
Abstract
Introduction
Ghrelin is a gastric peptide that has been implicated in the development of obesity and cardiovascular disease. It has been reported that ghrelin binds to lipoproteins, although the different binding patterns of acylated ghrelin (AG) and unacylated ghrelin (UAG) are still to be determined.
Methods
Lipoprotein fractions were generated using a self-generating iodixanol gradient. AG and UAG were measured using specific enzyme immunoassays.
Results
AG bound to all lipoproteins in approximately equal concentrations (VLDL 26%, LDL 22%, HDL 23%) and was present as a plasma protein (27%). UAG bound more specifically to HDL (49%) and was present as a plasma protein (48%).
Conclusions
The different binding patterns of AG and UAG may have significant implications for their biological effects, including roles in energy metabolism, the development of obesity and potentially in the modulation of cardiovascular disease.
Introduction
Obesity is increasing at epidemic proportions in the UK and is a major contributory factor to cardiovascular disease. Obesity is caused by a long-term imbalance in energy intake and expenditure, therefore a better understanding of factors affecting energy intake is crucial. Ghrelin is produced by the X/A cells of the stomach in an active, acylated form, which increases food intake and gastric motility, and stimulates growth hormone secretion. 1 Acylated ghrelin (AG) is rapidly deacylated in plasma to unacylated ghrelin (UAG), which can act antagonistically to AG to decrease food intake and gastric emptying. 2
Ghrelin also has a number of cardiovascular actions. AG can decrease blood pressure and reduce the formation of reactive oxygen species in human polymorphonuclear cells, 3 while UAG can decrease cardiomyocyte and endothelial cell apoptosis. 4 Total ghrelin (TGR) concentrations negatively correlate with subcutaneous fat volume, 5 hypertriglyceridaemia 6 and insulin resistance. 5,6
Lipoproteins have a well-established role in the development of atherosclerosis; however, despite the potential roles of both lipoproteins and gut hormones in atherosclerosis, there is little research describing their relationship. It has been reported that ghrelin binds to lipoproteins; however, the exact nature and pattern of lipoprotein binding is unclear. 7 The binding of ghrelin to lipoproteins may therefore both determine and modulate many of the cardiovascular functions of ghrelin thus described.
The aim of this study was to clarify the binding of ghrelin to lipoproteins, and investigate the possible implications.
Methods
Sample collection
Fasting blood samples were collected from eight free-living participants, with normal metabolic profiles. Samples were collected into tubes containing EDTA and aprotinin (300 KIU/mL of whole blood), centrifuged immediately (1800
Lipoprotein fractionation
Lipoprotein fractions were generated using a self-generating gradient of iodixanol.
8
Iodixanol (60% [w/v]) was added to plasma to produce 12% iodixanol–plasma. This was carefully layered underneath an equal volume of 6% iodixanol in phosphate-buffered saline (PBS), in a 13 × 35 mm polyallomer centrifuge tube (Optiseal™ tubes, Beckman Coulter, Fullerton, USA), and the tube filled with PBS. The tubes were centrifuged (401,000
Measurement of ghrelin lipoprotein fractions
Cholesterol, triglyceride and total protein were measured in each fraction (Roche Modular System, Mannheim, Germany), to identify the lipoprotein containing fractions.
AG and UAG were measured by ELISA (Sociétè de Pharmcologie et d'Immunologie -BIO, France), with coefficients of variation of 0.60% at 2500 pg/mL and 2.73% at 19.6 pg/mL for UAG, and 1.0% at 1250 pg/mL and 10.3% at 9.80 pg/mL for AG.
Results
The study participant demographics and lipid profiles are given in Table 1.
Lipid profile of study participants
*LDL-cholesterol calculated using the Friedewald equation
Both AG and UAG were found to bind to lipoproteins but demonstrated different patterns of binding; AG was found in approximately equal concentrations in VLDL (26%), LDL (22%), HDL (23%) and was present as a plasma protein (27%). UAG bound more specifically to HDL (49%) and was present as a plasma protein (48%) (Figure 1).
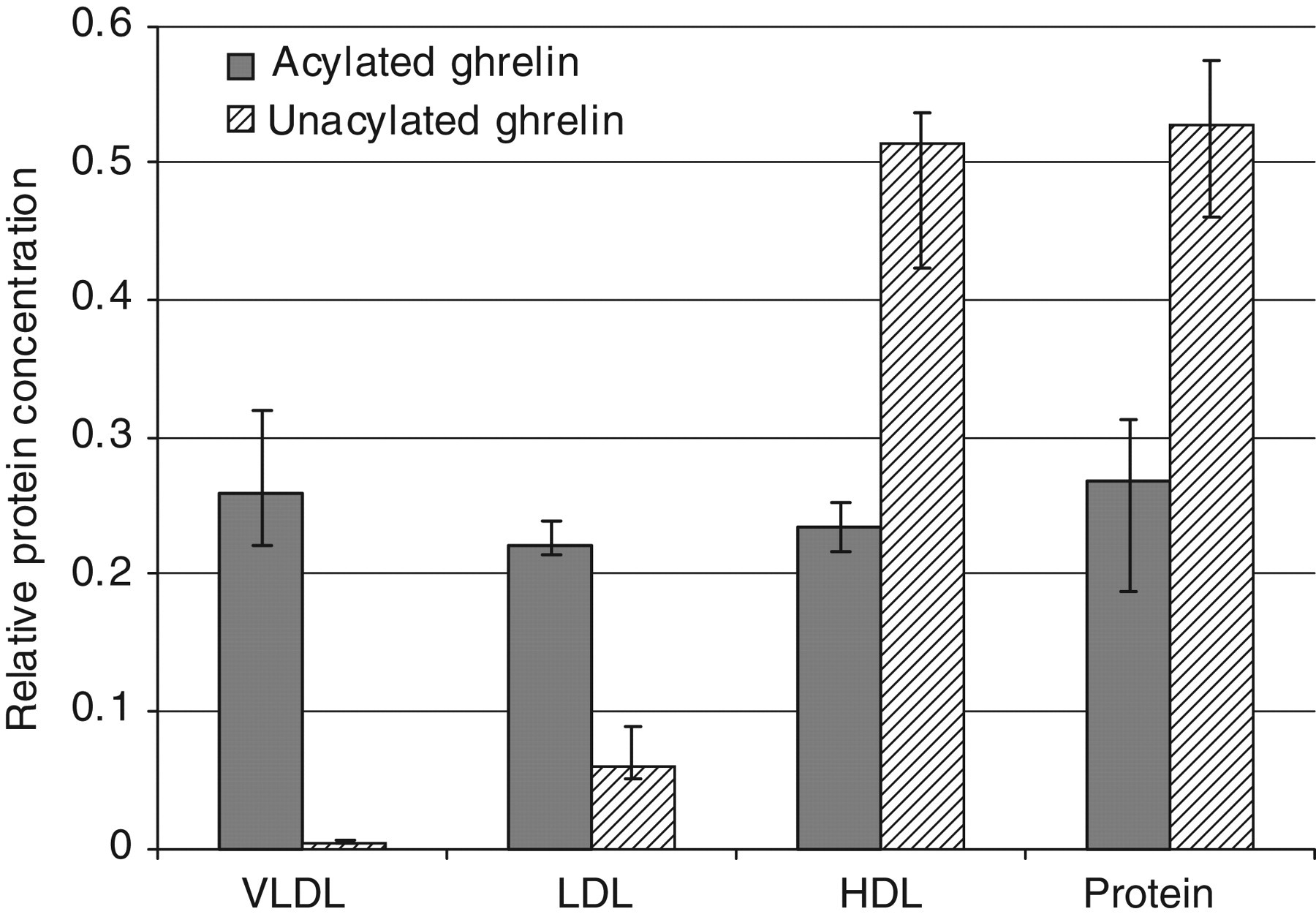
Ghrelin distribution in plasma. Results shown as median
Discussion
This study has demonstrated that AG binds to all lipoproteins, while UAG binds more specifically to HDL. This pattern of AG binding is supported by a previous study which found AG bound to all lipoproteins, with the acyl group essential for binding to VLDL and LDL, 7 possibly through a non-specific, hydrophobic interaction between the acyl group and the lipoprotein membrane. The pattern of HDL binding indicates a more specific binding mechanism. In contrast to previous reports, no UAG bound to VLDL; however, these data agree with reports that ghrelin binds to HDL by a mechanism independent of the acyl group. 7 These results clarify the apparent discrepancy reported between the lipoprotein-binding patterns and we can now conclude that UAG binds only to HDL.
When considering the results of this study, two questions should be considered; what is the effect of lipoprotein binding on ghrelin action and metabolism, and does the binding of ghrelin to lipoproteins explain the relationships observed between ghrelin and cardiovascular disease.
The biological action of ghrelin is mediated by the specific interaction of ghrelin with its receptor. The implicit assumption, therefore, is that the hormone is free and available for binding at its receptor. Ghrelin binding to lipoproteins may therefore add an additional level of complexity to ghrelin metabolism, through stabilization of AG, or by preventing AG and UAG from binding to receptors. Any alteration in the concentration of circulating lipoproteins, either through the production of chylomicrons following feeding, or through pathological increases in VLDL and LDL, may therefore affect the concentration of free hormone available for receptor binding.
One limitation of the studies published to date is the wide use of non-specific, TGR, radioimmunoassays that measure both AG and UAG. Given the different patterns of lipoprotein binding, analysis of AG and UAG by separate immunoassays would be more informative. For example, as UAG is the predominant form of ghrelin and binds specifically to HDL, it is probable that the positive relationship reported between TGR and HDL-cholesterol 5 reflects UAG binding by HDL.
A positive relationship has been described between TGR and atherosclerosis in men, 9 which may be a reflection of higher lipoprotein concentrations, both contributing to the development of atherosclerosis and stabilizing ghrelin. AG has also been shown to be an antioxidant, 3 therefore binding of AG to LDL may provide some protection against the oxidation of LDL, which is fundamental to the development of atherosclerotic plaques. The binding of ghrelin to lipoproteins may therefore not only provide a reason for the observed relationships between ghrelin, LDL-cholesterol and HDL-cholesterol, but may actively contribute to the cardioprotective role of ghrelin.
In summary, using specific immunoassays we have clarified the binding of ghrelin to lipoproteins and the different binding patterns observed for AG and UAG emphasizes the need to study their cardiovascular actions separately. The results further cement the close relationship between obesity and cardiovascular disease; however, further research is needed to clarify the biological significance of AG and UAG both in health and disease.
DECLARATIONS