
Abstract
Background
To decrease the incidence of neural tube defects, active efforts are currently undertaken to promote folic acid (FA) intake among women. In 2003, the Food and Drug Administration approved the proposal of introducing an oral contraceptive (OC) and FA combination pill. It is unknown whether these pills will reduce neural tube defect incidence for couples who do not become pregnant soon after discontinuation. We studied FA kinetics up to 12 weeks discontinuation of eight weeks 500 μg/d FA in 27 healthy Dutch women of child-bearing age.
Methods
In this controlled study, women were assigned to an intervention group (n = 13) or a control group (n = 14). The total study duration was 20 weeks, during which the subjects had to give blood on nine occasions (week –8 [baseline], –4, 0, 1, 2, 3, 4, 8 and 12) for analyses of serum and erythrocyte folate, and plasma total homocysteine. The intervention group received 500 μg/d FA during the first eight weeks, and discontinued the intake from weeks 0 to 12. No supplements were supplied to the control group.
Results
Serum folate and plasma total homocysteine returned to baseline after 12 weeks of FA discontinuation, erythrocyte folate did not.
Conclusion
An FA/OC combination pill seems to be of value for only a minor portion of women. Active efforts to stimulate women of child-bearing age to take FA remain essential.
Introduction
Increased periconceptional intake of folic acid (FA) reduces the risk of neural tube defects (NTDs) up to 70%, 1,2 and is also related to a lower risk of other birth defects. 3 Worldwide, women are recommended to take at least 400 μg/d FA from four weeks before conception until eight weeks thereafter. 4,5 In many countries the recommended intake is not achieved, particularly among women who are younger, less educated, single or who have not planned their pregnancy. 6,7 It is estimated that each year 4000 pregnancies in Europe are complicated by an NTD. 4 Active efforts are currently undertaken to promote FA intake among women. One of these is FA food fortification, probably accounting for a 19–54% reduction in NTDs. 5,8 In 2003, the Reproductive Health Drugs Advisory Committee of the Food and Drug Administration approved the proposal of introducing an oral contraceptive (OC)/FA combination pill. 9 To gain insight into the ability of these pills to lower the incidence of NTDs in women who stop using OC to become pregnant, we studied FA kinetics up to 12 weeks discontinuation of eight weeks 500 μg/d FA in healthy Dutch women of child-bearing age.
Participants and methods
Healthy premenopausal women ≥18 years were eligible to participate. A questionnaire was used to gain information on general health, and medication, OC and supplemental vitamin use. Women who were pregnant, had the wish to become pregnant during the study period, had a history of psoriasis, epilepsy, renal, heart and vascular disease, or who used high-dose vitamin supplements or drugs interfering with folate metabolism were excluded. The study was approved by the Medical Ethical Committee of the University Medical Centre Groningen and volunteers gave written informed consent. The protocol was compliant to the Helsinki Declaration of 1975 as revised in 1996.
The total study duration was 20 weeks. Subjects had to give blood on nine occasions for the analysis of serum and erythrocyte folate, and plasma total homocysteine (tHcy). Participants were assigned to an intervention or a control group. The intervention group received 500 μg/d FA (Pharmachemie, Haarlem, The Netherlands) during the first eight weeks of the study (week –8 until 0). Most over-the-counter FA pills in the Netherlands for women who are pregnant or hoping to become pregnant contain 400–500 μg FA. Differences, if any, are expected to be small. A 500 μg supplement was chosen, since we expected folate status to return to baseline after 12 weeks discontinuation. Thus similar results would apply for the lower 400 μg dosage. Tablets were taken at breakfast and on sampling days after blood collection. Tablets were supplied in tubes for 14 days. No tablets were supplied to participants in the control group. All participants were asked not to change their diet or their use of vitamin supplements and OC pills during the study period.
Blood samples were taken in week –8 (baseline), –4, 0, 1, 2, 3, 4, 8 and 12. During each visit, 20 mL blood (1 EDTA tube and 1 serum tube) was collected after a 10-h fast. EDTA blood was put on melting ice in the dark. For erythrocyte folate analysis, haematocrit was analysed with a Coulter STKS (Coulter Corporation, Miami, FL, USA), and 50 μL blood was diluted with 1-mL ascorbate solution (5 mg/mL) and left in the dark for 90 min. After storage at −20°C for a maximum period of one week, 100 μL 5% bovine serum albumin was added prior to the analysis. Serum folate (local reference values, 4–30 nmol/L), erythrocyte folate (340–990 nmol/L) and serum vitamin B12 (145–450 pmol/L) were measured by a fluoroimmunoassay (AutoDELFIA, Wallace Oy, Turkey, Finland, Germany). Whole blood vitamin B6 (35–136 nmol/L) was measured by reversed-phase high-performance liquid chromatography with fluorescence detection. 10 Haemoglobin (Hb, 7.5–9.9 mmol/L) and mean cellular volume (MCV, 80–96 fL) were measured at weeks –8, 0 and 12 only with a Coulter STKS (Coulter Corporation). Plasma tHcy (5–15 μmol/L) was measured by a fluorescence polarization immunoassay (FPIA ImX; Abbott Laboratories, Abbott Park, IL, USA). Serum methylmalonic acid (MMA) was measured by gas-chromatography negative ion chemical ionization mass-spectrometry. After liquid–liquid extraction, samples were derivatized with pentafluorobenzyl bromide. MMA was quantified using selected ion monitoring (target ion m/z 233.1) in ratio to deuterium-labelled MMA (target ion m/z 236.1). Calibrations were consistently linear (r > 0.999) up to at least 2000 nmol/L. Interassay variation coefficients of serum pool was 7.8% (283 nmol/L) and of commercial quality control samples were 7.9% (253 nmol/L), 3.4% (464 nmol/L) and 4.3% (866 nmol/L). Recoveries ranged from 87 to 109%. Adult reference values were 90–340 nmol/L and were independent of age and gender (based on 74 apparently healthy subjects).
SPSS version 14.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Analysis was performed on the basis of intention-to-treat. Between-group differences at baseline were tested with Mann-Whitney U tests at P < 0.05. Multiple linear regression analysis was applied to analyse between-group differences at weeks –8, 0 and 12 and changes from weeks –8 to 0, weeks 0 to 12 and weeks –8 to 12. OC use was added as a variable to these models to investigate the effect of OC use on folate kinetics. P < 0.05 was considered significant.
Results
Thirty-two women were eligible to participate. Two participants withdrew because of problematic blood sampling or personal reasons. Three women did not meet the inclusion criteria. The final study group consisted of 27 women (13 intervention, 14 control). Four participants in the intervention group took all tablets, seven forgot up to three tablets and two forgot eight tablets in the supplementation period. Baseline values are presented in Table 1. With the exception of a significantly lower Hb in the intervention group (P = 0.022), there were no significant between-group differences at baseline. No participants had folate or vitamin B6 deficiency based on local reference values. All participants also had normal vitamin B12 status based on serum MMA, although two participants (1 in each group) had low serum vitamin B12. One subject (intervention group) had a normocytic anaemia at baseline (Hb 7.3 mmol/L, MCV 89 fL). Her Hb increased from weeks –8 to –4 to 7.8 mmol/L. It is uncertain whether this is due to increased FA intake, since she had a high-normal plasma folate (19.0 nmol/L) and normal erythrocyte folate (557 nmol/L) at baseline, and used a low-dose FA supplement (100 μg/d) prior to and during the study period. Because this was no exclusion criterion, her data were used in the intention-to-treat statistical analysis. The significantly lower Hb in the intervention group was not due to mild FA deficiency, since Hb was also lower (P = 0.022) compared with the control group after eight weeks of FA supplementation (week 0). There were no significant changes in Hb and MCV from weeks –8 to 0 and from weeks 0 to 12 in the intervention group relative to the control group.
Study group characteristics
Data represent medians (ranges). No significant differences existed between the intervention and the control groups (Mann-Whitney U test)
Figure 1 illustrates the effect of FA supplementation and discontinuation on folate status. Compared with the control group, serum and erythrocyte folate significantly increased from weeks –8 to 0 and decreased from weeks 0 to 12. Plasma tHcy decreased from weeks –8 to 0 and increased from weeks 0 to 12. Serum folate and plasma tHcy changes from weeks –8 to 12 and concentrations at week 12 were not significantly different from the control group. On the other hand, erythrocyte folate significantly increased from weeks –8 to 12 and remained significantly higher at week 12 compared with the control group. OC use had no significant effect on serum folate, RBC folate and plasma tHcy concentrations and changes as controlled for the control group.
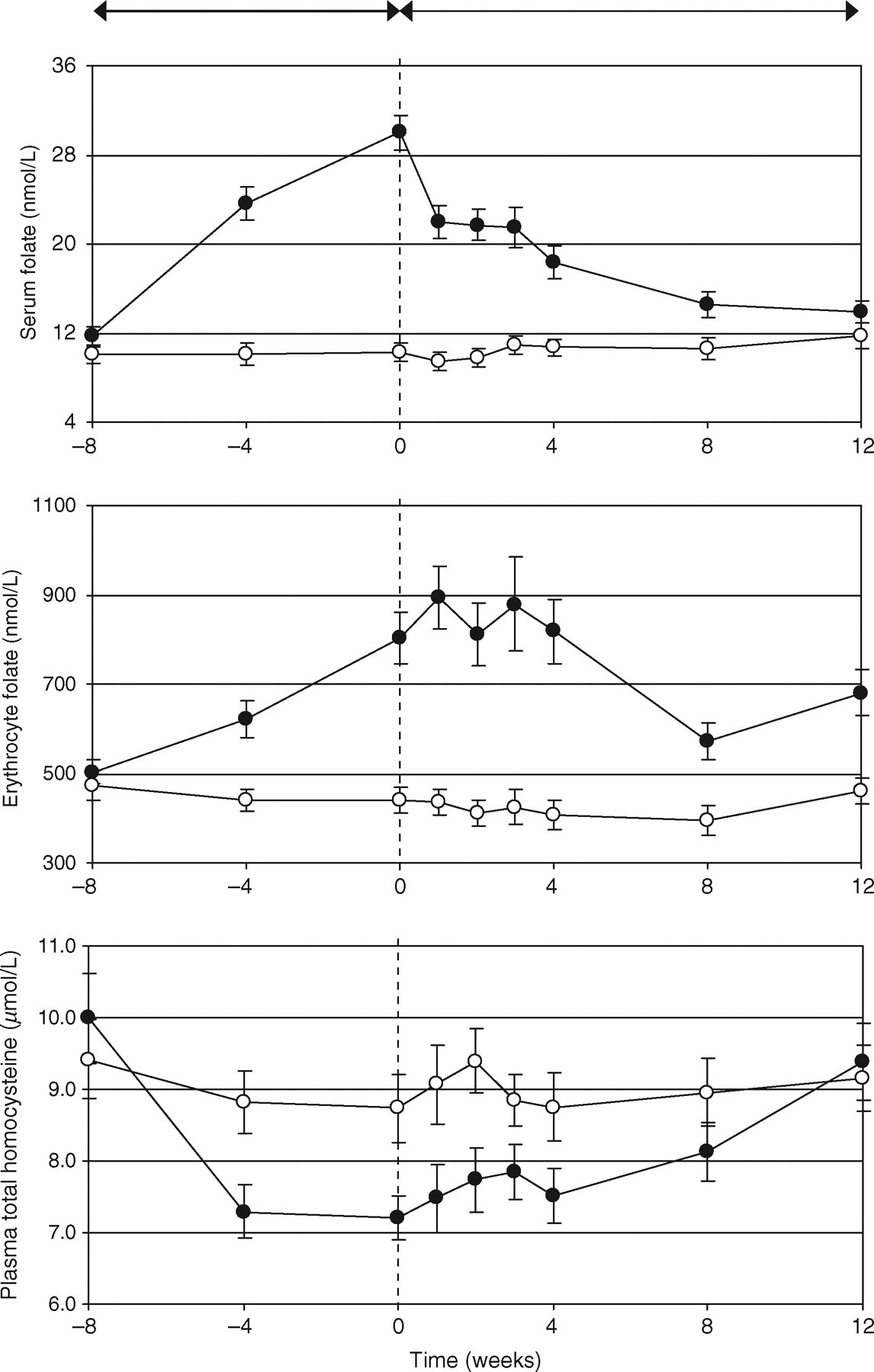
Influence of 500 µg/day folic acid supplementation (8 weeks) and discontinuation (12 weeks) on serum and erythrocyte folate and plasma total homocysteine of 27 healthy premenopausal women. The lines represent means ± standard error of the mean
Discussion
An FA/OC combination pill may effectively reduce NTD risk for newborns of women who become pregnant during OC use, but it is questionable whether these will reduce the risk for babies born to women who stop using OC and become pregnant months later. Serum folate and plasma tHcy, not erythrocyte folate, returned to baseline after 12 weeks discontinuation.
In two studies, folate status remained above baseline levels after 7–8 weeks ≥500 μg/d FA cessation. 11,12 Folate status in our study also remained elevated after eight weeks discontinuation. A significantly higher serum folate (32%, compared with placebo) and lower tHcy (3.7%) was found in another study 12 weeks after cessation of 12 weeks 400–600 μg/d FA in patients with ischaemic heart disease. 13 We also found higher serum folate (3.7%, compared with controls) and lower plasma tHcy (6.1%), but levels were not significantly different from baseline. Ten weeks discontinuation of 100–400 μg/d FA also returned serum folate to presupplementation levels in men. 14 These results altogether suggest that serum folate and plasma tHcy after 12 weeks cessation approach presupplementation status, which is considered suboptimal for the prevention of NTDs. 1
An important limitation of our study is the short supplementation period of eight weeks. An 8–12-week period is sufficient to cause serum folate and plasma tHcy to reach steady-state concentrations. 15,16 It is, on the other hand, certain that erythrocyte folate did not reach steady state, since others showed that steady state was not even reached in 17–24 weeks. 12,15 It is therefore unknown whether our results can be applied to women who use FA for much longer periods. This question depends on the accuracy of erythrocyte folate to reflect folate storage pools. Folate is incorporated in the erythrocyte during erythropoiesis in bone marrow and most likely not in mature erythrocytes. It therefore depends on erythrocyte half-life. Erythrocyte folate reflects folate storage pools up to a certain extent as reflected by a correlation coefficient of 0.47 (P < 0.0001). 17 Daly et al. 18 were the first to show that women with erythrocyte folate more than 906 nmol/L had the lowest risk of NTDs. Pietzrik et al. 19 showed that long-term intake of 400 μg FA per day increases erythrocyte folate well above this cut-off level. They, however, also calculated that after reaching steady-state conditions on this dose, merely eight weeks are necessary for erythrocyte folate to drop below the cut-off level. 19 In at least 50% of all pregnancies, conception does not take place within the first three months after the cessation of OC use 20 and FA is to be taken during the first eight weeks of pregnancy. Most women may therefore not be protected for giving birth to a child with an NTD when they stop taking OC/FA combination pills. The use of FA in combination with OC in a single pill does not invalidate this suggestion, since we and others found that OC use does not affect baseline folate status 21–25 and folate kinetics (this study).
There are unfortunately no studies relating plasma tHcy to risk of NTDs. Erythrocyte folate is considered to be the best parameter of folate stores. Plasma tHcy, on the other hand, is mainly dependent on intracellular folate status and may be a more functional marker of folate status than serum or erythrocyte folate. In the study of Gregory III et al., 26 plasma tHcy, but not erythrocyte folate, correlated to estimated folate storage pools. The recommended dose of 400–500 μg/d FA not only increases erythrocyte folate above the recommended level of 906 nmol/L, but also effectively reduces plasma tHcy concentrations. The relation between NTD and tHcy may therefore be as significant as the relation with erythrocyte folate. The fast increase in plasma tHcy after FA discontinuation may thereby represent an unfavourable situation. It may not be a good suggestion to rely on erythrocyte folate concentrations only.
In conclusion, addition of FA to OC pills seems to be of value for only a minor portion of women wanting to become pregnant, but may be helpful for those who become pregnant during OC use or shortly after its use. It is important to maintain stimulating women of child-bearing age, who want to become pregnant, to take an FA supplement daily.
Footnotes
ACKNOWLEDGEMENTS
We gratefully acknowledge the staff of the HPLC laboratory of our hospital for the vitamin B6 and MMA analysis. We thank the staff of the immunochemical laboratory of our hospital for the folate and vitamin B12 analyses. We also thank Pim Modderman for assistance with the plasma tHcy analyses.