
Abstract
Abstract
Background
The polyethylene glycol (PEG) precipitation test is widely used to detect hyperprolactinaemia caused by macroprolactin. We report two cases of hyperprolactinaemia in which a low recovery of serum prolactin (PRL) after PEG precipitation indicated the presence of macroprolactin, but no macroprolactin was detected by gel filtration chromatography (GFC). Both cases had elevated concentrations of serum globulin (IgG myeloma and polyclonal hypergammaglobulinaemia due to human immunodeficiency virus [HIV] infection), which prompted us to investigate further the effect of serum globulin on the specificity of the PEG precipitation procedure.
Methods
The effect of increasing concentrations of gamma globulin on the precipitation of PRL by PEG was studied by adding purified human gamma globulin to serum. Ten samples from HIV-infected patients, which showed a low recovery of PRL after PEG precipitation (<60%) were studied with GFC.
Results
Addition of gamma globulin decreased the recovery of PRL following precipitation with PEG and gamma globulin concentrations correlated inversely with PRL concentrations (r = 0.9429, P < 0.0167) and percentage recovery of PRL (r = −1.000, P < 0.005). Only one out of 10 samples from HIV-infected patients with PRL recoveries of <60% following PEG precipitation showed a substantial macroprolactin component on GFC.
Conclusions
Monomeric PRL is co-precipitated with serum globulins by PEG. Increased serum globulin concentrations can increase the amount of monomeric PRL precipitated by PEG giving a false estimate of the monomeric PRL and the erroneous impression that macroprolactin is present. The results of the PEG precipitation test should be interpreted with caution in patients with elevated serum globulin concentrations.
Introduction
Prolactin (PRL) circulates in several molecular forms, predominantly monomeric PRL (molecular weight [MW] 23 kDa) with smaller, but variable amounts of big PRL (MW 50–60 kDa) and big-big or macroprolactin (MW 150–170 kDa). 1,2 Macroprolactin and big PRL are of little clinical significance as they are not biologically active. 1,2 Macroprolactin, however, cross-reacts variably in PRL immunoassays and may be the predominant form of circulating immunoreactive PRL, accounting for up to 25% of cases of hyperprolactinaemia. 1–3 Detection of macroprolactin is, therefore, important to avoid erroneous diagnosis, investigation and treatment. 3,4
Precipitation with polyethylene glycol (PEG) is widely used to detect the presence of macroprolactin in hyperprolactinaemic samples. 1–4 Recovery of PRL of >60% after precipitation with PEG 6000 indicates that macroprolactin is not present in significant amounts. When recovery is ≤60%, macroprolactin may be present and the lower the recovery the more certain this is, with recoveries <40% typically consistent with the presence of substantial quantities of macroprolactin. 5 Gel filtration chromatography (GFC) is regarded as the reference technique and this may be used to investigate cases where the recovery post-PEG is close to the cut-off. 1
Samples from subjects infected with human immunodeficiency virus (HIV) have been reported to show low recovery of serum PRL following PEG precipitation when compared with control samples, and this has been interpreted as being a result of macroprolactin contributing to the circulating PRL in these individuals. 6
We report two cases of hyperprolactinaemia with false-positive (<40% PRL recovery) PEG precipitation tests, which prompted us to investigate the specificity of the PEG precipitation procedure and to re-evaluate the contribution of macroprolactin to circulating PRL in patients with HIV.
Case reports
Case 1
A 66-year-old man with an IgG myeloma (serum IgG paraprotein concentration 56 g/L) was found to have a serum PRL of 1941 mIU/L (Roche Elecsys I assay; Roche Diagnostics, Mannheim, Germany) during investigation for left-sided gynaecomastia. Other simultaneously requested relevant investigations, including serum testosterone, α-fetoprotein, β-human chorionic gonadotropin, oestradiol and thyroid function tests were all within normal limits. Recovery of PRL after PEG precipitation was 46% indicating that macroprolactin might be present together with modestly increased monomeric PRL (893 mIU/L).
Further investigations with the Wallac DELFIA assay (Perkin Elmer Inc, Waltham, MA, USA) confirmed the elevated total PRL (1520 mIU/L) and low recovery of PRL after PEG precipitation (37%), but no macroprolactin was detected by GFC. Subsequent questioning revealed that the patient was taking domperidone, a dopamine antagonist, which probably explained his high monomeric PRL.
Case 2
A 30-year-old woman was investigated for secondary amenorrhoea by her general practitioner and found to have a serum PRL of 660 mIU/L (Roche Elecsys I assay). Serum concentrations of luteinizing hormone, follicle-stimulating hormone and thyroid-stimulating hormone (TSH) were all normal. Further investigation of the elevated PRL concentration using the DELFIA assay showed total PRL 498 mIU/L and 39% recovery after PEG precipitation. Although this finding is consistent with the presence of macroprolactin, none was detected by GFC. Serum total protein was 100 g/L, albumin 38 g/L and calculated gammaglobulin was 62 g/L. Protein electrophoresis showed a polyclonal increase in the gammaglobulin fraction. The patient was subsequently found to be infected with HIV.
These two cases prompted us to investigate the effect of hypergammaglobulinaemia on the PEG precipitation test for the detection of macroprolactin and the specificity of the test in patients with HIV infection.
It should be noted that the Roche Elecsys I PRL assay used in the initial investigation of the cases presented above is now no longer available and has been replaced by an assay with lower immunoreactivity towards most forms of macroprolactin. 7
Materials and methods
Effects of serum globulin on the precipitation of prolactin by poleythylene glycol
We prepared a pool of serum with elevated monomeric PRL concentration (pool 1). We added human gammaglobulin (Sigma, Cohn fraction II and III; Sigma-Aldrich, St Louis, MO, USA) to part of pool 1 to give a pool with elevations of both PRL and gammaglobulin concentrations (pool 2). Pools 1 and 2 were then combined in varying proportions to give a series of samples with elevated PRL concentration (1210–1330 mIU/L) and varying gammaglobulin concentration (26–91 g/L). Serum PRL before and after PEG precipitation was determined with the Wallac DELFIA assay.
Macroprolactin in patients with human immunodeficiency virus infection
Samples from 10 HIV-positive subjects (5 women; median age 29.0 years, range 22–41, 5 men; median age 37.0 years, range 23–49) with <60% PRL recovery following PEG precipitation (median recovery 48.0%, range 25–57) were investigated by GFC. The median serum globulin concentration in these samples was 42.0 g/L, range 32–65 (Table 1). These samples were selected from those in a previous study 6 to provide a range of serum globulin concentrations and relatively low PRL recovery after PEG precipitation.
Details of patients with human immunodeficiency virus infection and low recovery of prolactin (PRL) after polyethylene glycol (PEG) precipitation
*GFC (gel filtration chromatography) pattern A, monomeric PRL only detected
†GFC pattern A/B, monomeric and big PRL detected
Analytical methods
Recovery of serum PRL after PEG precipitation in the series of HIV-positive patients was determined using the Architect PRL assay (Abbott Laboratories, Diagnostics Division, IL, USA). Inter-assay and intra-assay coefficients of variation for serum PRL were 4.7 and 3.8%, respectively.
Serum albumin and total protein were measured using the bromocresol green (BCG) dye binding and biuret methods, respectively, on the Roche Modular automated analyser (Roche Diagnostics). Inter-assay and intra-assay coefficients of variation for serum albumin were 0.4 and 1.71% and for serum total protein were 0.6 and 1.0%, respectively. Serum globulin concentration was calculated as the difference between the serum concentrations of total protein and albumin.
Poleythylene glycol precipitation test
PRL was measured in serum samples before and after precipitation with PEG molecular weight 6000 as described previously.
7
Briefly, 200 μL of PEG 6000 solution, 250 g/L in water, was mixed with an equal volume of sample and incubated at room temperature for 10 min. The suspension was then centrifuged at 3000
Gel filtration chromatography
GFC of serum PRL was performed on a 40 × 1.6 cm column of Sephacryl™ S 300 (Pharmacia , GE Healthcare Ltd, Little Chalfont, UK) as described previously. 8 Varying volumes of serum were applied to the column, dependent on the total serum PRL concentration and eluted with 10 mmol/L Tris buffered saline. Fractions of approximately 1.4 mL were collected and assayed for PRL using the Wallac DELFIA assay and for albumin using a BCG technique on the Roche Modular analyser. Albumin was used as a marker of molecular mass and to monitor the performance of the chromatography.
Statistical analysis
Data are expressed as medians with ranges. Spearman rank correlation was used to evaluate the significance of association between variables.
Results
In the samples with added gammaglobulin, increasing gammaglobulin concentrations correlated inversely with PRL concentrations (r = −0.9429, P = 0.0167) and percentage PRL recovery (r = −1.000, P < 0.005) following precipitation with PEG 6000 (Figure 1).
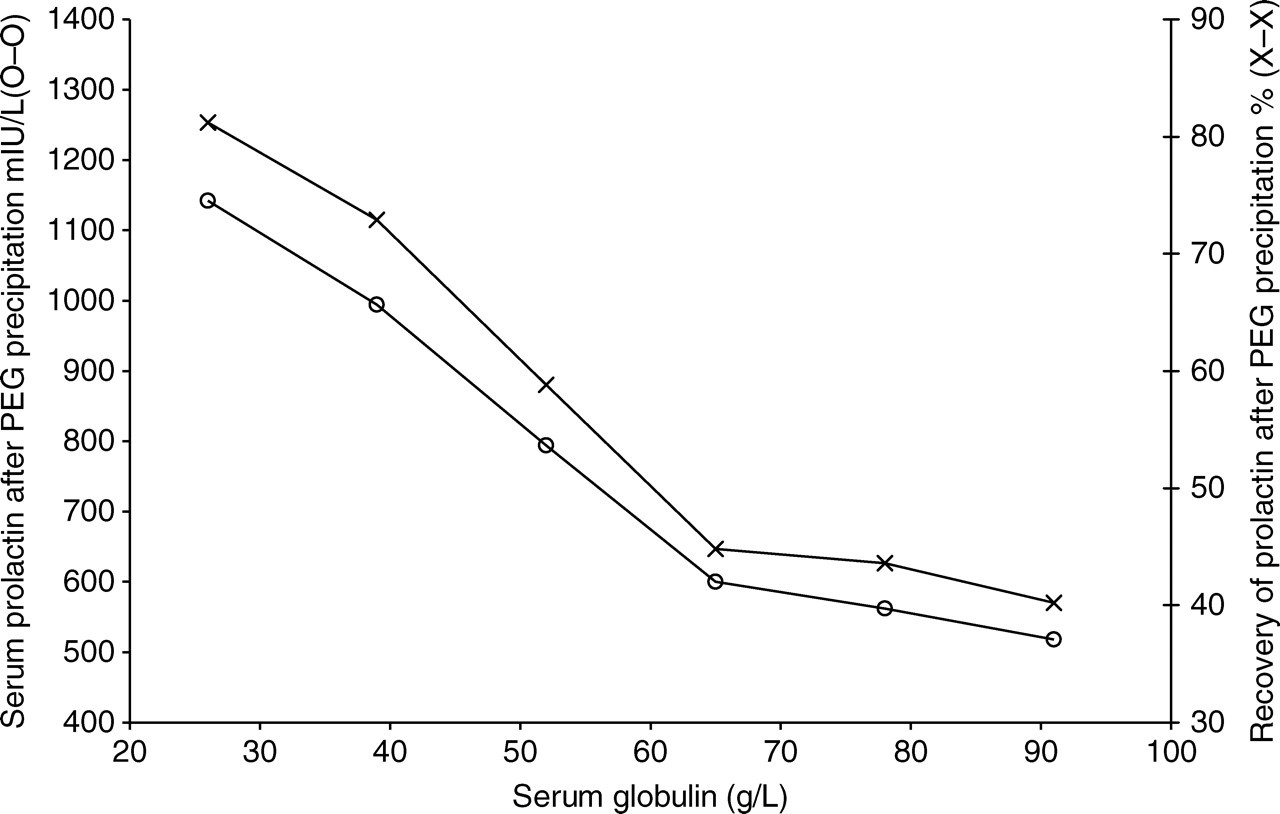
Effect of added gammaglobulin on precipitation of prolactin from serum by polyethylene glycol (PEG)
In the 10 patients with HIV infection, only one instance of macroprolactinaemia was identified following GFC (case 10). In this case, the macroprolactin contributed 66% of the total serum PRL immunoreactivity in the DELFIA assay (Table 1). This case also showed the lowest recovery of PRL after PEG precipitation (25%) compared with the other samples in the series. A much lower proportion of macroprolactin (10–25%) was detected in three further samples that showed relatively low recovery of PRL after PEG precipitation (cases 6, 8 and 9). In the remaining six patients, samples were shown to contain only monomeric PRL or monomeric PRL together with big PRL.
In the eight cases with elevated globulin concentrations (>38 g/L), there was no correlation between percentage PRL recovery and serum globulin concentration (r = 0.09639, P = 0.8401), but among the cases without macroprolactin the two cases (5 and 7) with the highest globulin showed the lowest recovery after PEG precipitation (Figure 2).
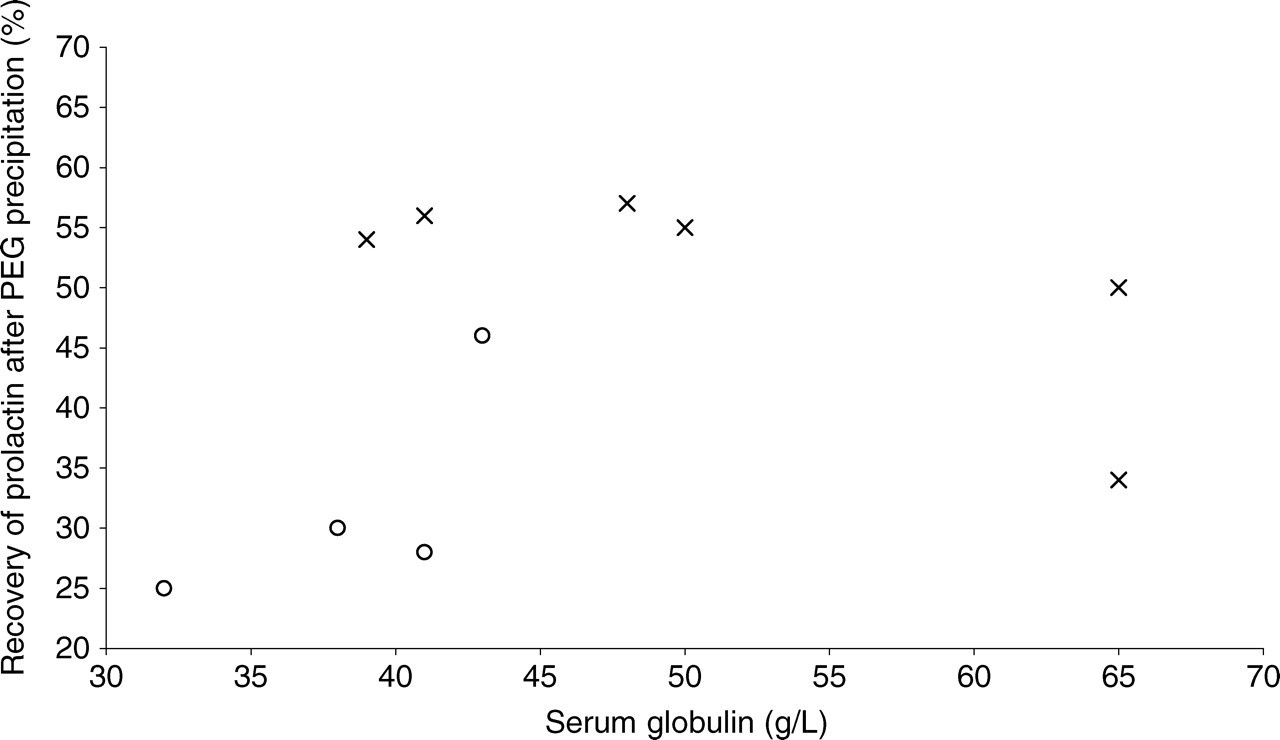
Correlation of recovery of prolactin after polyethylene glycol (PEG) precipitation and serum globulin in patients with human immunodeficiency virus infection. Patients with macroprolactin on gel filtration chromatography (GFC) (O) and no macroprolactin on GFC (X)
Discussion
Routine screening of hyperprolactinaemic serum to detect macroprolactin is recommended 1,2,4 because macroprolactinaemia is a relatively common cause of erroneous diagnosis and inappropriate treatment in patients with hyperprolactinaemia. 3 The PEG precipitation test has been advocated as the best approach for the detection of macroprolactin 9 and has been widely adopted for this purpose. The test is commonly interpreted after calculation of percentage recovery of PRL. This approach has been justly criticized by Suliman et al. 3 because it may fail to distinguish macroprolactinaemia (in which the elevated total serum PRL is due to macroprolactin and the concentration of monomeric PRL, which is bioactive in vivo, is normal) from the situation in which elevated monomeric PRL concentration coexists with the presence of macroprolactin, which contributes to the elevated total PRL, but is not the sole cause of it. It has been suggested that the proper focus of laboratories seeking to obviate the problem of macroprolactinaemia should be the determination of monomeric PRL and Suliman et al. 3 proposed that the PRL result obtained after PEG precipitation be used as a measure of monomeric PRL and referred to a reference interval determined by PEG precipitation in a normal population. We accept that this is the best approach to take, but since reference intervals for PRL after PEG precipitation are not available for the majority of immunoassays for PRL, we have included calculation of recovery in this paper, as this method still remains widely used.
It has been clearly shown that the PEG precipitation test is not specific for the removal of macroprolactin but also precipitates big PRL and a proportion (approximately 20%) of monomeric PRL. 9 The non-specific nature of PEG precipitation is a major limitation of the technique which is considered in detail elsewhere in this journal. 10 Our findings indicate that monomeric PRL is co-precipitated with gammaglobulins by PEG and this is a contributing factor to the observed non-specificity of PEG precipitation. The amount of PRL precipitated is related to the serum globulin concentration and high serum globulin concentrations, as in the cases presented here, may thus cause low recovery of PRL after PEG precipitation and lead to the erroneous interpretation that macroprolactin is present. Furthermore, if the results of PEG precipitation are interpreted as recommended by Suliman et al., 3 high serum globulin concentrations may lead to a falsely low estimate of the monomeric PRL concentration.
In the series of patients with HIV infection, macroprolactin was identified as the cause of low recovery of PRL after PEG in one case and as a likely contribution to low recovery in three other cases (6, 8 and 9). In contrast to our findings in the experiment with added gammaglobulin, we found no correlation between recovery of PRL after PEG precipitation and serum globulin in the patients with HIV infection and elevated gammaglobulin. This may be because any effect of gammaglobulin concentration on recovery of PRL after PEG precipitation in these patients was obscured by the influence of other factors, such as the presence of small amounts of big PRL and/or macroprolactin, or because the range of PRL and gammaglobulin concentrations was relatively narrow. Nevertheless, in cases 5 and 7 it seems probable that the particularly high serum globulin concentrations contributed to or caused the low recovery of PRL after PEG precipitation. Previous studies have reported low PRL recovery in samples from HIV patients and this has been interpreted as indicating an increased prevalence of macroprolactinaemia in HIV infection. 6 These results may have been influenced by elevated serum globulin concentrations typical of HIV infection and may therefore require re-evaluation.
In summary, the PEG precipitation test for macroprolactin is non-specific. False-positive results may occur in serum samples containing elevated globulin concentrations and estimates of monomeric PRL in these samples may be falsely low. In samples containing elevated serum globulin concentrations, the results of the PEG precipitation test should be interpreted with caution and consideration should be given to using GFC to investigate the presence of macroprolactinaemia and to determine the concentration of monomeric PRL.