
Abstract

Introduction
We present the case of a young man with cystic fibrosis (CF) who presented with a massive haemoptysis. All management options were considered and treatment with tranexamic acid was commenced. We discuss the treatment options for patients with CF presenting with massive haemoptysis and the underlying evidence base.
DECLARATIONS
None declared
MH is funded by a Fellowship from the Wellcome Trust
Written informed consent to publication was obtained from the patient or next of kin
HLT
All authors contributed equally
Case report
Our patient is the youngest of two brothers with CF, he also has an older sister and younger half-sister who are both well. He is homozygous for ?F508 after being tested at birth. His early life was complicated by pyloric stenosis which required a Ram-stedt's pyloromyotomy at the age of 1 month. He was also noted to have a degree of pulmonary stenosis and aortic stenosis, neither of which required treatment. By the age of 2.5 years he was established as chronically colonized with Pseudomonas aeruginosa and developed CF-related liver disease by the time he was 6 years old.
At the age of 10 years he was receiving intravenous (IV) antibiotics every four months and by this time his lung function had reduced to FEV1 45% predicted and FVC 61% predicted. With growth his lung function reached the highest level at the age of 12. At the age of 15 years he suffered a portacath infection associated with Candida sp. bacteraemia and the following year isolated multiply-resistant P. aeruginosa.
After an episode of increased cough, he was at home when he experienced a massive haemoptysis. This haemoptysis continued over the following three days with an estimated cumulative blood loss of 400 mL. He was transferred from his local hospital to the regional centre and underwent a CT thoracic angiogram which demonstrated a tortuous and dilated artery entering the right hilum and right lower lobe (the area of most significant bronchiectatic change) (Figure 1). This arose from a vessel that also appeared to pass through some of the intervertebral foraminae. Tranexamic acid was commenced, 1 g orally three times a day. The artery identified as the cause of the haemoptysis was considered amenable to bronchial arterial embolization (BAE), however the haemoptysis resolved and embolization was unnecessary. Tranexamic acid therapy continues currently.

CT angiogram of dilated tortuous bronchial artery (in cross-section) considered to be responsible for haemoptysis. The insert is reproduced with kind permission from the Radiological Society of North America. Yoon W, et al. Bronchial and nonbronchial systemic artery embolization for life-threatening hemoptysis: a comprehensive review. Radiographics 2002;22:1398
This event heralded an increased rate of decline in our patients’ condition (Figure 2). Alongside multiple recent admissions for pulmonary exacerbations, he experienced a decline in lung function demonstrated by a fall in FEV1 from 46% predicted at the age of 16 prior to his haemoptysis to 14% predicted currently. At the age of 15 years his BMI peaked at 17.7 kg/m2 and had begun to reduce prior to his admission with haemoptysis.
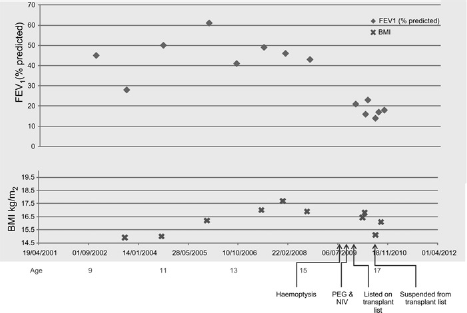
Clinical condition (lung function, FEV1) and BMI over time
At the end of 2009 he was accepted as a candidate for lung transplantation. At this time his deterioration had continued with a FEV1 of 20% predicted, oxygen saturations of 89%, an exercise tolerance of 425 metres, a body mass index of 16.5 kg/m 2 , and a variable adherence to treatment. He has since been maintained on overnight non-invasive ventilation.
In order to optimize nutrition and calorie intake he accepted a gastrostomy (PEG). This initially functioned well, however gradually the use of the PEG became associated with abdominal pain and nausea, despite antiemetics and reduced feed volumes and rates. Troubled by chest pain and breathlessness, which is managed with fentanyl patches, the frequency of his admissions has increased such that he spends 50% of his time in hospital for IV antibiotics. During this time his weight insidiously continued to fall to the point that his BMI fell below 15 kg/m 2 . In this condition it was felt by the transplant team that his candidacy for a transplant should be suspended. After a concerted effort, his decline in weight has reversed and our patient aims to reach a level at which he would once again be a candidate for lung transplantation.
Discussion
Patients with cystic fibrosis account for over 65% of those of all causes who experience haemoptysis in their youth. 1 There are three series in the literature describing major haemoptysis in patients with cystic fibrosis.2–4 Two of these are retrospective case reviews reporting 91 patients2,4 and one registry study reporting data from the Cystic Fibrosis Foundation Registry which detailed 1153 patients 3 who had experienced an episode of haemoptysis. Episodes of haemoptysis are common with 9.1% of patients reporting an episode in the previous 5-year period. 2 In a patient's lifetime, 4.1% will experience an episode of ‘massive hae-moptysis’ 3 – defined as the loss of over 240 mL in a 24-hour period. 5
Older patients with more severe lung disease appear to be most at risk, with the majority having a FEV1 less than 40% predicted. 3 Of children with CF who present with their first bleeding episode, the average agewas15 years (range7–19years) with an average FEV1 predicted of 56% (range 14–98%). The CFF registry study suggested that infection with Staphylococcus aureus and co-morbid diabetes mellitus may also be risk factors whereas treatment with dornase alpha and inhaled tobramycin appeared to be protective. 3
The majority of those who experience an episode of major haemoptysis are older with poorer lung function and following an haemoptysis episode lung function deteriorates significantly. 3 It is therefore difficult to separate cause and effect. Our patient's lung function and clinical condition appeared to have begun to deteriorate prior to his haemoptysis but his lung function declined precipitously thereafter (Figure 2). The CFF Registry study grouped patients according to severity of lung function and found that for all levels of severity, those who experienced an episode of haemoptysis had an excess mortality compared to their peers with CF that had not. They calculated an attributable two-year excess risk for mortality due to haemoptysis between 5.8% and 16.1%. 3
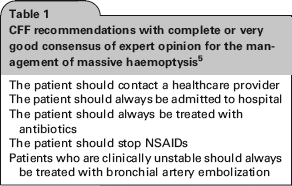
The evidence base supporting the optimal management of those with haemoptysis and CF is weak. Recently published guidelines for the management of haemoptysis in patients with CF depend on expert opinion (Table 1). 5 There appears to be a significant lack of consensus among experts regarding the optimal management strategy for treating haemoptysis, except that all those with massive haemoptysis should be hospitalized. These guidelines also report a reasonable level of consensus in recommending BAE in patients who are clinically unstable and bleeding; and antibiotic treatment is recommended as haemoptysis may be a manifestation of an infective exacerbation. There is also a good degree of consensus recommending that patients with massive haemoptysis should stop non-steroidal anti-inflammatory drugs (NSAIDS), stop bi-level positive airway pressure (BiPAP) for as long as there is bleeding and stop airway clearance therapies. There was some degree of consensus that hypertonic saline should be withheld although they stopped short of making recommendations for other inhaled therapies. They deemed that lung resection should only be considered as a final treatment option. 5
CFF recommendations with complete or very good consensus of expert opinion for the management of massive haemoptysis 5
Tranexamic acid does not feature in the recently published consensus statement from the Cystic Fibrosis Foundation. The evidence base supporting the use of tranexamic acid for treating haemoptysis in patients with CF is limited to single case reports.6,7 Tranexamic acid is a lysine derivative that blocks the lysine binding sites on plasminogen, preventing the plasmin-tPA complex from binding to fibrin, thus inhibiting fibrinolysis. 8 Administration by IV and oral routes result in peak serum levels after one and three hours, respectively. 9 Renal excretion predominates with 90% of an IV and 40% of an oral dose being recovered in the urine after 24 hours. 9 To maintain a therapeutic level 4-hourly dosing is recommended at a level of 10 mg/kg IV and 30–40 mg/kg orally. 9
Recent Cochrane reviews support the use of tranexamic acid in the prevention and treatment of postpartum haemorrhage, 10 the reduction of need for red blood cell transfusions during surgery 11 and the reduction of blood loss during scoliosis surgery in children. 12 Its use however is not supported to prevent blood loss after acute traumatic injury. 13 Tranexamic acid therapy has been more frequently used in pulmonary haemorrhage due to malignancy and the durations of treatment used have been variable. 14 Two cases in the CF literature report the successful treatment of haemoptysis in patients with CF, but also report re-bleeding upon the cessation of therapy.6,7 Just as there is a lack of evidence supporting the administration of tranexamic acid, there is also uncertainty regarding its cessation. In our case tranexamic acid may have contributed to the cessation of bleeding and due to the concern in the literature regarding cessation being associated with recurrence, therapy continues.
The evidence supporting the use of BAE is similarly weak and while there appears to be consensus that it is effective, it is invasive, requires a skilled interventional radiologist and is accompanied by the possibility of severe complications. 15 As a result it is recommended for those who are actively bleeding and unstable. 5 Our patient was considered to be a candidate for embolization on the basis that an embolizable vessel was identified, however the bleeding stopped and so BAE was not required. In our patient's case embolization may have been accompanied by a risk of inadvertent embolization of a spinal artery with possible sequelae of paralysis as it is possible that a spinal artery also originated from the intercostobronchial trunk. 16 In one series 83% of those presenting for the first time with massive haemoptysis were treated with bronchial artery embolization; 46% of those receiving embolization required multiple procedures. 4
Conclusion
For patients with CF, haemoptysis is a frightening event that for many is associated with a period of decline in their lung function and clinical condition. There is also an excess mortality that accompanies such an event. Unfortunately, the evidence base informing clinicians of the optimal strategy to treat this complication of CF is poor and limited to a base of expert opinion that for the most part lacks consensus. Rigorous randomized trials are required to fill this evidence gap.
Footnotes
Acknowledgements
We would like to acknowledge Dr S Whittaker, Consultant Interventional Radiologist, Nottingham University Hospitals NHS Trust for his comments and advice regarding interpretation of the radiological findings.