
Abstract
Heterophilic antibodies are polyspecific natural human antibodies that bind to animal immunoglobulins. 1,2 These antibodies interfere in immunoassays by forming a bridge between the capture and detection antibodies, leading to false-positive results. Interference with false-negative results is rarely observed. The incidence of interference in immunoassays has been reported to range from 0.4% to 4%, 3 although an estimate of only 0.05% has also been suggested. 1 The magnitude of interference depends on the affinity of the heterophilic antibody (binding strength between the antigen and antibody) and its concentration in serum. 3
In our laboratory, we occasionally observe samples in which the free fraction of prostate-specific antigen (PSA) exceeds total PSA. Owing to this unexpected presentation, the possibility was raised that heterophilic antibodies interfere in the free PSA assay. This interference can be detected by the addition of non-specific blocking agents (animal serum or purified non-immune globulin) or specific blocking agents (specific commercial products for the reduction of interference by heterophilic antibodies) to the assay, execution of a parallel assay and serial dilutions of the samples. 1,2
We selected five PSA samples in which the concentration of the free fraction was higher than that of total PSA measured by the Beckman–Coulter Unicel DxI® (Beckmann Coulter Inc. Brea, CA, USA) chemiluminescent immunometric assay (Hybritech® free PSA and Hybritech® PSA tests, Beckmann Coulter Inc. Brea, CA, USA). In parallel, the samples were tested using an Abbott chemiluminescent immunometric assay on the Architect® (Abbott Laboratories Diagnostic Division, Abbott Park, IL, USA) platform (free PSA and total PSA). Both assays use mouse capture and detection monoclonal antibodies. The samples were pretreated with heterophilic blocking tube (HBT) (Scantibodies Laboratory). The main components of HBT are mouse antibodies against heterophilic antibodies in human fluids. Before use, the absence of interference of HBT in the assay should be tested. Previous evaluation of the Beckmann free PSA assay has shown that the assay is adequate for the combined use with HBT. 2 In that study, a reduction of more than 80% in PSA levels after treatment of the sample with HBT was considered to indicate interference by heterophilic antibodies. 2
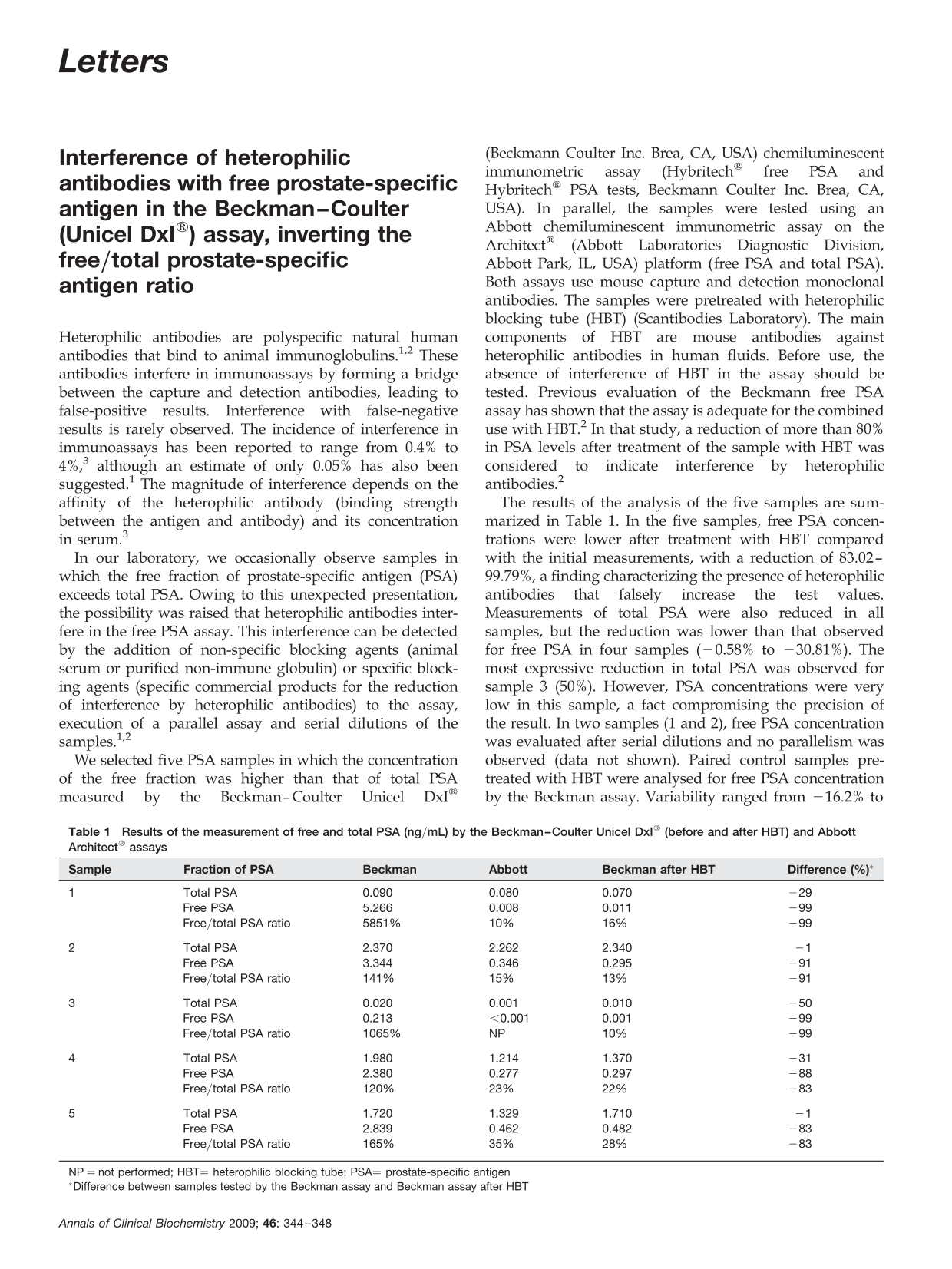
The results of the analysis of the five samples are summarized in Table 1. In the five samples, free PSA concentrations were lower after treatment with HBT compared with the initial measurements, with a reduction of 83.02–99.79%, a finding characterizing the presence of heterophilic antibodies that falsely increase the test values. Measurements of total PSA were also reduced in all samples, but the reduction was lower than that observed for free PSA in four samples (−0.58% to −30.81%). The most expressive reduction in total PSA was observed for sample 3 (50%). However, PSA concentrations were very low in this sample, a fact compromising the precision of the result. In two samples (1 and 2), free PSA concentration was evaluated after serial dilutions and no parallelism was observed (data not shown). Paired control samples pretreated with HBT were analysed for free PSA concentration by the Beckman assay. Variability ranged from −16.2% to +21.54% for free PSA and from −9.92% to +14.21% for total PSA when compared with the non-pretreated sample.
Results of the measurement of free and total PSA (ng/mL) by the Beckman–Coulter Unicel DxI® (before and after HBT) and Abbott Architect® assays
NP = not performed; HBT= heterophilic blocking tube; PSA= prostate-specific antigen
*Difference between samples tested by the Beckman assay and Beckman assay after HBT
In 2006, Park et al. published a case report in which interference in the PSA assay was demonstrated by a higher free fraction of PSA compared with total PSA in a postsurgery patient. The Hybritech® PSA assay (Beckman–Coulter) was also used and subsequent pretreatment of the samples with human antimouse heterophilic antibody blocking reagent resulted in a reduction of total PSA concentrations. Interestingly, the authors observed lot-to-lot variability in total PSA concentrations due to the presence of heterophilic antibodies. 4
Discrepant results have been reported by another group of investigators, notably higher free PSA concentrations than expected in a patient with a malignant tumour of the prostate. 5 In one of the assays tested (Immulite® [Diagnostic Product Corporation, LA, USA] Free PSA), free PSA concentration was higher than total PSA concentration. The authors raised the possibility of an alternative structure of the PSA molecule, leading to a reduced recognition by anti-PSA antibodies used in some assays and reduced binding to α 1-antichymotrypsin. 5
The incidence of interference by heterophilic antibodies in free and total PSA assays has been reported to be 1% and 1.2%, respectively. 2 In conclusion, we have presented five cases in which the free PSA concentration was higher than total PSA due to interference by heterophilic antibodies. PSA was measured using the Unicel DxI® (Beckman–Coulter) system, with total PSA concentrations ranging from 0.01 to 2.34 ng/mL.
Declarations