
Abstract
Abstract
Background
The aim of the study was to determine the extent of bilirubin interference on two different Beckman–Coulter creatinine methods used on the CX5 PRO/DxC 600 and the DxC 800 systems, respectively.
Methods
The Beckman methods were compared with a high-performance liquid chromatography (HPLC) method using 104 patient samples with creatinine concentrations <133 μmol/L and bilirubin concentrations of between 30 and 802 μmol/L.
Results
The linear regression analysis calculations expressing the relationship between bilirubin concentration and the observed difference between the Beckman and HPLC creatinine methods are: DxC800 creatinine M (modular or cup) method: r 2 0.217, slope −0.023 and intercept 6.43; and DxC600 method: r 2 0.7324, slope −0.0882 and intercept 12.01.
Conclusions
There is significantly greater interference by bilirubin on the CX5 PRO/DxC 600 method, which can lead to inaccuracy in the calculation of the estimated glomerular filtration rate by the Modification of Diet in Renal Disease equation.
Introduction
Bilirubin has been shown 1,2 to cause negative interference with Jaffe creatinine methods. Recent studies 3,4 (including one within our own organization) have shown the Roche Modular method to have a small negative bias across all creatinine concentrations, irrespective of the bilirubin concentration when compared with chromatography methods. Our organization (consisting of 33 laboratories in total) is currently in the process of converting our general chemistry analysers from Roche (Hitachi 917, Hitachi Modular and Integra) chemistry analysers to Beckman (CX5 PRO, DxC 600 and DxC 800) platforms. We therefore undertook a comprehensive evaluation of the extent of bilirubin interference on creatinine estimations, as it is not uncommon to receive specimens from patients with total bilirubin concentration of >1000 μmol/L (e.g. liver transplant candidates or neonates). Beckman literature states that the creatinine method for the CX5 PRO and DxC 600 systems has no significant interference by bilirubin concentrations up to 256 μmol/L, and that at a bilirubin concentration of 385 μmol/L the observed effect is a 44 μmol/L reduction in creatinine concentration. The creatinine M (modular or cup) method on the DxC 800 systems states that there is an underestimation by 18 μmol/L at a bilirubin concentration of 342 μmol/L.
Methods
We used a high-performance liquid chromatography (HPLC) method as the comparative ‘reference’ method to investigate the extent of bilirubin interference on the Beckman assays. The HPLC method is a modification of the Yue-dong method. 5 HPLC analysis was performed on a Waters 2695 Alliance separations module with a 996 Photodiode array detector. The system was controlled and data analysis performed on Empower Enterprise Chromatography software (Waters Corporation). Plasma samples (200 μL) were ultrafiltered using Millipore Microcon 30,000 MWCO filters and 10 μL of the filtrate was injected into a Waters Atlantis 4.6×150 mm column. Patients samples with creatinine concentrations <133 μmol/L and total bilirubin values >20 μmol/L were randomly selected from routine specimens, which were assayed on the Roche Modular D-analyser. The cut-off value of <133 μmol/L for creatinine was used as it is the relevant range recommended for detecting chronic kidney disease by the National Kidney Disease Educational Program (NKDEP) Working Group. 6 In total, 104 lithium heparin plasma samples were evaluated with a range of total bilirubin of between 30 and 802 μmol/L.
Results
Our results confirm that the Beckman creatinine methods show increasing negative bias with bilirubin increase when compared with the HPLC method, even below the bilirubin concentrations stated in the Beckman literature (Passing-Bablok: DxC 600 vs. HPLC y = 1.049x−13.78; DxC 800 vs. HPLC y = 0.929x + 6.00). Linear regression analysis of the actual difference between the Beckman and HPLC methods vs. bilirubin (Figure 1) indicates that with the DxC 800 creatinine M (modular or cup) method there is minimal correlation between bias and bilirubin concentration (r 2 0.217, slope −0.023 and intercept 6.43), indicating that there is no significant interference from bilirubin. In contrast, the CX5 PRO/DxC 600 method shows significant correlation between bias and bilirubin concentration (r 2 0.7324, slope −0.0882 and intercept 12.01).
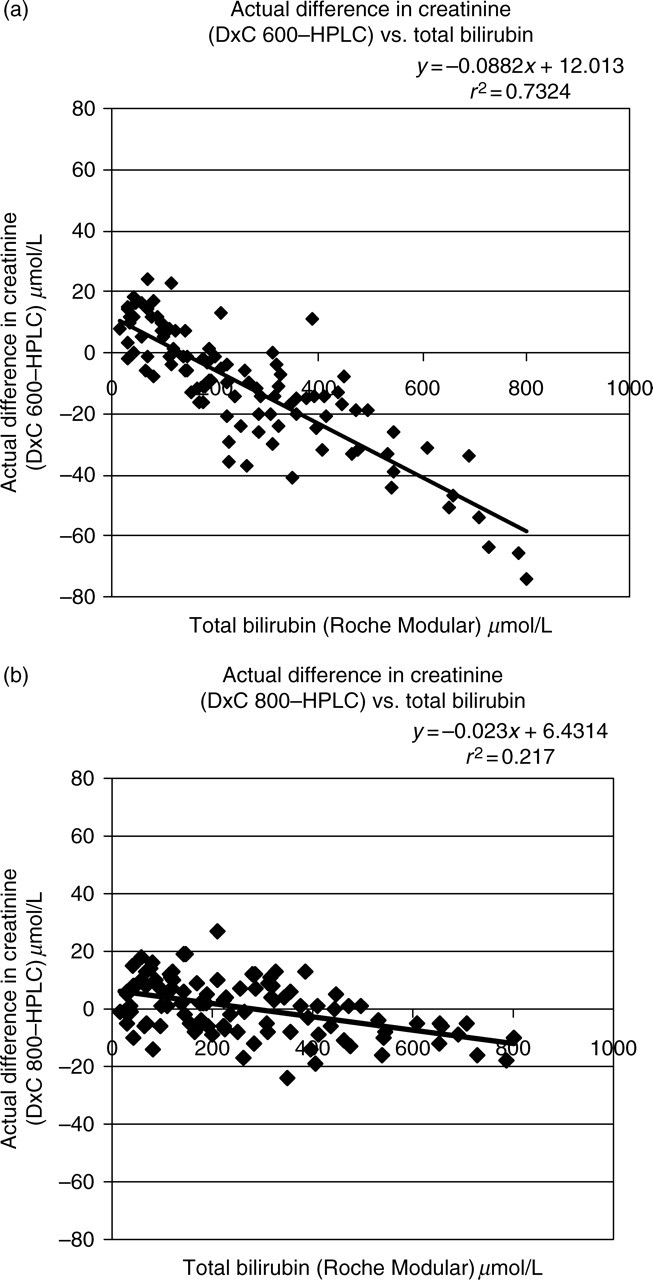
(a) Actual difference in creatinine between Beckman DxC 600 and high-performance liquid chromatography (HPLC) method vs. total bilirubin. (b) Actual difference in creatinine between Beckman DxC 800 and HPLC method vs. total bilirubin
Discussion
As far as we can determine from literature provided by Beckman–Coulter, the reactive ingredients in the two methods are identical. The main differences between the Beckman methods are: (1) incubation temperature −41°C on the DxC 800 and 37°C on the CX5 PRO/DxC 600; and (2) the incubation times for the rate reactions −20.5–26.4 s on the DxC 800 and 16–64 s on the CX5 PRO/DxC 600. The higher incubation temperature could allow interfering substances to complete their reaction in a much shorter time span, before creatinine forms a picrate complex. This could well limit interference caused by biliverdin, an oxidation product of bilirubin formed in the alkaline solution. 2
The derived equations from our data provide a far clearer indication of the bilirubin interference on the two methods than the Beckman literature. This is important within our organization and other laboratories or networks of laboratories that may use the two methods on patient samples interchangeably. The significant negative effect by bilirubin on the CX5 PRO/DxC 600 method furthermore has an impact on the estimated glomerular filtration rate (eGFR) calculated using the Modification of Diet in Renal Disease equation. Falsely decreased creatinine results due to bilirubin interference lead to falsely elevated eGFR results. Thus, use of the eGFR in assessing severity of renal failure in patients with jaundice must be considered in conjunction with the bilirubin concentration. The choices available for laboratories using the CX5 PRO or the DxC 600 method include the use of derived equations such as the ones determined in this study, or alternatively to provide a cautionary note regarding bilirubin's effect on creatinine and eGFR when reporting results from these analysers. Another potentially desirable outcome may be for Beckman–Coulter to standardize on the cup method, re-engineering the CX5 PRO and DxC 600 analysers to accommodate this method.