
Abstract

Introduction
Gastro-oesophageal reflux is common in children and adults with cystic fibrosis (CF).1,2 It has been associated with both decline in lung function and low body mass index.3,4 Traditionally oesophageal pH monitoring has been used to detect acid reflux, but more recently impedence pH studies has allowed more sensitive detection of not only acid, but also non-acid reflux. Fundoplication has been performed in children and adults with variable outcomes, but may reduce decline in forced expiratory volume (FEV1) in those with poor lung function. 5 We describe the multidisciplinary team (MDT) management of a 17-year-old girl with decline in lung function, severe reflux, vomiting and weight loss despite gastrostomy feeding. She underwent successful fundoplication in spite of preoperative respiratory failure.
DECLARATIONS
None declared
None
Written consent to publication has been obtained from the patient
DB
All authors contributed equally
Case report
At transfer at the age of 16 years she weighed 36.4 kg (body mass index [BMI] 14.8) and she was receiving nocturnal gastrostomy feeds. She had a poor appetite and vomited frequently. She had previously received total parenteral nutrition (TPN) to achieve her current weight. The child psychology and psychiatry teams had been actively involved in issues related to her compliance and eating behaviour. Fundoplication had been considered in childhood, but due to lack of objective evidence of reflux and marked psychological distress associated with parental marriage breakdown, this was not pursued. Her lung function was moderately impaired (at best FEV1 1.67 or 55%). She had recently started insulin for CF-related diabetes. She was on maximal medical therapy, including oral Omeprazole 20 mg twice daily (b.d.), Ranitidine 150 mg b.d., Ondansetron 4 mg b.d., Domperidone 15 mg three times daily, and Levomepromazine 6.25 mg b.d. She also inhaled Symbicort 400/12 2 puffs b. d. and nebulized DNase 2.5 mg once daily (o.d.), Colomycin nebulized 1 MU b.d., Gentamycin nebulized 80 mg b.d. She took oral Azithromycin 500 mg o.d., Voriconazole 100 mg b.d., vitamin K 10 mg o.d., vitamin E 400 IU o.d., multivitamins two tablets o.d. and Creon 10000 with meals at variable doses according to oral intake and subcutaneous Glargine and Novorapid variable doses according to oral intake.
We were faced, at transition, with a girl with recurrent admissions, falling weight and effortless vomiting. Her lung function was declining (Figure 1) and she became increasingly despondent and withdrawn. An impedance study showed marked non-acid reflux. We took an MDT approach with psychological support. She agreed to commence TPN alongside prolonged intravenous antibiotics in order to maximize her lung function and her chances with future interventions such as transplant or reflux surgery. She expressed her clear wishes to explore any intervention which would allow her more prolonged wellbeing and improved quality of life and expressed her interest in transplantation if that option were open to her.
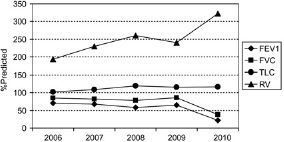
Lung function over 5 years demonstrating decline in FEV1 and FVC and rising RV
A Hickman line was inserted, dedicated to TPN, while her other intravenous medication was given via a peripherally inserted central catheter. She received 1841 kcals via her TPN over a 20-h period and approximately 1300 kcal via her gastrostomy overnight, although her tolerance of this was variable. Her oral intake was very limited. Particular attention was paid to her glycaemic control, with frequent adjustments to her insulin.
Four months into her admission her nutritional state had improved. Her weight increased from 35 kg to 48 kg (Figure 2), making her a better candidate in nutritional terms for surgery of any sort. However, nausea and vomiting persisted despite the acid suppression, anti-emetic and prokinetic medications shown above. Her respiratory function had declined despite prolonged courses of intravenous (IV) antibiotics and good compliance with physiotherapy. Her FEV1 fell to 0.56 (19%) and she was in type-2 respiratory failure (pCO2 8.1 pO2 8.5) requiring 4 L oxygen at rest and nocturnal non-invasive ventilation (NIV) (Figure 3).

Weight since starting TPN showing steady weight gain from 36 kg to 49 kg over 24 weeks followed by stability postoperatively and after cessation of TPN

Preoperative CT demonstrating severe bilateral bronchiectasis with sputum
The option of transplantation was discussed but the transplant team were clear that the evidence of marked reflux with impact on lung function decline would represent a contraindication to transplant and that corrective surgery would be required before listing.
We held an MDT meeting involving a paediatric surgeon experienced in laparoscopic Nissens fundoplication, the adult intensive care unit (ICU), anaesthetics and extra-corporal membrane oxygenation (ECMO) teams as well as our regional transplant team. Discussions covered the anaesthetic challenges of maintaining adequate ventilation despite marked preoperative gas trapping and the likely difficulties associated with insufflation of carbon dioxide into the peritoneum. Alternatives to CO2 including Xenon were explored, but were not thought to be possible. The ECMO team explored the possibility of use of ECMO or Novalung in the event of catastrophic perioperative respiratory failure unresponsive to mechanical ventilation. This involved scanning her femoral and neck blood vessels to assess their suitability for catheters, and sourcing of paediatric-sized instruments. We also agreed guidelines for withdrawal of support in the event of progressive decline. The transplant team outlined that transplant would not occur if she could not be weaned from invasive ventilation.
After open discussion regarding the risks of surgery, she opted to go forward with fundoplication as the only alternative to likely progressive decline with no prospect of transplant. An operation date was set. Her explicit consent was sought for all the different aspects of proposed therapy including potential tracheostomy and ECMO.
She underwent Nissens fundoplication in August 2010. Her perioperative course was stormy but her pCO2 remained less than 11 kPa. Postoperatively she made good respiratory effort and was successfully extubated onto NIV 3 hours postoperatively, when her pCO2 was back to 8.1. She was subsequently weaned to nocturnal use of NIV. She returned to the CF ward after 48 hours. She had some early difficulties with nausea and retching, which improved when Ali-memazine 10 mg at night was commenced. She is now eating without swallowing difficulties, nausea or vomiting, for the first time in years. Her motivation and compliance has greatly improved since her operation.
At review in clinic in October 2010 she had maintained her weight after two weeks at home on enteral feeding alone and, although oxygen-dependent, was enjoying going out with friends and was starting a college course. If her reflux remains controlled, she will be listed for lung transplant shortly.
Discussion
This case raises a number of points for discussion. We will discuss the impact of reflux on CF lung disease, whether reflux is a contraindication to lung transplantation, this patient's nutritional management and how the MDT makes a decision about high-risk surgery.
Impact of reflux on cystic fibrosis lung disease
Gastro-oesophageal reflux is caused by inappropriate relaxation of the lower oesophageal sphincter. 6 It is most common within 3 h of food intake. 6 Traditionally reflux has been investigated with pH monitoring, but more recently impedence studies have allowed detection of non-acid reflux. Here reflux is detected by changes in intraluminal resistance determined by the presence of liquid or gas inside the esophagus. This can be combined with pH monitoring to classify reflux as acid or non-acid (Figure 4). 7
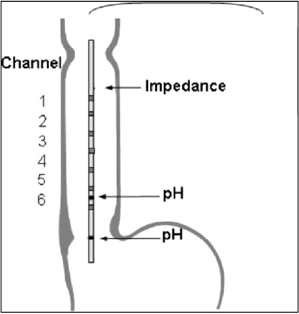
Diagram of probe position for impedence study
Studies have shown prevalence of GOR in children to be 67% with most reflux episodes related to acid rather then weak acid or alkaline reflux. 1 In adults, symptoms suggestive of reflux are common, 63–94% of patients had upper gastrointestinal symptoms and up to 80% had evidence of significant reflux on 24-hour pH monitoring.8,9 Another study of 33 adult CF patients investigated with impedence pH monitoring found 85% had evidence of GOR, most of which were acid, but 21% had weakly acid or alkali reflux.
Less is known about the impact of GOR on lung disease. Epidemiological studies have identified associations between impaired lung function and GOR. 3 In children, GOR has been shown to be associated with significantly reduced FEV1 and FVC, and earlier acquisition of Pseudomonas aerugenosa and Staphylococcus aureus. 10 Inhibition of gastric acid was associated with a smaller yearly decline in MEF 50 and MMEF 25–75 compared with controls. 10 In our case there was no doubt that reflux had significantly impaired enteral feeding efficacy and hence contributed to poor BMI and hence declining lung function. We also believed that the reflux was responsible for recurrent exacerbations of pulmonary disease despite maximal CF therapy.
Nutritional management
Throughout her childhood nutritional status was always a concern, her BMI was well below the 4th centile. She has received supplementary gastrostomy feeds since she was 13 years old and has tried numerous different types of feeds (whole-protein, elemental) at different rates and volumes with variable success. Her oral intake was very limited although she had never been a very good eater. As the symptoms of her GOR got worse her toleration of gastrostomy feeds deteriorated. In order to optimize her nutritional status the decision was made to commence TPN. The decision was made to continue her enteral feeds and promote oral intake in order to limit gastro-intestinal stasis. She received TPN and enteral feeds (Emsogen) providing approximately 3100 kcals per day for 6 months prior to her surgery. Her nutritional status significantly improved with her weight increasing to 48 kgs (BMI 19.3 kg/m2) during this time. Post-surgery once she was established onto full oral intake and an increased volume of gastrostomy feeds (1800 kcals) her TPN was phased out. She is now managing at home on this regimen.
Reflux and lung transplantation
GOR is a relative contraindication to lung trans-plantation. 11 Guidelines recommend the optimisation of GOR prior to consideration of lung transplant. 11 GOR is associated with accelerated decline in lung function following lung transplant. The mechanism for this is thought to be micro-aspiration causing acceleration of progression of bronchiolitis obliterans syndrome. Some transplant centres recommend fundoplication at the time of transplant or shortly post-transplant to try to reduce this progression. 12 Our transplant centre do not perform fundoplication at the time of transplant and recommended preoperative action to allow listing.
Body mass index and lung function
The median BMI in the UK national adult cohort is 21.6. 13 Low BMI is associated with GOR and also with lower FEV1 and faster decline in FEV1. 4 Patients with CF may struggle to meet their increased nutritional requirements and can require oral energy supplements or enteral tube feeding. Adequate nutrition can stabilize or slow the rate of decline in lung function. 14 BMI is an independent predictor of mortality. 15
We hoped our efforts to improve BMI would help maintain lung function but despite good therapy and continuous IV therapy her lung function declined and we suspect this was a direct consequence of reflux. However the achievement of her target weight we believe improved her outcome from surgery and opened the door for transplantation.
MDT decision about high-risk surgery
Others have described their approaches to decision-making in high-risk situations. Important factors identified are identification of team members with appropriate technical skills, identification of potential complications and exploration of potential alternative management routes.16–18
From the patients perspective; estimates of risk of complications and expected benefits of different treatments were particularly important.19,20 Of note, clinicians were often unable to predict the degree of risk patients were prepared to accept, and overestimated the reassuring effect of their counselling about risk. 19 Lower anxiety levels, better quality of life and greater patient satisfaction with care is associated with a better understanding of prognosis and higher level of education. Patients who discuss their care with family members also report better quality of life. 21 Patients with a ‘passive’ approach to decision-making were at greater risk of distress and had poorer quality of life. 22
It was notable that our patient benefited from strong emotional support from her mother once the severity of the situation was clearly explained and the importance of the choices that were being made.
Conclusions
This case highlights the importance of the MDT approach to management of malnutrition, assessment for high-risk surgery and perioperative management. With careful planning, skilled team members and coordinated care, patients with poor lung function and respiratory failure can have a good functional outcome from laparoscopic fundoplication. Such interventions may be necessary to allow patients to be considered for lung transplantation. This case highlights the need to consider gastroesophageal reflux as a cause of nutritional failure despite enteral feeding and laparoscopic fundoplication as a therapy despite poor lung function.
Footnotes
Acknowledgements
The authors wish to thank the multidisciplinary team at the Royal Brompton Hospital