
Abstract
Abstract
Background
Pre-analytical problems causing pseudohyperkalaemia have been highlighted previously. These include transit time and temperature effects when sample collection points are geographically widely spread. Similarly, inappropriate phlebotomy technique (in particular, requesting patients to fist clench to facilitate venesection) is a documented cause of pseudohyperkalaemia, but its incidence may be impossible to establish. This study illustrates how primary care population serum potassium data altered when local phlebotomy clinics optimized their technique.
Methods
The effect of improving phlebotomy was studied by plotting average monthly primary care population serum potassium data and average percentage of samples with hyperkalaemia (5.2 mmol/L or higher) against mean monthly temperature before and after changes in phlebotomy practice. Only samples from primary care were included between 2002 and 2005 inclusive.
Results
Primary care population serum potassium was inversely related to ambient temperature. Following the change in phlebotomy practice, the annual percentage of results above reference range (5.2 mmol/L or higher) was reduced from 9% to 6% and the number of results breaching the upper telephoning threshold (5.8 mmol/L or higher) fell from 0.9% to 0.5%.
Conclusions
Ensuring that phlebotomists were trained to avoid facilitating venesection by requesting patients to hand grip (fist clench), was associated with lower mean serum potassium results for the primary care patient population and a reduced incidence of hyperkalaemia. It is likely that the contribution of patient fist clenching during phlebotomy to pseudohyperkalaemia has been underestimated.
Introduction
Increasing numbers of queries to our department regarding unexpectedly high serum potassium results (despite satisfactory analytical quality assurance) prompted us to investigate pre-analytical handling of samples for primary care. Pseudohyperkalaemia due to intracellular potassium leakage caused by low ambient temperature and prolonged transit time is well documented 1,2 but five patients had persistent apparent pseudohyperkalaemia despite prompt sample analysis. When re-bled in the pathology department all five had to be asked to refrain from hand gripping and normal potassium results were then obtained. Potassium released from myocytes into extracellular fluid during muscle contraction contributes to pseudohyperkalaemia. 3
The possibility that patient fist clenching during phlebotomy would be sufficiently common to significantly affect population serum potassium data has not previously been considered.
Most ambulant patients in primary care in the Bromley area attend one of three outpatient phlebotomy clinics. Of these one is on the main hospital site where the pathology department is situated. The other two are at smaller hospitals within five miles of the main site. Numbers attending are divided evenly among these clinics and regular transport between sites avoids major delays, most samples arriving within 1 hour. Only for non-ambulant patients are delays common when home visits are needed.
Methods
Discussions with senior nursing staff responsible for the phlebotomy clinics took place at the end of August 2003. Literature describing the effect of fist clenching 3 was provided and an agreement that phlebotomists would receive appropriate training was reached. The potassium data up to and including the first month in which the changes began to be implemented (September 2003) were compared with subsequent data. Potassium was measured using Ortho Vitros dry slide methodology up to mid-March 2003 then Bayer Advia 1650 analysers thereafter. Agreement between the two methods was excellent for patient samples.
Retrospective review
Mean monthly serum potassium concentrations were calculated for all general practitioner (GP) requested analyses between January 2002 and December 2005 (n = 228,523). No hospital inpatient or outpatient samples were included. The percentage of results above the reference range (3.5–5.1 mmol/L), that is results of 5.2 mmol/L or higher was calculated on a calendar monthly basis. The percentage breaching our upper telephoning threshold (5.8 mmol/L or higher) was also calculated. These results were plotted against the mean monthly temperature for South East England as published by the Meteorological Office website. Analysis of the data was carried out using Analyse-It for Excel (Leeds, UK). Regressions were compared using Student's t-test.
The calculations included only the reported results. Results for samples showing evidence of contamination (e.g. chelating agents) or those withheld due to high platelet counts, 4 haemolysis or not being received on the day obtained were excluded.
Results
When mean calendar monthly potassium results for GP patients were plotted against mean temperature for the month, there was clearly an inverse relationship (Figure 1). The curves shown before and after the changes in phlebotomy practice are significantly different (P < 0.01) and the intercept is significantly lower following implementation of the change (P < 0.001) with a much closer correlation between potassium and temperature. Figure 2 shows linear regression between mean monthly temperature and percentage of potassium results above the reference range (3.5–5.1 mmol/L) before and after changing phlebotomy practice. Again the regressions are significantly different with a shallower slope (P < 0.05) and considerably lower intercept (P < 0.001) following implementation of the changes. In the latter period, the large fluctuations have settled and the percentage of samples showing hyperkalaemia is consistently below 9%. The switch from Ortho Vitros dry slide chemistry to Bayer wet chemistry was not associated with any significant change to the slope or intercept (Student's t-test) when mean monthly serum potassium versus temperature regressions were compared prior to phlebotomy changes. This data has therefore been combined in the figures. When the regressions using either the Ortho Vitros or Bayer method individually or as pooled data prior to phlebotomy improvement were compared with that obtained after implementing phlebotomy changes, significant changes in the intercept were observed. The alteration in regression is therefore associated with phlebotomy improvement not methodology.
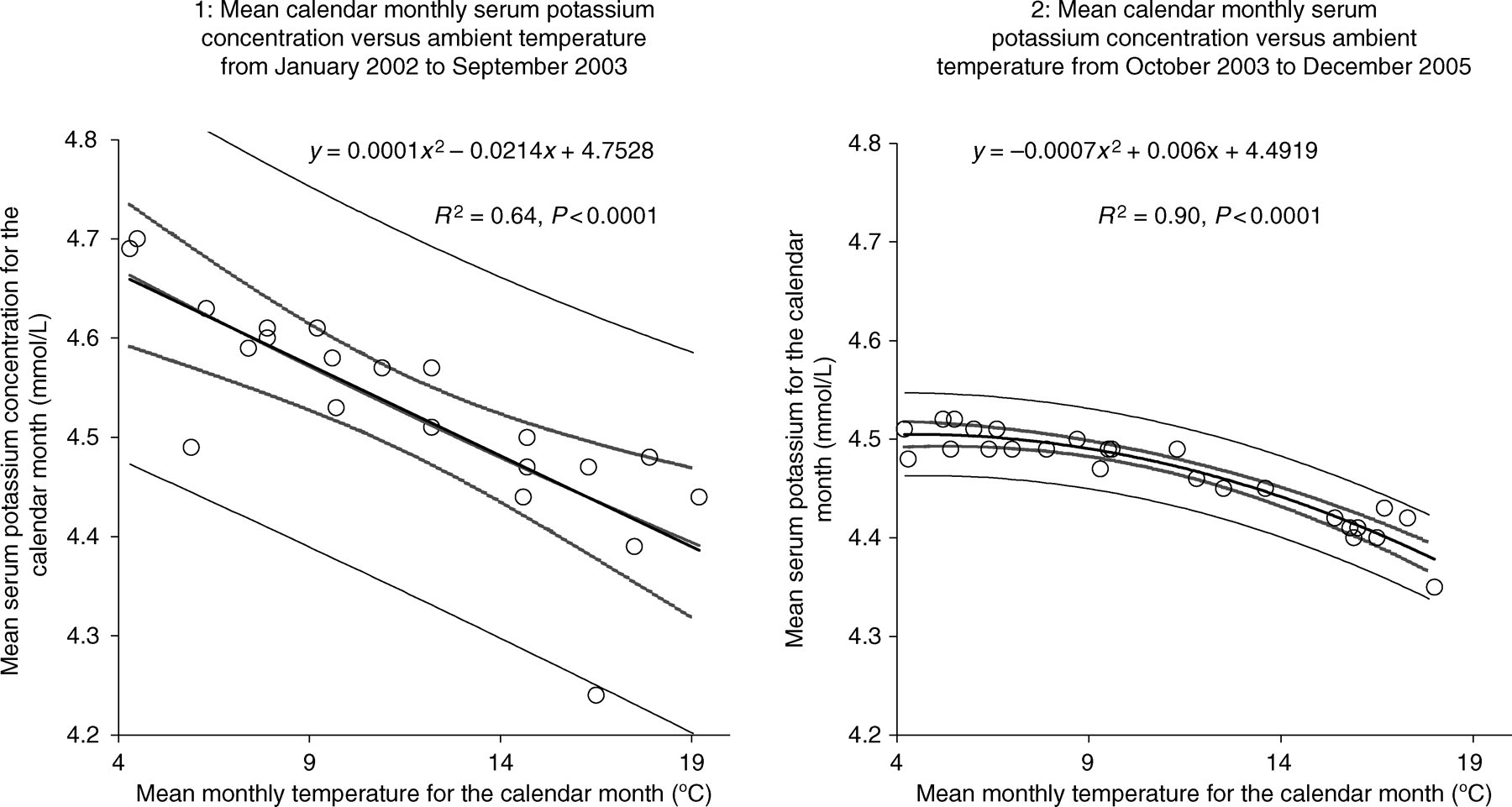
Effect of changing phlebotomy practice on average serum potassium concentration for patients in primary care at varying transport (ambient) temperatures. Chart 1: January 2002 to September 2003 (prior to change in phlebotomy practice). Chart 2: October 2003 to December 2005 (following change in phlebotomy practice)
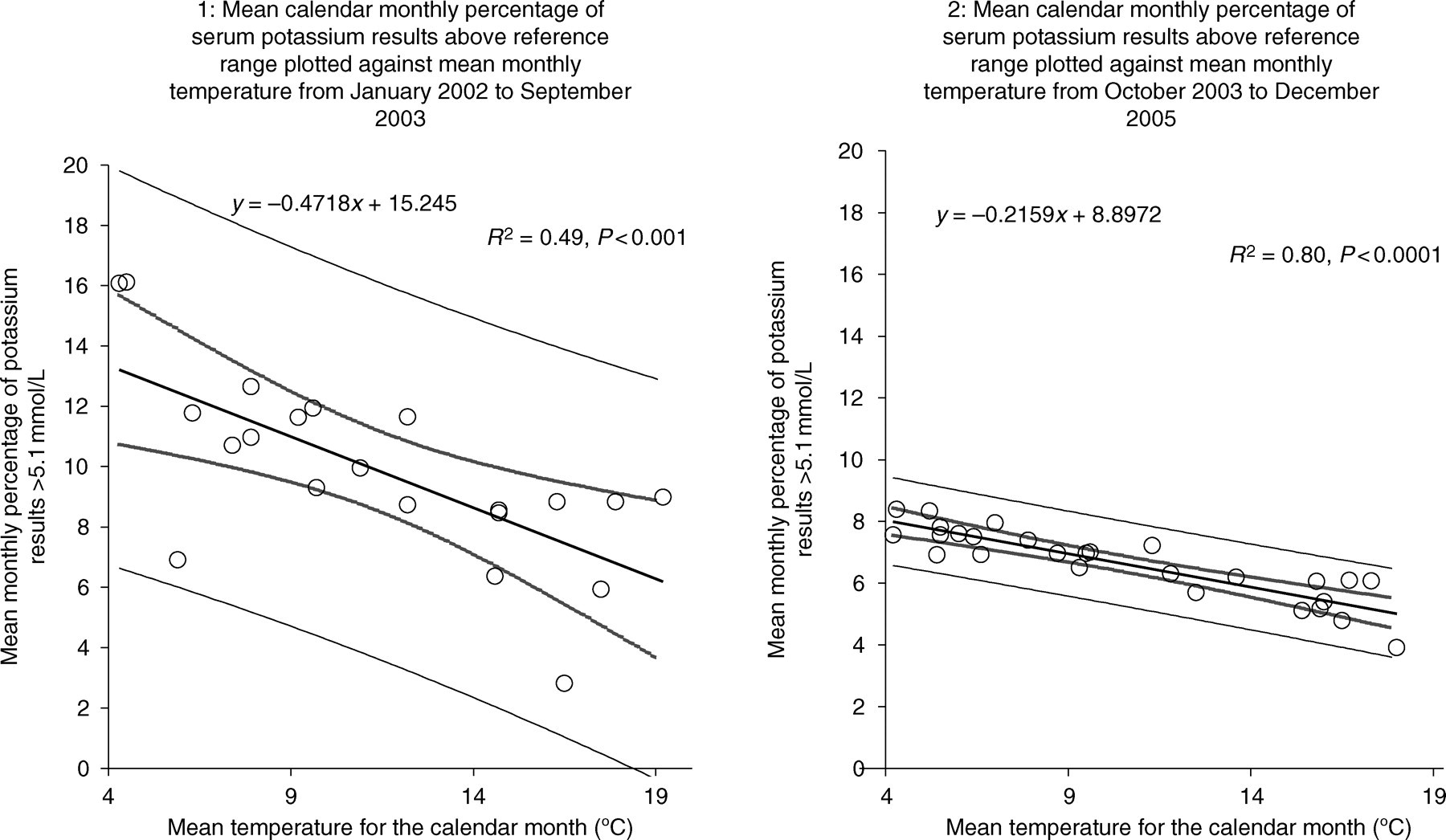
Effect of changing phlebotomy practice (no fist clenching) on the percentage of cases of hyperkalaemia at varying transport (ambient) temperatures. Chart 1: Before change in phlebotomy practice. Chart 2: After change in practice
When the percentage of results breaching our telephoning threshold (5.8 mmol/L or higher) was plotted, the statistical significance of the relationship with ambient temperature was lost. This suggested that although low ambient temperature does increase serum potassium concentration, the increase is modest (unless sample receipt is delayed) and would not alone explain cases of spurious potassium results (pseudohyperkalaemia).
Discussion
Following implementation of improved phlebotomy practice, the incidence of hyperkalaemia fell from approximately 13% to 8% during the coolest weather and from approximately 6% to 4.5% during the hottest. The incidence of hyperkalaemia had always been lower in summer. The authors' personal experience is that venesection for some ‘difficult to bleed’ individuals is facilitated by higher temperatures, as their veins become visible. It is possible that temperature-associated changes in population serum potassium are multi-factorial, related to both in vitro leakage and frequency of problematic venesection.
Mean monthly serum potassium values decreased slightly following changed practice, but remained temperature correlated (r 2 = 0.90). This correlation compares well with another study, 1 which obtained figures equating to an r 2 value of 0.84.
The annual percentage of results breaching the upper telephoning threshold has fallen by almost half (from approximately 0.9% to 0.5%). The incidence of reported hyperkalaemia for primary care patients has fallen from an annual rate of approximately 9% to 6%. Other workers observed seasonal variation in the incidence of hyperkalaemia ranging between 5% and 17% for patients in primary care. 1 This study suggests that when more than 9% of results are above the reference range, the possibility of a pre-analytical problem should be considered. Assessing quality within the pre-analytical phase is difficult, 5 but reviewing population data is informative. 6
Conclusion
Although exposure to outdoor ambient temperature in South East England has a significant effect on serum potassium results when blood samples are transported to the laboratory from external collection points, the change in potassium concentration for most patients is likely to be quantitatively small (<0.5 mmol/L), unless sample receipt is also delayed. Suboptimal phlebotomy practice, particularly requesting patients to fist clench to ease venesection, can lead to quantitatively serious overestimation of serum potassium and the percentage of patients with reported hyperkalaemia falls when such practice is corrected.
Footnotes
Acknowledgements
The authors are very grateful to Dr Brian Payne, Leeds for help and advice with statistical analysis and data processing.
This work would not have been possible without co-operation and support from Vanessa Lidsey, Susan Donovan, Clemency Newman and Avril Coffey, senior nursing staff in our phlebotomy outpatient departments.