcresol green methods for measurement of calcium and albumin, respectively.
DECLARATIONS