
Abstract
Cryoglobulins are serum immunoglobulins that precipitate at temperatures below 37°C and re-dissolve on warming. Cryoglobulinaemia leads to variable symptoms including characteristic purpura, ischaemia of extremities, renal failure, peripheral neuropathy, abdominal pain secondary to intestinal ischaemia and arthralgias. Cryoglobulin testing is underutilized in clinical practice. It has been neglected in clinical laboratories and by clinicians due to several factors, such as the length of time it takes for serum cryoglobulin analysis to be performed in the laboratory, the perceived difficulty in getting optimal sampling conditions and a failure to appreciate that even apparently low levels of cryoglobulin can be associated with severe symptoms in some patients. The most important variable confounding standardization of cryoglobulin testing is improper sample handling. A recent report critically appraising the current practice of cryoglobulin evaluation in 137 laboratories in Europe by United Kingdom National External Quality Assurance Scheme (UKNEQAS) illustrated the wide variability in practice. Although many clinical laboratories perform cryoglobulin evaluation, there are widespread differences in the methodology used and the care with which this is carried out and this leads to considerable intralaboratory and interlaboratory variability. The most common sources of error are false-negative results due to loss of cryoprecipitate during transport and storage. Better standardization is needed to avoid missed diagnoses and improve the comparability of results. Laboratories should ensure that sample temperature is maintained at 37°C until the serum is separated. In this article, we briefly review the classification and clinical features of cryoglobulins and suggest best practice guidelines for laboratory detection and identification of cryoglobulins.
Introduction
Cryoglobulins are immunoglobulins that precipitate or gel out of serum at low temperatures and re-solubilize on warming. Other cold precipitable proteins include cryofibrinogens, fibronectin and C-reactive protein–albumin complexes. In 1974, Brouet et al. 1 proposed a classification based on the type of immunoglobulin in the cryoprecipitate (Table 1).
Characteristics and clinical associations of cryoglobulins
MGUS, monoclonal gammopathy of uncertain significance; LPD, lymphoproliferative disease; HCV, hepatitis C virus; HBV, hepatitis B virus; HIV, human immunodeficiency virus; EBV, Epstein-Barr virus; CMV, cytomegalovirus; SLE, systemic lupus erythematosus; RA, rheumatoid arthritis; IBD, inflammatory bowel disease; SBE, subacute bacterial endocarditis; TB, tuberculosis; FLC, free light chains
Type I cryoglobulins (10–15% of cases) consist of monoclonal immunoglobulin (Ig), most frequently IgM, occasionally IgG and rarely IgA. Type I cryoglobulins are mostly found in patients with lymphoproliferative diseases.
Type II cryoglobulins (50–60% of cases) are a mixture of immunoglobulins of different isotypes, including at least one monoclonal directed at the Fc portion of normal IgG (rheumatoid factor [RF]), which is usually IgM kappa (occasionally IgG and IgA). Type II cryoglobulins are associated with chronic hepatitis C virus (HCV) infection and Sjögren's syndrome. 2–4
Type III cryoglobulins (25–30% of cases) are mixtures of polyclonal immunoglobulins of different isotypes usually polyclonal or oligoclonal IgM and IgG with IgM polyclonal RF activity, which reacts with the IgG. Type III can be seen in viral (HCV, hepatitis B virus, human immunodeficiency virus, Epstein-Barr virus, cytomegalovirus), bacterial or parasitic infections, as well as some autoimmune and lymphoproliferative disorders.
Brouet 1 and colleagues realized that a large proportion (30%) of patients with cryoglobulinaemia had no known disease. This was called ‘essential’ cryoglobulinaemia. In the 1990s, it became clear that most of these essential cryoglobulinaemias were associated with HCV infection. 5
In addition to immunoglobulins (with or without RF activity) cryoprecipitates may contain albumin, fibronectin, C1q, viruses and bacteria. 6
Some authors 7,8 have recommended classifying cryoglobulins into ‘simple monoclonal cryoglobulins’ (Type I) and ‘mixed cryoglobulins’ (Type II and Type III).
Why are cryoglobulins cold insoluble?
The biochemical basis of cold insolubility remains incompletely understood. The solubility of proteins depends upon concentration, hydrophobicity, size and surface charge, as well as the solution temperature, pH and ionic strength. Relative abundance of hydrophobic amino acids, decreased tyrosine and sialic acid residues has been implicated. 9 Abnormal immunoglobulins with reduced concentrations of sialic acid and galactose in the Fc region of Immunoglobulin may lead to decreased solubility in cold. In mixed cryoglobulinaemia IgM–RF–IgG complexes may be an important factor in cryoprecipitation. 10
The formation of cryoaggregates upon exposure to cold may be the triggering factor for vasculitis. However, this does not explain why tissues that are distant from the site of exposure to cold (e.g. kidney, nerves) may be affected. Alterations of chloride 11 and calcium 12 concentration in the renal interstitium may influence cryoglobulin structure and aggregation.
Which cryoglobulins are found in a UK reference centre?
As the method of cryoglobulin detection becomes more sensitive, the percentages of positive samples of types II and III tend to increase with a decrease in type I cryoglobulins. This is also a reflection of the population screened. The Protein Reference Unit, Sheffield receives samples from secondary and tertiary services in rheumatology, infectious diseases, hepatology, neurology and haematology. During the past four years, 887 samples were analysed for cryoglobulinaemia. Of these, 193 had cryoproteins of which five were cryofibrinogens (Table 2). Forty-three percent had a serum cryoglobulin concentration of <1 g/L (Table 3). There were three bi-clonal cryoglobulins, one of which later evolved into a standard Type II. Most monoclonal components were IgM kappa. There were only 1×IgM lambda, 2×IgG kappa, 1×IgA kappa and 1×IgA lambda monoclones. The variation in the reported prevalence and types of cryoglobulins reflects the differences in patient population, analytical sensitivity and analytical techniques. 13
Sheffield Protein Reference Unit 2004–2008: 188 cryoglobulins: types and prevalence
Sheffield Protein Reference Unit 2004–2008: 188 cryoglobulins: relative concentrations of different types
Clinical syndrome for cryoglobulinaemia
It is important to distinguish the clinical features of cryoglobulinaemia from that of underlying disease. In general, common symptoms of cryoglobulinaemia are due to cutaneous ischaemia and include purpura, livedo reticularis, Raynaud's syndrome, ecchymosis, ulcerations, ischaemic necrosis and, rarely gangrene. Other manifestations of cryoglobulinaemia include membrano-proliferative glomerulonephritis and peripheral neuropathy with dysaesthesia. The mixed cryoglobulinaemia syndrome is characterized by a typical clinical triad of purpura, weakness and arthralgias. 14
In general, Type I rarely causes vasculitis and tends to be associated with signs of peripheral vessel occlusion. Isolated mixed cryoglobulins may represent the only feature in asymptomatic patients probably as an expression of early-stage disease. On the other hand, patients may present with a characteristic cryoglobulinaemic syndrome. It is widely held that cryoglobulins that precipitate at higher temperatures (i.e. at temperatures found in live human beings rather than only at refrigerator temperatures) are more likely to cause peripheral ischaemic features, but this is not easily tested in vitro, although some clinicians question the physiological relevance of a cryoglobulin that can only be precipitated after seven days at 4 degrees. Nevertheless, it is general practice to take clinical note of all large cryoglobulins detected by such methods where the clinical features are consistent with cryoglobulin deposition.
A negative cryoglobulin assay should not exclude the diagnosis if the clinical suspicion remains high. Poor collection technique leads to false-negative results. C4 concentrations can be a surrogate marker of cryoglobulin immune complex activity but can be normal in the presence of clinically relevant cryoglobulinaemia. We recommend that multiple attempts should be made where clinical suspicion remains high in the absence of a positive test and it is our practice to repeat at least three times. Episodic failure to detect cryoglobulins is well recognized in cryoglobulinaemic renal disease and may reflect poor standardization of technique as much as fluctuation in cryoglobulin levels.
Purpura is the most common (55–100%) clinical sign of cryoglobulinaemia. 15 It can be variable and intermittent. Palpable lesions may appear on the lower limbs, buttocks and trunk, often preceded by paresthesia or local pricking sensations rather than frank pain. Exposure to cold is reported to precipitate lesions in only 10–30% of cases. 15
Raynaud's phenomenon is reported in about one-third of patients 15 and affects hands, feet, lips, ear lobes and nose. When severe this may lead to necrosis and digital gangrene, hence the need to keep peripheries warm.
Mixed cryoglobulinaemia causes small vessel vasculitis similar to cutaneous leucocytoclastic vasculitis and Henoch-Schonlein purpura. 16 Cryoglobulinaemic vasculitis is caused by cryoglobulin immune complex deposits in small and medium-sized vessels of skin and glomeruli and is characterized by infiltrating monocytes and lymphocytes associated with fibrinoid necrosis, endothelial cell hyperplasia and haemorrhage.
Cryoglobulinaemic nephropathy is characterized by proteinuria, microscopic haematuria and hypertension. Up to a third of patients may present with an acute nephritic syndrome and rapid deterioration in renal function. 17,18 Membrano-proliferative glomerulonephritis is the most common histological pattern, with endocapillary proliferation with massive infiltration of monocytes/macrophages, amorphous subendothelial deposits and monocytes engulfing and degrading the deposits. Indirect immunofluorescence demonstrates immunoglobulins and C3 deposits. Electron microscopy shows characteristic deposits with in the macrophages (Figure 1).
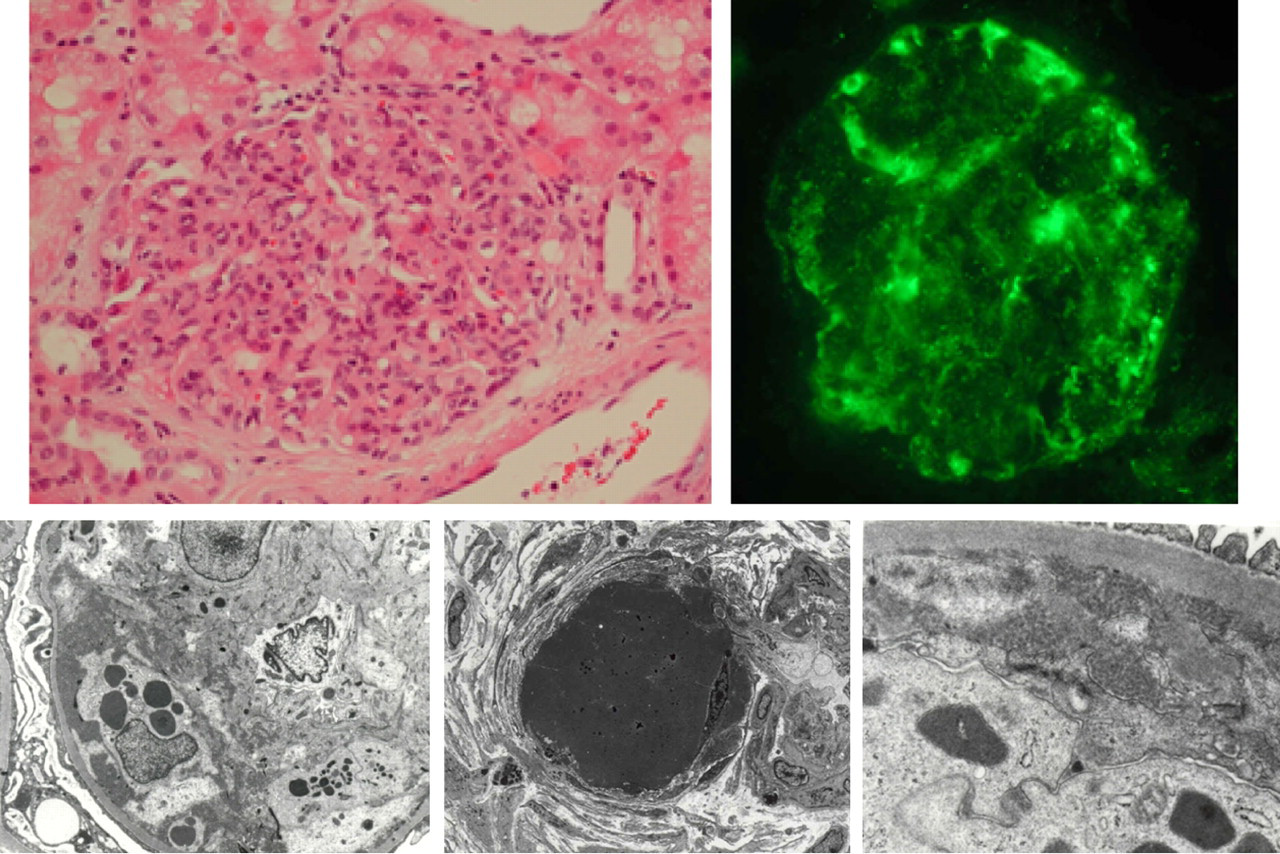
Cryoglobulinaemic nephritis. Histology – membranoproliferative glomerulonephritis with intense cellular infiltrate; direct immunofluorescence (DIF) – IgG and C3 deposition; electron microscopy (EM) – monocyte with phagocytosed cryoglobulin, hyaline thrombus and subendothelial deposits
In hepatitis-C-related nephropathy, HCV core protein and immunoglobulin are homogeneously distributed along the capillary walls of the glomeruli and are a component of the immune complexes. 19
Nephrotoxicity is probably dependent on immunoglobulin physicochemical properties, including the isoelectric point, chloride concentration in the renal interstitium and the ability to activate complement. 11,20–22
Peripheral neuropathy is a common nervous system manifestation in Type II and III cryoglobulinaemia. Neuropathy is reported in up to 86% of mixed cryoglobulinaemia series. 23,24 Mononeuritis multiplex can occur. Impairment of the vasa nervorum microcirculation by intravascular cryoglobulin deposits or vasculitis are likely mechanisms. 25
Cryoglobulinaemia can be life threatening. In a series of 209 patients, 26 29 (14%) had severe acute renal failure, intestinal vasculitis, pulmonary haemorrhage or central nervous system involvement. Two-thirds died, most from pulmonary haemorrhage and 100% of those with intestinal ischaemia died.
Cryoglobulins, HCV and Sjögrens syndrome
HCV is lymphotrophic. The E2 capsid protein binds to CD81 on hepatocytes, B and T lymphocytes. 27 HCV-infected patients with mixed cryoglobulinaemia have higher lymphocyte-associated viral load compared with patients without cryoglobulinaemia. 28
CD81 is a part of the B-cell signalling complex and HCV binding may lower the threshold required for signal transduction and lead to polyclonal activation of immunoglobulin production including IgM RF. 29,30 Enhanced and sustained B-cell signalling and activation lead to polyclonal or oligoclonal B-cell proliferation.
Cryoglobulins have been reported in 5–61% 14,31 patients with Sjögren's syndrome and majority of these have mixed cryoglobulinaemia. Fifty percent of Sjögren's syndrome patients with mixed cryoglobulinaemia had HCV infection compared with only 8% of Sjögren's syndrome patients without cryoglobulins. 32 Cryoglobulin positivity was associated with the risk of lymphoproliferative disease and vasculitis. During a 10-y follow-up, half of the patients with cryoglobulins developed lymphoma or vasculitis as opposed to only 5% of patients without cryoglobulin. 33
When should we test for cryoglobulins?
Healthy individuals may have low concentrations of cryoglobulins (<0.06 g/L). 34,35 Mixed polyclonal cryoglobulins often occur transiently during infections. Careful laboratory interpretation in the light of the clinical context by an appropriately trained individual with experience in the diagnosis of cryoglobulinaemia is essential. If a laboratory is unable to provide effective clinical interpretive support it should probably not be doing the assay.
Cryoglobulins are heterogeneous compounds varying in composition, thermal properties and ability to activate complement. Serum concentrations do not correlate with symptom severity in all cases. Mixed cryoglobulin is reported in 20–56% of HCV-infected individuals 36,37 but only 5–27% of the HCV cryoglobulins cause a cryoglobulinaemic syndrome. 13 Cryoglobulin testing should be reserved for patients with appropriate clinical symptoms or laboratory findings (Box 1).
Indications for investigation
Raynaud's syndrome Peripheral ischaemia in the absence of peripheral vascular disease Cold-induced cyanosis of ears, nose and fingers Skin purpura Cutaneous vasculitis Membrano-proliferative glomerulonephritis Sjögren's syndrome with nephritis or gammopathy Monoclonal gammopathy with hyperviscosity Monoclonal gammopathy with low C4 Monoclonal gammopathy with cold sensitivity Undiagnosed peripheral neuropathy Chronic HCV and HBV infection* Sjögren's syndrome* Laboratory abnormalities that should lead to investigation of cryoglobulins
– Gelling of blood on blood drawing – Pseudo-thromobocytosis – Pseudo-erythrocytosis – Very low C4 – Rouleax formation of red blood cells on the blood film – Changing immunoglobulin levels – Unexplained high titre rheumatoid factor – Failure of migration of proteins on electrophoresis needing reducing agent treatment
HCV, hepatitis C virus; HBV, hepatitis B virus
*Only if symptoms attributable to cryoglobulinaemia are present
Laboratory analysis
Several groups have described different analytical approaches for cryoglobulin detection. There is no internationally accepted standard. 8,13,38
United Kingdom National External Quality Assurance Scheme (UKNEQAS) surveyed current practice in the detection, analysis and reporting of cryoglobulins in Europe, with a survey of 137 laboratories 39 demonstrating that only 36% of laboratories used procedures to ensure that the temperature did not drop below 37°C until after serum separation (tube preheating, transport in container and sedimentation and/or centrifugation at 37°C). There was wide variability in the time allowed for cryoprecipitation at 4°C from 12 h to nine days, with 30% of laboratories allowing precipitation for less than three days. One in five laboratories did not re-solubilize the cryoprecipitate at 37°C and cryoprecipitate was not immunotyped by one in four laboratories with the result that the type of the cryoprecipitate remained unknown. We recommend the following minimum steps (Figure 2).
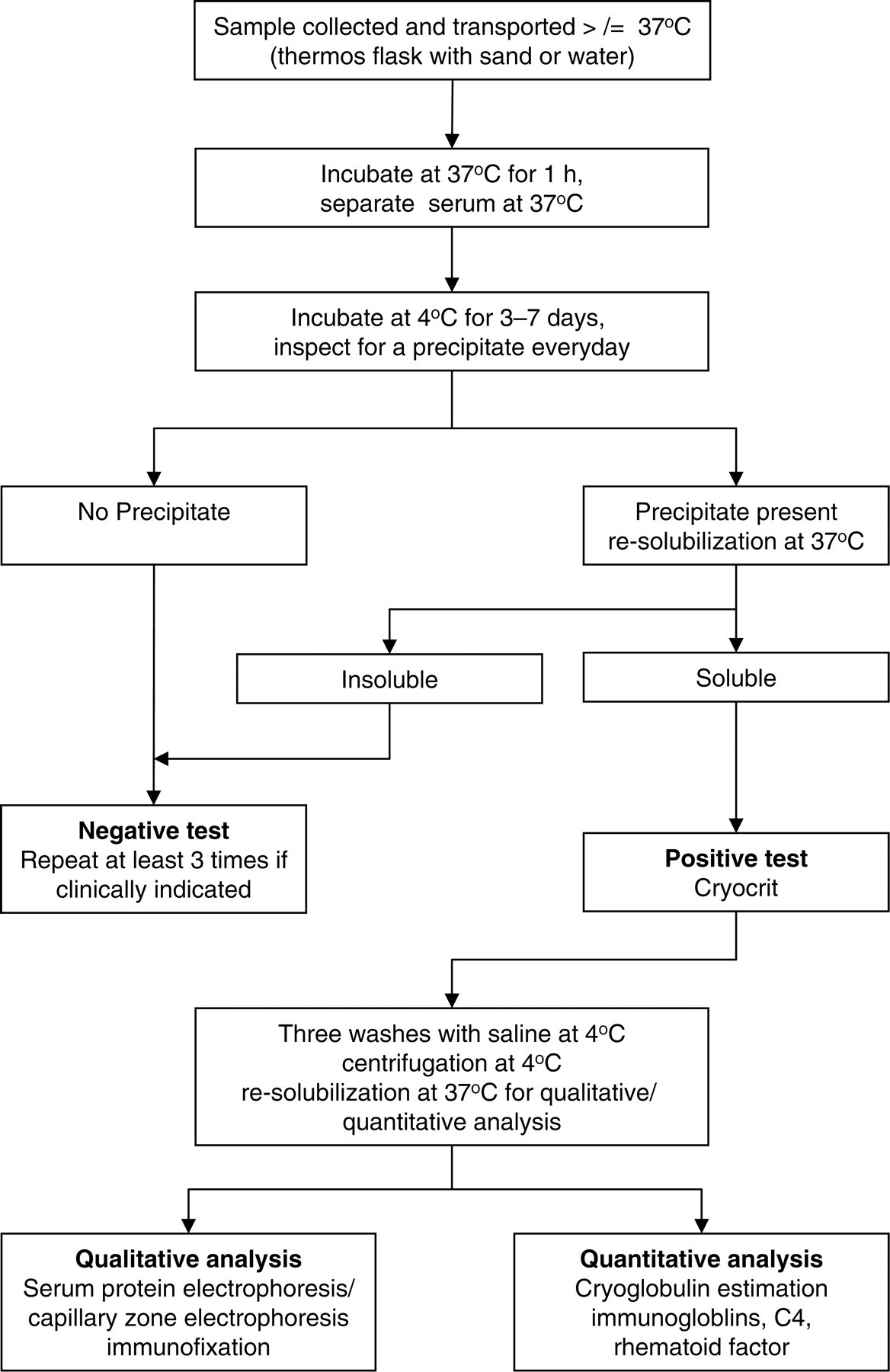
Laboratory evaluation of cryoglobulins
Sample collection and transport
Sample collection is the most critical phase in cryoglobulin analysis. The most common reason for a false-negative result is improper collection and transport of the sample. The analytical phase of cryoglobulin evaluation begins at this stage and improper collection can make subsequent results meaningless. Blood should be collected, transported, clotted at 37°C and centrifuged at 37°C to avoid false-negative results. 8 We suggest collecting 15–20 mL of blood into tubes prewarmed to 37°C. Tubes should never be carried by hand to the laboratory. Samples should be placed in a flask filled with water or sand at 38-40°C depending on the ambient temperature and the estimated delay in delivery of the specimen to the laboratory (to ensure that the temperature does not fall below 37°C at any time). Once delivered to the laboratory it should be immediately transferred to a 37°C incubator/water-bath and allowed to clot for at least one hour. Serum should be separated from the clot by centrifuging at 37°C. There is considerable variability in the techniques used by laboratories, which ranged from 1800 relative centrifugal force (rcf) for five minutes to 2500 revolutions per minute (rpm) for 10 min. 8 This is unlikely to be critical.
In the UKNEQAS survey, 39 40% of laboratories did not use preheated tubes and a further 18% samples were brought to the laboratory by hand-held transport. In circumstances where adequate temperature control cannot be ensured during sample collection and transport, cryoglobulin investigations should not be attempted (to avoid false-negative results). In many laboratories (47%), the sample was centrifuged without maintaining the temperature at 37°C probably because of a lack of a heated centrifuge. When a warm centrifuge is not available, specimens should be allowed to separate at 37°C, and serum drawn off without centrifugation. Following separation, any haemolysis or lipaemia should be noted since this may interfere with visual interpretation of cryoprecipitation.
In patients who are receiving heparin, fibronectin–heparin complexes may lead to false-positive cryoprecipitation. We recommend collecting an EDTA sample at the same time as the serum routinely to exclude cryofibrinogenaemia 40,41 as cryoglobulins and cryofibrinogens can lead to similar clinical symptoms and signs.
Two aliquots of separated serum should be incubated for at least three days, one at 4°C and the other at 37°C 42 and preferably for seven days 8 and visually inspected every day. Type I cryoglobulins tend to precipitate within hours and become apparent by the next day. Mixed cryoglobulins at low concentrations may take several days to precipitate. A cryoprecipitate may be seen as gelatinous, flocculent, crystalline material or sometimes as a dusty hue.
Rapid screening methods for cryoprecipitation such as detection of light scattering by turbidimetry or nephelometry 43,44 or increasing the rate of cryoprecipitation by adding distilled water 45 are not recommended.
Re-solubilization
Re-dissolution of the cryoglobulin precipitate by re-warming to 37°C is very important. If the precipitate is not resoluble within a few minutes then the result is negative– no further analysis is required. Initially keeping separate aliquots aids processing of samples.
Quantitation
The simplest estimate of cryoglobulin concentration is the cryocrit, measured in a calibrated sedimentation tube, 8 the volume of the cryoprecipitate is read from the tube markings. The procedure is convenient, rapid and inexpensive but reproducibility is suspect and it is at best a crude estimation and is not therefore recommended practice as the sole means of determining cryoglobulin levels.
Cryocrit estimation requires a large volume of serum. It is influenced by contaminating proteins, washing and resolubilization steps and is not standardized by volume or centrifugation conditions.
Centrifugation and washing of the cryoprecipitate must be performed at 4°C with cold saline (0.15 mmol/L) or phosphate-buffered saline (pH – 7.4; 0.138 mmol/L) to separate the cryoglobulins from other serum proteins. After each wash, the specimen is centrifuged at 7500 rcf for five minutes and supernatant removed and reconstituted with cold saline. After three successive washes, cold saline is added to the purified cryoglobulin to recover the same volume as the initial blood sample. Precipitate is re-dissolved by warming back to 37°C overnight before further analysis.
There are wide differences in the number of washes used by different laboratories as evidenced by the UK NEQAS survey. 39 Each wash is associated with a potential loss of protein resulting from dilution.
Cryoglobulin purity should be assessed by using electrophoresis optimized for urinary protein analysis at low concentrations. If the cryoglobulin is properly washed and purified, only the gammaglobulin band will be stained (and albumin will be gone).
Laboratories using capillary zone electrophoresis can compare the ratio of gammaglobulin to albumin peaks in the solubilized cryoprecipitate with a control serum sample stored at 37°C.
Further studies
Detailed characterization and typing of the cryoprecipitate should always be performed. The type of cryoglobulin will assist in determining the cause and prognosis.
Gel electrophoresis (or capillary electrophoresis) and subsequent immunofixation have become methods of choice for most laboratories. Serum immunoglobulins, serum viscosity, RF, antinuclear antibodies, investigations for HCV and other infections and complement C3 and C4 levels may be indicated depending upon the clinical features and type of cryoglobulinaemia. Some laboratories estimate complement, RF and immunoglobulins before and after cryoprecipitation, densitometry on warm electrophoresis (performed as close to 37 degrees as practicable) to quantify paraproteins, and immunofixation to type the components. There is no consensus on the best method. Some laboratories do not type the cryoglobulin; that would generally be regarded as inadequate practice.
Common problems
Samples that contain high concentrations of cryoglobulin may block analytical instruments that run at room temperature. Cryoglobulins, which precipitate during serum centrifugation or storage, may elude detection. Electrophoresis of such samples may appear normal because the monoclonal protein has been lost prior to electrophoresis. In gel electrophoresis at room temperature the cryoglobulin may precipitate at the application point and will need to be distinguished from aggregation of non-cryoglobulin IgM monoclone using mercaptoethanol or dithiothreitol. The presence of cryoglobulin can cause falsely elevated cell counts in automated cell counters. 46
Cryoglobulins may adversely affect the measurement of protein in light scattering assays. Complement may be activated ex vivo and appear falsely low, hence complement measurements should be carried out on serum kept at 37°C.
Management of cryoglobulinaemia
The treatment of cryoglobulinaemia depends on the severity of symptoms, the underlying disease and the type of cryoglobulin. Quantitation of cryoglobulins can be used to make therapeutic decisions (plasmapheresis) and to assess the efficacy of therapeutic interventions.
The cryocrit and complement levels do not correlate with disease activity and treatment should be based on the clinical features rather than the laboratory markers. No treatment is required in asymptomatic patients even in the presence of high cryocrit levels. In symptomatic diseases, therapy should be adapted to the individual patients according to the severity of clinical symptoms and to the underlying disorder.
The goal of therapy is to limit in vivo precipitation of cryoglobulins and the resultant inflammatory effects. Some patients with cryoglobulinaemia suffer from mild, recurrent episodes of lower extremity purpura that require no specific therapy or can be controlled with non-steroidal anti-inflammatory drugs or low doses of steroids.
In Type I, cryoglobulinaemia therapy directed towards underlying lymphoproliferative disease will usually be initiated in symptomatic patients.
In Type II and Type III, cryoglobulinaemia secondary to HCV infection, interferon-alpha either alone or with ribavirin is the standard treatment. 47,48 Reduction of HCV-RNA is associated with decline of cryocrit, IgM and RF activity. Cryoglobulins may, however, persist even after symptoms resolve. Purpuric lesions tend to respond rapidly while neuropathy and nephropathy are the slowest to respond. 15
In non-HCV-associated mixed cryoglobulinaemia, corticosteroids and immunosuppressive treatment are used and may be considered in symptomatic patients receiving anti-HCV treatment.
In HCV-negative patients with uncontrolled symptoms of cryoglobulinaemia despite the above therapies, cyclosporine, azathioprine and cyclophosphamide have been used alone or with steroids. 15
Plasmapheresis (in a warm room) is indicated in those rare patients with severe manifestations of cryoglobulinaemia (cryoglobulinaemic nephropathy, skin ulcers, sensory motor neuropathy and widespread vasculitis) and hyperviscosity syndrome. It removes circulating cryoglobulins and prevents their deposition in tissues. Improvement of symptoms is related to the rapid reduction of the levels of circulating complexes, antibodies and toxic substances. Plasmapheresis is not used as monotherapy, as frequently a rebound of phenomena is observed after discontinuation of the procedure and thus is combined with concomitant immunosuppressive treatment with high-dose corticosteroids and cyclophosphamide. 15
Rituximab is a chimeric monoclonal antibody consisting of human IgG1 and kappa constant regions and of mouse variable regions from a hybridoma directed against human CD20. CD20 is expressed throughout the stages of B-cell development except the earliest stages and plasma cells 49 making it an excellent target for therapy directed at B-cell malignancies. In 1997 rituximab was approved for treatment of non-Hodgkin's B-cell lymphomas. 50
Efficacy of rituximab has been reported both in Type I 51 and mixed cryoglobulinaemias. 52–56 Most of the patients showed a complete response characterized by rapid improvement of clinical signs, arthralgia, purpura, skin ulcers, peripheral neuropathy, decline of cryocrit and RF titres. It may well be increasingly used in severe symptomatic cryoglobulinaemia, avoiding hazardous immunosuppressive treatment.
Symptomatic response to treatment is the mainstay of monitoring of responses. The intrinsic variability and difficulty in controlling cryoglobulin estimation mitigate against its use in this circumstance, as does the long lead time to complete cryoglobulin investigation (up to 7 d). Rapidly changing surrogates such as C4 levels, RF may be useful is some cases.
Conclusions
A badly performed cryoglobulin assay is often a waste of time, money and effort. Many factors should be standardized as much as possible before attempting cryoglobulin analyses. There is significant variability in the composition and clinical manifestations of cryoglobulins between patients. They differ widely in their thermal thresholds and rate of precipitation. There are no obvious red flags for their pathogenicity, except perhaps for the presence of large Type I cases in concentrations of several grams per litre.
Preanalytical factors are the major cause of assay variability. Laboratories should realize that the analytical phase of this assay starts the moment the serum is collected from the patient. Unless appropriate sample collection and transportation to the analysing laboratory is ensured and controlled there is no point doing the rest of the assay. Inappropriately handled samples should not be used. This remains the greatest challenge to laboratories as collection is often not in their direct control, whereas acceptance of the sample is.
There is need for international and national consensus on the minimum standards for cryoglobulin evaluation to avoid missed diagnoses and to improve the comparability of results. We recommend the following minimum standards (Box 2). Laboratories should ensure that sample temperature does not drop below 37°C until after serum separation. The serum should be kept at 4°C for at least three (preferably 7) days. The cryoprecipitate should be washed and re-solubilized at 37°C for further analysis. Cryoglobulin evaluation should not be done if the above criteria are not satisfied.
Cryoglobulin evaluation – best practice
Fresh specimen of blood should be taken directly into a warmed container at 37°C Sample should be delivered to the laboratory =/>37°C Allowed to clot at 37°C – minimum 1 h. Serum should be separated by centrifugation at 37°C Aliquots of separated serum should be kept at 4°C and 37°C for at least three days Observation of any cryoprecipitate formation at 4°C, which should become soluble again when placed at 37°C Provide a reasonably robust quantitation estimate Should analyse the proteins to classify the type of cryoglobulin Must be prepared to repeat the sample on multiple occasions to ensure that false-negative results do not occur when clinical suspicion remains high Must be part of EQA scheme for measurement of other proteins in the protocol
Further standardization of the later analytical phases are also required. Further typing of the cryoglobulin to reliably distinguish Type I from Type II and III is required as a minimum for clinical utility. No cryoglobulin should be reported in the absence of an interpretative report in the light of the clinical details. Finally, the clinical significance of a finding of a cryoglobulin is critically dependent on the context in which it is found. If a laboratory is unable to provide appropriate interpretive support then they should not be performing the assay.
DECLARATIONS