
Abstract
Background
We found a unique cholesteryl ester transfer protein (CETP) deficient case with markedly elevated serum triglyceride (TG) as well as high-density lipoprotein cholesterol (HDL-C) levels. Most of the CETP deficiency cases were reported to have normal or reduced serum TG with elevated HDL-C.
Methods
The case subject was a 40-year-old male with a compound heterozygous CETP deficiency. Two heterozygous CETP deficient cases and 10 normal volunteers were also recruited as controls. They underwent an oral fat tolerance test (OFTT) and their blood was taken at fasting and during the OFTT to be used for laboratory tests.
Results
The case subject had apolipoprotein E (apo-E) phenotype 4/2 with fatty liver but without any cardiovascular disease. His serum TG, HDL-C, apo-AI and apo-B48 levels were significantly higher, but the low-density lipoprotein cholesterol level was lower than controls. Although post-heparin plasma lipoprotein lipase and hepatic lipase (both mass and activity) were nearly normal, the serum level of angiopoietin-like-protein-3 was extremely elevated. While his serum remnant-like particles-TG (RLP-TG) and total TG levels significantly increased after a fat load, the RLP-cholesterol (RLP-C) level did not increase during OFTT.
Conclusions
The case subject was different from the common CETP deficient cases reported previously. Also, the results indicated that the metabolic pathways of RLP-C and RLP-TG formation in the postprandial state are controlled independently in CETP deficient cases. CETP deficiency itself may not be atherogenic, while one with elevated RLPs may be atherogenic. These cases may have raised the controversy of whether CETP deficiency is atherogenic or not.
Introduction
Elevated postprandial triglyceride (TG)-rich lipoprotein levels have been reported to be a risk for atherosclerosis. 1 In general, serum TG concentration increases after a meal and the magnitude of the elevation is mostly dependent on the amount of fat intake. 2 After a fat load, both chylomicron and very low-density lipoprotein (VLDL) remnant levels are known to increase. 3 We have investigated the postprandial remnant lipoprotein metabolism using an assay of remnant-like particle (RLP) immunoseparation method as a surrogate measurement of remnant lipoproteins. 4–7 In normal individuals, both RLP cholesterol (RLP-C) and triglyceride (RLP-TG) levels increased almost in parallel after a fat load. An abnormal increase in RLP-C and RLP-TG levels after a fat load is closely associated with coronary heart disease (CHD) risks.
Cholesteryl ester transfer protein (CETP) is known to play a key role in high-density lipoprotein (HDL) metabolism. HDL exchanges its cholesterol esters with the TGs of other apolipoprotein B carrying lipoproteins in the presence of CETP. In patients with CETP deficiency, the plasma cholesterol (TC) level is usually very high because the HDL cholesterol level (HDL-C) is strikingly higher than that in normal individuals. Many genetic studies on CETP deficiency have been reported in the last decades. 8–11 In cases of homozygous mutation, CETP mass and activity are not detectable because of the complete gene defect. In contrast, the serum HDL-C level was often reduced by an accelerated CETP activity observed in patients with type 2 diabetes and/or CHD. 12,13 Therefore, an elevated CETP activity was considered to be atherogenic and CETP inhibitors were developed as a drug for the prevention of cardiovascular diseases. 14
Recently, we found a very unique CETP deficiency case with both elevated TG and elevated HDL-C levels. We investigated whether or not a new mutation was present, and the reasons for not only HDL-C but also TG levels being elevated were elucidated in this case subject through various markers, including serum levels of angiopoietin-like-protein-3 (ANGPTL3), lipoprotein lipase (LPL), hepatic lipase (HTGL) and endothelial lipase (EL). 15–18
Materials and methods
Case and control subjects
The case subject was a 40-year-old Japanese male of 180 cm height, 68 kg body weight and 20 kg/m2 body mass index. He had never pointed out any abnormality except hyperlipidaemia. Physical examination showed no particular abnormality. Blood analysis showed no anaemia (a red blood cell count of 515 × 104/μL and a haemoglobin level of 15.8 g/dL). His serum aspartate aminotransferase, alanine transaminase, creatine phosphokinase and lactate dehydrogenase levels were within normal limits as 23, 22, 121 and 175IU/L, respectively. However, his abdominal ultrasound image showed fatty liver without hepatomegaly or splenomegaly. Ophthalmological examination showed overt atherosclerosis to date in arteries in his retinas. His paternal line did not show high levels of serum TG or HDL-C. Unfortunately, his familial history in the maternal line could not be followed.
Two patients with heterozygous CETP deficiency (CC-1: 66-year-old female; CC-2: 67-year-old female) and 10 male normolipidaemic volunteers (mean age 40 ± 1 years) as control subjects were recruited to compare their lipid and lipoprotein profiles with those of the case subject. All subjects participated in an oral glucose tolerance test (OGTT) and an oral fat tolerance test (OFTT) as described below. All the studies were conducted under the approval of the ethical committee of Tokyo Medical and Dental University.
Lipid and lipoprotein analysis
Serum concentrations of TC, TG, HDL-C, low-density lipoprotein cholesterol (LDL-C) (Dai-ichi, Tokyo, Japan), RLP-C and RLP-TG (JIMRO, Takasaki, Japan) as well as apolipoprotein AI, AII, total B, CII, CIII, E (Dai-ichi, Tokyo, Japan) and B48 (Fuji-rebio, Tokyo, Japan) were measured at all time points of OGTT and OFTT. Serum lipoprotein profile and apolipoprotein E phenotype were determined by the isoelectric focusing method (Joko, Tokyo). CETP mass was determined by enzyme-linked immunosorbent assay (ELISA) (Dai-ichi, Tokyo, Japan). High-performance liquid chromatography (HPLC) analysis of RLP was conducted by the method of Usui et al. 19
Post-heparin plasma concentrations (mass) of LPL and HTGL were measured as previously reported 20 and LPL and HTGL activity was measured by the newly developed methods of Imamura et al. 21,22 The serum concentration of ANGPTL3 was determined by the sandwich ELISA system. 17,18
CETP gene; analysed by PCR and sequencing
DNA was extracted from peripheral blood cells from these CETP deficient cases and analysed by polymerase chain reaction as reported by Inazu et al. 8,9
Oral fat tolerance test
All the participants performed an OFTT as previously reported 4–6 within a month after the OGTT at Tokyo Medical and Dental University. Briefly, after 12 h fasting, the subjects ingested 17 g/m2 body surface area of fat emulsion (OFTT cream, Jomo Foods, Co Ltd, Takasaki, Japan). Blood samples were taken before and 60, 120, 240 and 360 mins after an oral fat load. For the normolipidaemic volunteers, blood samples were taken before and 120 and 240 mins after a fat load. Plasma glucose (PG) and serum TC, TG, HDL-C, LDL-C, RLP-C, RLP-TG, apolipoproteins and insulin levels were determined as previously reported. 7
Oral glucose tolerance test
All the participants performed a 75 g OGTT to determine their glucose tolerance. 5,6,23 Blood samples were taken before and 30, 60, 90, 120 and 180 mins after an oral glucose loading. PG and serum TC, TG, HDL-C, LDL-C, RLP-C, RLP-TG, apolipoproteins and insulin levels were determined.
Statistics
StatView-J 5.0 software was used for all statistical analyses. P < 0.05 means statistically significant.
Results
Case subject
Table 1 shows the characteristics and fasting serum levels of CETP, LPL, HTGL and ANGPTL3 in the case subject. The CETP mass of the case subject was under detective limits. Analysis of the CETP gene using polymerase gel reaction (PCR) revealed a compound heterozygote of Intron 14 G(+1) > A and R268X. Apo-E phenotype of the case subject was E4/2 and all the control cases were E3/3. Post-heparin LPL mass and activity and post-heparin HTGL mass and activity were within normal range. ANGPTL3 in this case was significantly higher than in the normal population.
Characteristics and fasting serum levels of cholesteryl ester transfer protein (CETP), lipoprotein lipase (LPL), hepatic lipase (HTGL) and angiopoietin-like-protein-3 (ANGPTL3) in the case subject
HPLC profile of RLP isolated from the case subject
RLP-C in the case subject monitored by HPLC was shown to be a similar RLP profile of a common hypertriglyceridaemia, indicating a large VLDL size as a main peak and a large HDL size as a minor peak (Figure 1) in fasting state. This profile was different from those in homozygous CETP deficiency cases reported by Inazu et al. 24 After a fat load, the RLP-TG/RLP-C ratio of the case subject increased significantly, indicating the increase of RLP with VLDL size. 25
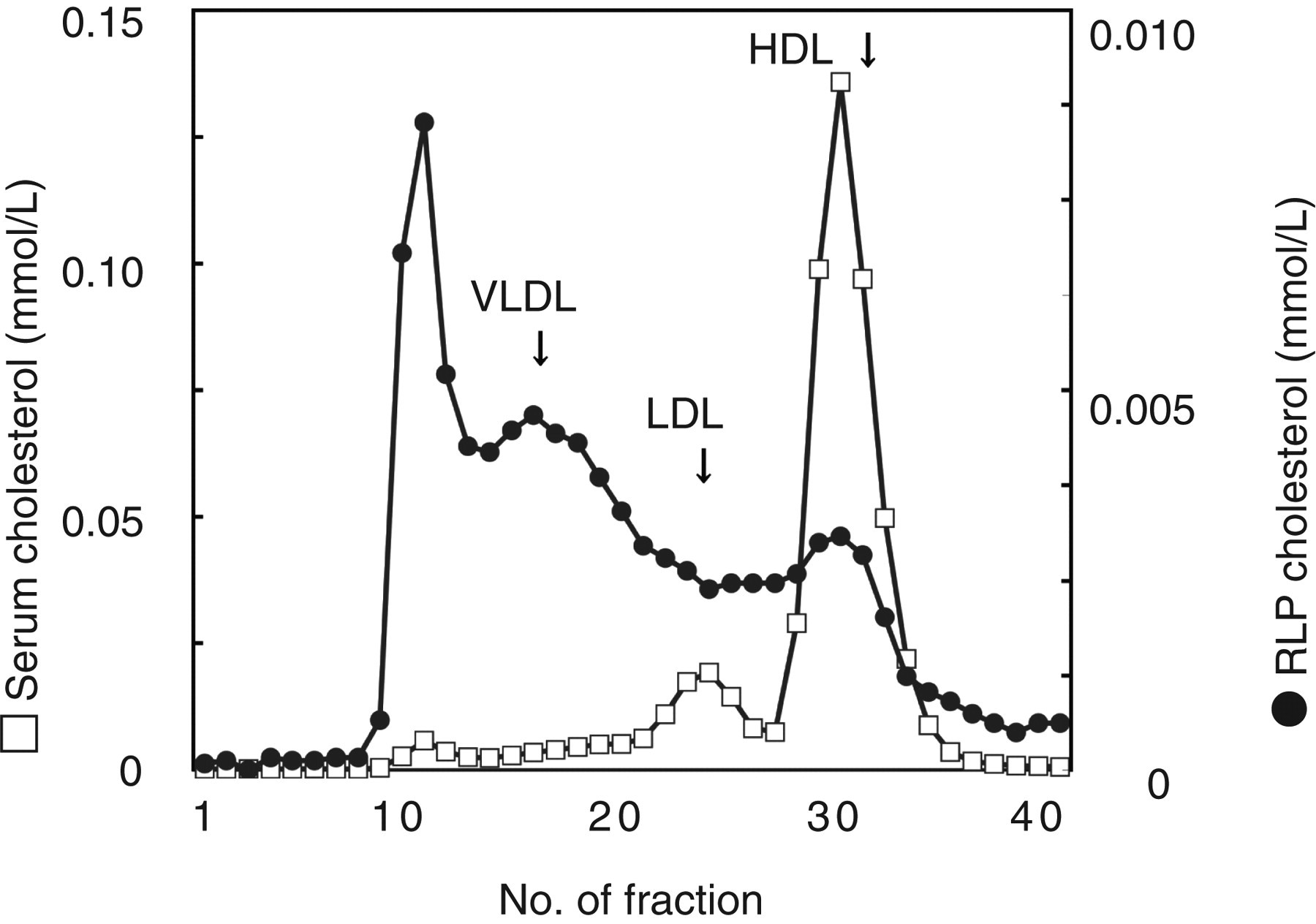
High-performance liquid chromatography (HPLC) profile of plasma and remnant-like particle (RLP) isolated from the plasma of the cholesteryl ester transfer protein (CETP) deficient case subject. HPLC profiles of plasma and RLP were monitored by total cholesterol. Plasma profile showed abnormally high high-density lipoprotein cholesterol (HDL-C) and low LDL-C. The major particle size of RLP was found in large and small VLDL fractions, which were the similar particle sizes commonly found in CAD patients. However, smaller particles, large HDL particles (apo-E-rich HDL), were also observed as the fraction found in CETP deficient cases
Oral fat tolerance test
Table 2 shows the serum concentrations of lipids and lipoproteins. For serum levels of TG, RLP-C and RLP-TG, the values were plotted in Figure 2. Serum concentrations of TG, HDL-C, RLP-C, RLP-TG, apo-AI, apo-AII, apo-B48, apo-CII, apo-CIII and apo-E of the case subject were higher than those of normal controls. The serum LDL-C level of the case subject was lower than that of other participants. The two typical cases (CC-1 and CC-2) of heterozygous CETP deficiency (Intron 14 G(+1) > A, CETP levels below 1.0 μg/mL) with elevated HDL-C and apo-AI were compared with this case. CC-1 shows the typical large HDL size RLP (apo-E-rich HDL), indicating the RLP-TG/RLP-C ratio (<1.0) in the fasting and after a fat load as reported by Inazu et al. 24 in CETP deficiency cases. CC-2 shows a similar RLP-TG/RLP-C ratio (1.1) with CC-1 in the fasting state indicating the presence of large HDL size RLP, but in 120 and 240 mins the ratio increased as in normal CETP cases. These results indicate that CC-2 has both large HDL size RLP (apo-E-rich HDL) and ordinary VLDL size RLP after a fat load.
Changes in serum lipids and apolipoprot in cases of cholesteryl ester transfer protein deficiency and in normal subjects during an oral fat tolerance test (OFTT)
TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; RLP-C, remnant-like particles-cholesterol; RLP-TG, remnant-like particles-triglyceride
CC-1 and -2 were patients with heterozygous cholesteryl ester transfer protein deficiency
Values of normal controls are expressed as mean ± SD
Serum concentrations of TG and RLP-TG of the case subject increased significantly and peaked at 240 mins after an oral fat load (delayed peak compared with 120 min in normal controls) and then decreased (Figure 2). However, the RLP-C level did not increase, but rather decreased during OFTT. PG and serum TC, HDL-C, LDL-C and insulin levels did not change during the observation. The serum apo-AI level slightly increased throughout the observed period, while the serum levels of apo-AII, B, CII, CIII and E did not change. Fasting apo-B48 level in this case subject was higher than that of an average Japanese population. 26 The Apo-B48 level in this case subject did not increase significantly after OFTT (Table 2).
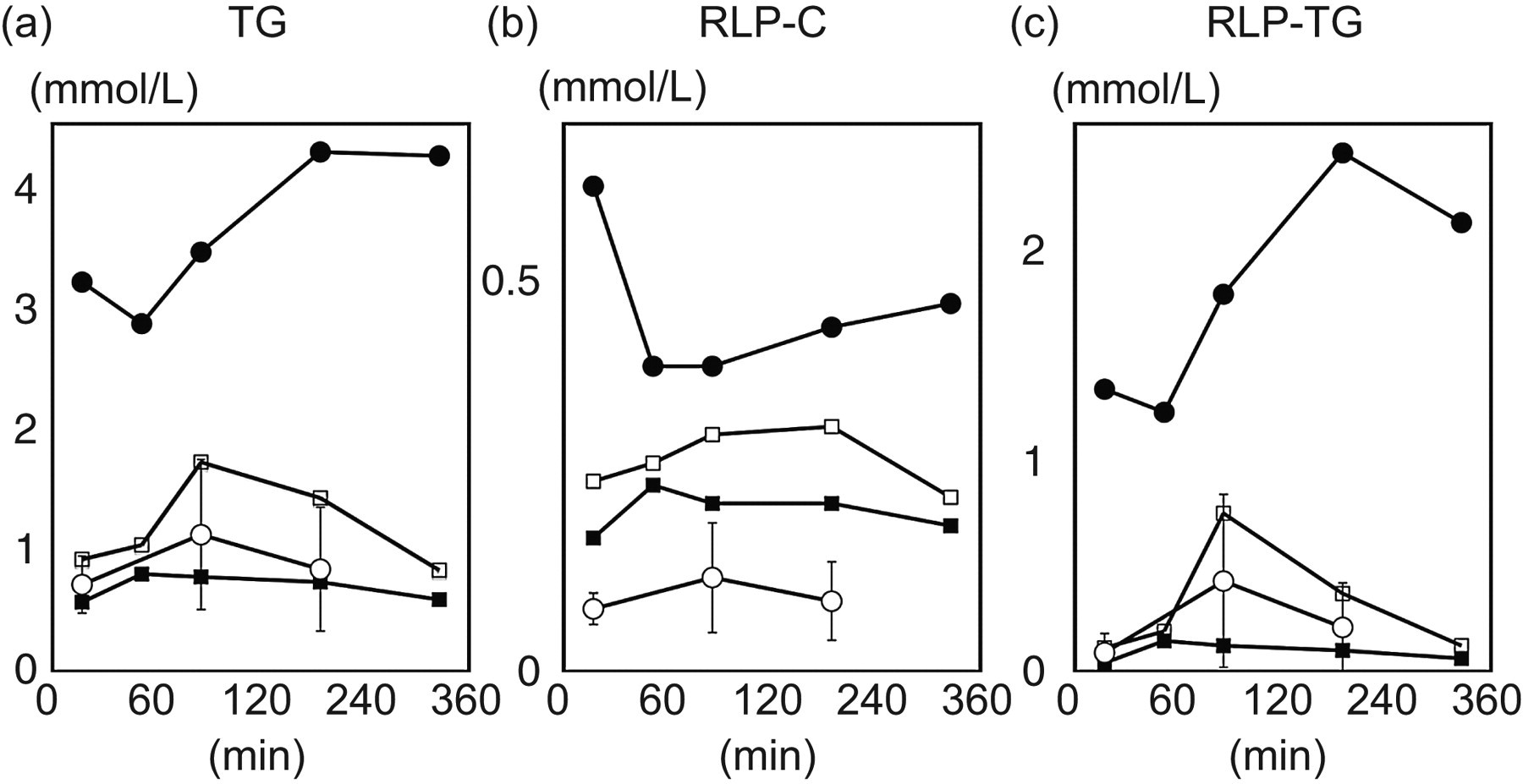
Serum triglyceride (TG) (a), remnant-like particle-cholesterol (RLP-C) (b) and remnant-like particle-triglyceride (RLP-TG) (c) levels of the CETP deficient case subject (•), the CETP deficient controls (CC-1: ▪ and CC-2: □) and normolipidaemic controls (○, mean ± SD) during an oral fat tolerance test (OFTT). The CETP deficient case subject showed a significant increase of TG and RLP-TG in 240 mins after a fat load, but RLP-C levels rather decreased during OFTT. In control subjects, RLP-C increased parallel with RLP-TG and TG after an oral fat load
For normal volunteers, the serum levels of TG, RLP-C and RLP-TG increased after a fat load and peaked at 120 mins, and then decreased. Other parameters did not change during OFTT. In CC-1 (one of the 2 heterozygous CETP deficient subjects), RLP-C, RLP-TG and TG levels increased slightly after a fat load. In CC-2 (the other heterozygous CETP deficient subject), RLP-C, RLP-TG and TG levels markedly increased at 120 min after a fat load as in normal individuals (Figure 2). The increase of VLDL size RLP was also detected in the case subject, but the increase was within normal range as shown previously. 4
In the case subject and CC-2, the decrease of RLP-C started later than that of RLP-TG during OFTT, which was rarely observed and different from normal individuals. 4
Oral glucose tolerance test
While PG and serum insulin concentrations in normal volunteers peaked at 30 mins after glucose loading and then returned to the baseline promptly, those in the case subject peaked late (Figure 3). PG concentration at 120 mins after loading in the case subject was 8.4 mmol/L (152 mg/dL) and he was diagnosed as impaired glucose tolerant (IGT). Other participants were normal glucose tolerant by the criteria of the American Diabetes Association. 27 For all participants, the sum of the six measurements of serum insulin concentration was within normal range. The profiles of serum lipids and lipoproteins during OGTT in the case subject were similar to other controls. HbA1c of the case subject was 5.1%, which was slightly higher than that of other participants (4.8 ± 0.1%) but all of them were within normal range.
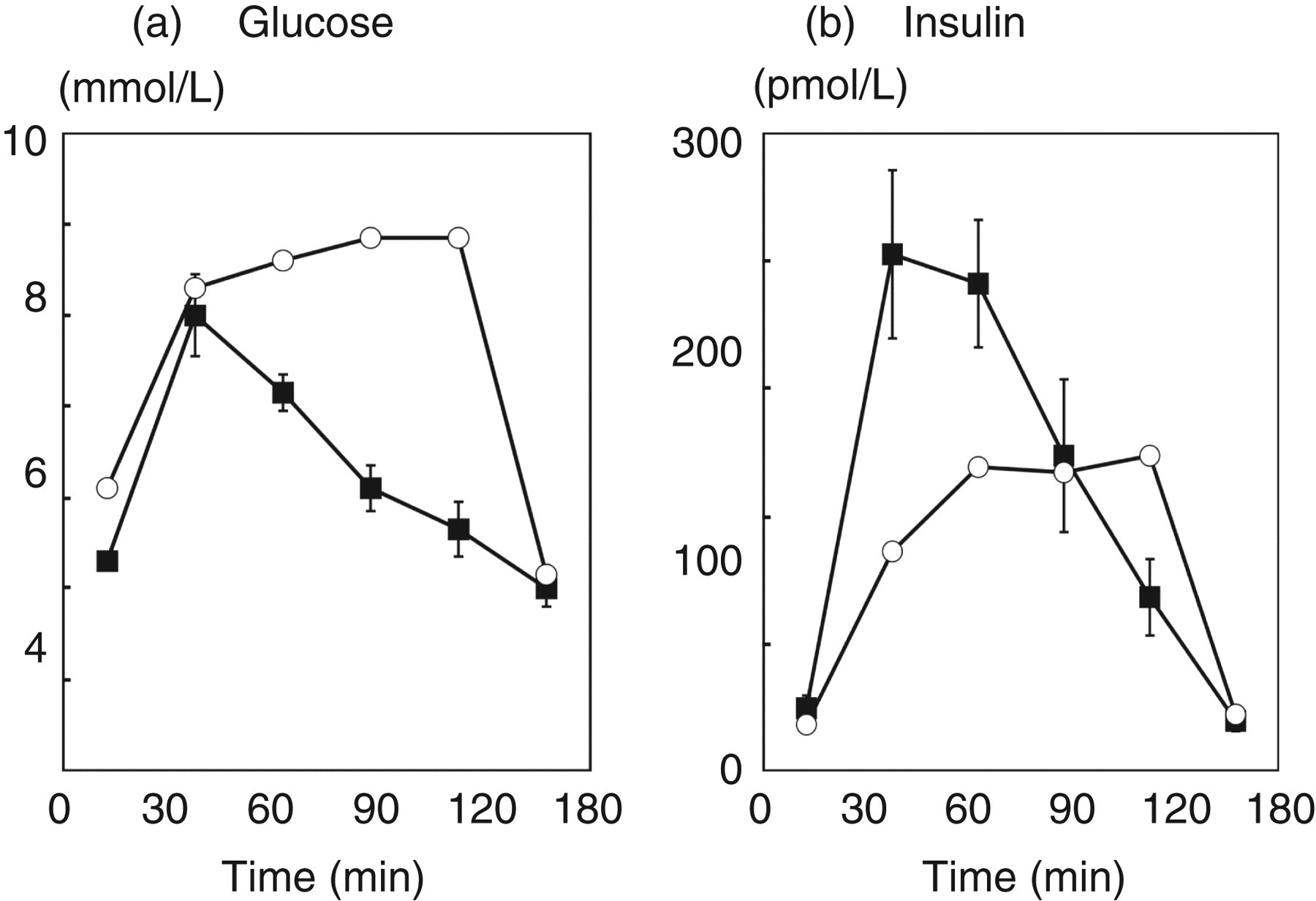
Plasma glucose (PG) (a) and serum insulin (b) concentrations during 75 g oral glucose tolerance test in the case (○) and in normal volunteers (▪). While PG and serum insulin concentrations of normal volunteers peaked at 30 mins after glucose loading and then returned to the baseline promptly, those of the case peaked late. PG concentration at 120 mins after loading in the case was 8.4 mmol/L (152 mg/dL) and he was diagnosed as impaired glucose tolerance by the criteria of the American Diabetes Association
Discussion
We found a unique profile of serum postprandial RLP-C and RLP-TG during OFTT in a male CETP deficiency, aged 40, whose serum HDL-C, apo-AI and TG levels were abnormally elevated. From genetic analysis, this case was a known compound heterozygote with known mutation of Intron 14 G(+1) > A and R268X. 8,28 The former mutation was a common one but the latter had not been reported previously in Japanese populations. That is why his CETP mass was less than the detected limit. Because of CETP deficiency, his HDL cannot exchange its cholesteryl ester with the TG of other lipoprotein particles, including RLP. 24,29 In this case, it is not easy to assume that CETP deficiency originated the cause of this unique profile of postprandial RLP-C and RLP-TG. A similar CETP deficient case with abnormally elevated TG was previously reported by Ritsch et al. 30 and precise genetic analysis of CETP was performed to find the cause of the dissociation between cholesteryl ester and TG transportation in plasma. However, they could not find any specific cause for it in their case, besides the fact that she was completely CETP deficient and an apo-E2 carrier.
Serum levels of RLP-C and RLP-TG as well as total TG usually increased and decreased in parallel after an oral fat load in normal individuals. Also, both RLP-C and RLP-TG in CETP deficient cases were fairly reduced, as reported previously by Inazu et al. 24 . However, in this case subject, the serum RLP-C level was highly elevated in fasting and did not increase after a fat load but rather decreased, while the RLP-TG and total TG levels significantly increased after a fat load with a delayed peak time compared with those of normal control subjects. This phenomenon indicated that CETP and HDL played an important role for the formation of RLP-C, as previously reported on postprandial lipid metabolism in homo- and heterozygous CETP deficiency cases 24 and as reported on an in vitro study by Okamoto et al. 29
However, interestingly, RLP-TG and total TG levels in the case subject increased significantly at 240 mins after a fat load like those in common hyperlipidaemic patients. The trend of the case subject was similar to that of individuals treated with estrogen whose serum RLP-C level is reduced but RLP-TG level increases after the treatment. 31,32 This means that the major metabolic pathway of RLP-C and RLP-TG in the postprandial state is controlled independently, although the RLP particle itself is composed of the same structure as other lipoproteins with TC, TG, phospholipids and apolipoproteins and isolated by the same immunoseparation method. 33 In the case subject, we found an extremely elevated plasma level of ANGPTL3, which was discovered as an inhibitory modulator of LPL and HTGL in mice. 15 However, it was recently reported that ANGPTL3 associates more strongly with EL, which controls HDL-C metabolism, but not with TG in humans. 16,18 As the case subject showed nearly normal LPL and HTGL activity in post-heparin plasma, ANGPTL3 might not affect RLP-TG levels associated with LPL and HTGL activities. However, the lack of CETP together with enhanced EL inhibition by elevated ANGPTL3 may have significantly increased the HDL-C level, especially apo-E-rich HDL in this case.
Another interesting dissociation between RLP-C and RLP-TG was observed in one of the heterozygous CETP deficient subjects (CC-2) after a fat load. We usually observe that serum RLP-C and RLP-TG levels increase and decrease almost in parallel after an oral fat load in a normal population. 4–6 However, as shown in CC-2, the heterozygous CETP deficient subject with increased RLP-C and RLP-TG (VLDL remnants) after a fat load showed that RLP-TG was decreased in 240 mins and RLP-C in 360 mins (Figure 2). The dissociation might be associated with the magnitude of CETP deficiency, in which CC-2 still promoted the formation of VLDL size RLP-C and RLP-TG, but was not capable enough to complete the normal metabolic pathway between CETP and LPL. 34 These cases may be associated with some genetic disorder of CETP or its activity, which revealed faster RLP-TG decrease than that of RLP-C. However, we could not try further genetic analysis of CETP in CC-2.
The apo-B48 level in this study case was significantly elevated as in type III cases as previously reported, 35 and apo-B48 did not increase after a fat load like RLP-C in this case. CETP deficiency may inhibit the formation of both chylomicron and VLDL remnants in this case. CC-2 showed a closer correlation of postprandial increase between apo-B48 and RLP-C than between apo-B48 and RLP-TG. Therefore, the formation of RLP-TG may be controlled by some independent factors from CETP.
In the case subject, fasting serum TG, RLP-C and RLP-TG levels were much higher than those of controls. The peak time of TG and RLP-TG after an oral fat load was delayed when compared with that of other participants (Figure 2). One of the causes for this phenomenon could be associated with IGT (Figure 3). Although he was not obese and his fasting serum insulin level was within normal range, he had a fatty liver and IGT. IGT individuals are known to have elevated serum RLP-C and RLP-TG levels and to have a high risk for CHD. 6,23 CETP deficiency itself may not be atherogenic, whereas together with elevated RLPs may be atherogenic and cause CHD. These cases may have caused the controversy of whether CETP deficiency is atherogenic or not.
In conclusion, the metabolic pathway of RLP-C and RLP-TG may be controlled independently in the postprandial state. As post-heparin LPL and HTGL activities were normal, the elevated ANGPTL3 level did not affect the increase of the postprandial RLP-TG level, but rather may be associated with the significant increase of HDL-C by inhibiting EL activity. This CETP deficient case may have a risk of cardiovascular events because of elevated RLP-C and RLP-TG regardless of elevated HDL-C. More cases of CETP deficiency with elevated remnant lipoproteins are necessary to be recruited and further investigations will be needed for the analysis of this dyslipidaemia.
DECLARATIONS
All authors planned this study, determined the data, and approved the manuscript. Masumi Ai, Akira Tanaka, Takamitsu Nakano and Katsuyuki Nakajima analysed the data and outlined the manuscript.