
Abstract

Introduction
Exercise is a complex cardiovascular, respiratory and musculoskeletal interaction which facilitates energy transformation. The UK Cystic Fibrosis (CF) Trust recommends that exercise testing be undertaken at annual review/ although a recent questionnaire survey of centres caring for adults and children with CF suggests that less than 40% patients undergo such tests. 2
DECLARATIONS
None declared
None
Not applicable
DSU
DSU is the sole contributor
None
Adaptation to exercise
A series of adaptations to physiological homeostasis take place on exercise, to enable continued and optimal energy generation when exercising.
Energy generation 3
Energy generation (Figure 1) is governed by the metabolism of carbohydrate and lipid substrates in the presence (aerobic metabolism) or absence (anaerobic metabolism) of oxygen to generate adenosine tri-phosphate (ATP), which functions as a source of energy within muscle cells enabling muscle contraction. Such reactions yield differing amounts of carbon dioxide, a waste gas that requires exhalation.

Energy generation at rest and during exercise
At rest, fatty acid oxidation takes place and for each molecule of fatty acid used, 44 molecules of ATP are generated. This reaction requires oxygen (O2), and results in production of carbon dioxide (CO2) with 16 CO2 molecules produced for every 23 O2 molecules used. As exercise begins, the energy substrate switches to glucose that is mobilised from muscle glycogen stores and, when it undergoes oxidative metabolism glucose too is an efficient method of energy generation with 38 molecules of ATP produced per molecule of glucose used. For every six O2 molecules utilized, six CO2 molecules are produced.
With ongoing high intensity exercise, energy demands cannot be met by oxidative pathways alone, and energy is produced from glucose in the absence of oxygen (anaerobic metabolism). This is a relatively inefficient method of energy generation with only two molecules of ATP produced per molecule of glucose. Furthermore, two lactate molecules are produced which when buffered by bicarbonate lead to production of two molecules of CO2. The point at which non-oxidative glucose metabolism begins to support energy generation on exercise is known as the ‘anaerobic threshold’ or AT.
Thus energy production requires the uptake of oxygen (VO2), as well as yielding carbon dioxide (VCO2). With increasing exercise, the amount of oxygen required (VO2) increases, and the level of carbon dioxide produced (VCO2) increases also. The ratio of oxygen uptake to carbon dioxide production (VO2/VCO2) is known as the respiratory quotient (RQ). This increases from a value of 0.7 when burning fat at rest, to levels approaching 1.0 when utilizing glucose via oxidative (aerobic) pathways. RQ increases to levels >1.0 when ongoing CO2 production ensues from anaerobic metabolism of glucose in the absence of oxygen.
Limitation to exercise
All of us have a limitation to exercise capacity. This may be a limitation in ventilatory capacity to supply O2, a limitation in circulatory ability to deliver O2 to and remove CO2 from exercising muscles, or limitation in muscular utilization of O2 for energy conversion. During exercise, oxygen uptake (VO2) increases linearly with workload until a plateau is reached where further increases in workload do not bring any change in VO2. 4 This point is known as the maximal oxygen uptake point or VO2 max.
Minute ventilation (VE) is a product of respiratory rate (RR) and tidal volume (VT). VE must adapt to meet the energy needs, by meeting demands for oxygen uptake (VO2) and also clearing CO2 that has been produced (VCO2). Increases in RR and breath size (VT) occur, such that VE may increase as much as 25-fold on exercise. In the initial phases of exercise, VT increases to cope with the increased demands of exercise, but when anaerobic metabolism leads to large increases in CO2 production in later exercise a greater increase in RR compared with VT occurs towards maximal exercise VE. At maximal exercise, VE reaches a plateau where further increases in workload do not change the minute ventilation (VEmax).
Cardiac output increases five-fold on exercise and is met by increases in both heart rate and also stroke volume. Peak heart rate is limited by age, although prediction equations vary. 5 Furthermore, re-distribution of blood flow to the pulmonary circulation occurs on exercise, reducing mismatch between ventilation and perfusion; as well as increased blood flow to exercising muscles to meet oxygen demands. There may come a point where cardiac output can no longer increase, and maximal exercise capacity is thus reached. Muscle mass and available energy stores in the form of muscle glycogen may also contribute to exercise limitation. Finally, motivation and volition may limit exercise capacity.
Adaptation to exercise in CF
Exercise ability in CF is determined by both pulmonary function and skeletal muscle mass 6 (which correlates to nutritional status). The principal difference between subjects with CF and healthy individuals on exercise is the presence of an increased dead space within the CF lung 7 which has a deleterious effect on the ability to increase alveolar ventilation.
The dead space refers to areas of lung which have been damaged due to disease, and which no longer allow exchange of oxygen between the airways and the pulmonary capillaries. Dead space is wasted ventilation. The more dead space (i.e. the greater the severity of the disease), the greater the ventilation challenges.
This is illustrated below in Figure 2, where for the same 500 mL tidal breath some 350 mL (70%) contributes to alveolar ventilation (VA) in the healthy individual but only 250 mL (50%) in the individual with CF. Hence in order to meet the ventilatory demands of exercise, respiratory rate and/ or tidal volume must increase to meet these needs. For a given level of oxygen uptake (VO2), a child with increased dead space requires higher minute ventilation (VE) to maintain normal VA.

Illustration of the effect of dead space on proportion of a 500 mL tidal breath available for useful (alveolar - VA) ventilation in a healthy individual and a patient with CF
Reduced lung function in CF may mean that increases in RR play a greater role in meeting ventilatory demand than does increasing VT. Dynamic hyperinflation ensues as shallow breaths and incomplete expiration lead to gas trapping, such that a greater proportion of each breath moves in and out of this dead space rather than participating in gas exchange. Furthermore, airway obstruction may occur in CF as a result of mucus within the airways and/or airways hyper-reactivity. The result of this obstruction is that greater inspiratory airflows must be generated in order for gas exchange to continue optimally. Thus an increase in respiratory muscle effort is required for the same amount of ventilation.
In summary, individuals with CF may have an increased metabolic demand (increased VO2 requirement for same workload) on exercise due to the increased work of breathing that is required to achieve the same level of alveolar ventilation as a healthy subject. Furthermore, those with CF have higher VE for the same level of VO2, due to the presence of an increasing physiological dead space on exercise (which increases with disease severity) that requires increases in VT and/or RR to maintain VA. These factors, when combined together lead to ventilatory limitation on exercise in subjects with CF (Figure 3).
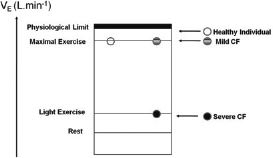
Illustration of relationship between maximal VE and VO2 in healthy subjects and those with differing degrees of CF lung disease
This illustrates that a healthy individual achieves maximal exercise capacity (VO2) at a point before the maximal minute ventilation on exercise (exercise VE) is reached (i.e. a degree of ventilatory reserve exists). In a subject with mild CF, although the same VO2 as a healthy individual is reached, this is achieved with the maximal VE being reached, and published data show that CF subjects will often reach (or even exceed) predicted maximal voluntary ventilation when exercising.7,8 Finally, a subject with severe CF lung disease will also reach the limits of maximal exercise VE, but at a much lower workload and VO2 than those achieved by healthy individuals or those with mild CF.
Why undertake exercise testing in CF
There are several reasons for performing an exercise test in CF subjects.
First, an exercise test is recommended by a number of sources as part of annual assessment.1,9
Second, there is evidence that information from exercise testing gives additional prognostic information to lung function and anthropometric data. Nixon and colleagues 10 studied 109 subjects with CF, and undertook 8-year follow-up to look at factors associated with mortality. Both lung function and also maximal exercise capacity (VO2 max) were correlated with mortality in univariate analyses. Furthermore, when subjects were matched for lung function and other controllable variables, VO2 max remained an independent predictor of subsequent 8-year mortality. Associations of VO2 max with mortality have also been demonstrated in a 7-year follow-up of children with CF 11 and in a 5-year follow-up study of UK adults with CF. 12
Third, the demonstration to CF patients and their families (by way of an exercise test) that an individual with CF can exercise safely can be an empowering and liberating experience. Not only can such a test offer encouragement, but the information gleaned from exercise testing can be used to devise an individualized exercise programme for patients – the notion of ‘exercise prescription’. Exercise is an important therapeutic modality with evidence existing that physical activity correlates with preservation of VO2 max, FEV1, and nutritional status.13,14 Furthermore, exercise training leads to improved exercise capacity and lung function,15,16 and also quality of life 17 in individuals with CF. Finally, exercise testing may prove to be a useful research outcome and shuttle test data are planned secondary outcome measures for the forthcoming UK CF gene therapy trial. 18
How to undertake exercise testing in CF
Exercise testing in CF is recommended by the UK CF trust, to be performed on an annual basis for all CF patients. 1 Which test to perform, and what to do with the information is less clear.
The gold standard exercise test is an incremental cardiopulmonary exercise test (CPET), utilizing a ramp protocol on either treadmill or cycle ergometer. Breath-by-breath ventilatory gas analysis allows the accurate measurement of maximal oxygen uptake (VO2max) – the gold standard measure of exercise capacity. Additionally, assessment of exercise ventilation and circulation characteristics, as well as precise estimation of the time at which energy production switches from an efficient, aerobic method to inefficient, anaerobic energy generation (the anaerobic threshold) can be made. In practice, however, CPET equipment is expensive, requires expert supervision and interpretation, and <10% UK CF centres have access to facilities for CPET. 2
Thus, in the majority of centres a surrogate test for exercise capacity will be performed. Often termed ‘field tests’ for their portable nature, such tests include the six-minute walk test, 19 the three-minute step test, 20 shuttle walk 21 and run22,23 tests, or simply utilizing a treadmill or cycle ergometer in isolation without metabolic measurements. Each of the tests is discussed in turn and the relative merits and drawbacks of CPET and various field tests are summarized in Table 1.
Summary of characteristics of field tests versus CPETs

Field tests
Six-minute walk test (6MWT)
The 6MWT is an established measure of exercise capacity in those with chronic cardiac and/or respiratory disease. The test is performed over a 30–50 m course, walking up and down to complete laps at the best pace possible. Running is not allowed, and vocal encouragement is given throughout. Equipment required is a measuring tape, some cones to mark out walking course, and a pulse oxi-meter to measure heart rate and arterial oxygen saturation (SpO2). A breathlessness score using a Borg scale adapted for exercise can be measured. 24
Reference ranges in children illustrate that a subject's height, as well as age will influence walking distance. 25 Although correlation with peak VO2 was shown in children with severe cardiorespiratory disease, 26 in children with moderate CF lung disease, 19 the correlation between VO2 max and walking distance was lost when VO2 was corrected for body weight. Adults with mild–moderate CF lung disease achieved similar walking distances when compared with healthy controls, 27 however, a greater degree of breathless-ness and lower SpO2 were observed in the CF subjects. This fits with notion discussed above that patients with mild–moderate CF can achieve normal exercise capacity but work harder to achieve this. The 6MWT is submaximal for all but those with severe CF lung disease, and its usefulness is limited accordingly.
Incremental shuttle tests
There are a number of externally-paced, multilevel shuttle tests in use for assessment of exercise capacity, each requiring space but minimal equipment (cones, measuring tape, test CD, recording sheets and pulse oximeter).
The incremental 20 m shuttle run test (or ‘bleep test’) (Figure 4) was developed by Leger and colleagues 22 and is a multistage maximal exercise test that is a commonly used measure of exercise capacity for groups including the police, armed forces, schoolchildren, sports teams, and those signing up to personal trainers. The test begins with a series of shuttle runs at a speed of 8.5 km/h. A ‘bleep’ sounds at the beginning and at regular intervals, such that the shuttle needs to be completed before the next bleep. The test speed increases by 0.5 km/h each minute, resulting in a reduced time between each bleep which continues until a point of voluntary exhaustion is reached. The test has been validated for use in the CF population by Selvadurai and colleagues. 23 The 20 m shuttle test was modified for use in CF, with a starting speed of 4 km/h and subsequent 0.5 km/h increases each minute. 23

CF subject performing the 20 m incremental shuttle test alongside a physiotherapist
A standardized, externally-paced 10 m shuttle walk test was developed by Singh and colleagues 21 along similar lines in order to evaluate exercise capacity in adults with COPD. This incremental walking test has 12 levels varying from approximately 2 km/h on level 1 to 8.5 km/h by level 12. The test was adapted and validated for use in CF by allowing subjects to run, and increasing the number of levels to 15 with a maximum speed of 10.2 km/ h. 28 In spite of these adaptations, this 15-level test remains sub-maximal for some CF patients as well as more than 30% healthy adults who exceed the 15th level, 29 which has resulted in work to extend the test to 25 levels and create a truly maximal test. 29
Three-minute step test
This test is simple to perform, with the only equipment needed being a commercially-available aerobics step, a metronome and a pulse oximeter. Described by Balfour-Lynn and colleagues, 20 the methodology employed is to step at a metronomic rate of 30 steps per min on and off a 15 cm (6 inch) high step. The test is performed over 3 min and subjective patient measures of breathlessness using a Borg scale are made, along with recording of maximal heart rate during exercise and change in SpO2. Exercise-induced hypoxia on the step test has been defined as a fall in SpO2 of >4% on exercise. 30 The test is influenced by patient height and leg length, and is limited by the fact that it is submaximal for many subjects, and is non-progressive. On the positive side, it is easy to set up and perform, and is short in duration.
Incremental step test
Work is in progress to develop an incremental step test that combines the simplicity of the ‘step test’ with the progressive increases in test intensity that allow maximal exercise capacity to be reached. The Nottingham physiotherapy group presented their work at the 2009 Association of Chartered Physiotherapists in CF conference. 31 They have adapted the step test by varying metronome speed every 2 minutes, such that a total of six levels exist with a maximum test time of 12 minutes. The total number of steps can be measured, and used for within subject comparisons on subsequent testing occasions. Prasad and colleagues at Great Ormond Street Hospital have been utilizing a custom-made three-level step with side-rail, and are developing an incremental test based on this equipment (personal communication).
Treadmill tests
Treadmill tests alone can be utilized with a ramp protocol of progressively increasing intensity in order to achieve maximal exercise. This allows assessment of maximum workload achieved, alongside measures of heart rate, SpO2, as well as assessment of breathlessness using a Borg scale.
Cycle ergometry
Similarly, a ramped protocol of increasing workload can be devised using a cycle ergometer, achieving maximal exercise. Maximum workload, heart rate, SpO2, and measures of breathlessness can thus be obtained.
Cardiopulmonary exercise testing
Cardiopulmonary exercise testing (CPET) is a comprehensive assessment of cardiorespiratory and metabolic changes on exercise. Progressive exercise is performed at increasing levels of intensity either on a treadmill or cycle ergometer, while simultaneous breath by breath measures of airflow and inhaled and exhaled mouth pressures of O2 (pO2) and CO2 (pCO2) are made, along with heart rate, SpO2 and breathlessness scores. The set-up costs for CPET are high with the required metabolic cart equipment costing around £15,000. Furthermore, because of the infection control risks associated with CF, there is a per test cost with regard to disposing of the pneumotachographs used to measure air flow, as well as cleaning of sampling lines used for ventilatory gas analyses. Data collected throughout the exercise include direct measures of VO2, VCO2, heart rate, RR, VT, and end-tidal measures of O2 and CO2.These data in turn allow calculation of respiratory quotient (RQ), minute ventilation (VE) and ventilatory equivalents for O2 and CO2 (VE/VO2 and VE/VCO2) throughout exercise. Furthermore, the point at which energy production switches to non-oxidative pathways – the anaerobic threshold can be estimated with reasonable precision. Data from CPET can be analysed at each time-point, and is also graphed as a nine-panel plot with the following series of graphs:
VE and RR (y axis) and time (x axis);
Heart rate (HR) and VO2/HR (the oxygen pulse) (y axis) and time (x axis);
VO2, VCO2 and workload (y axis) and time (x axis);
VE (y axis) and VCO2 (x axis);
HR and VCO2 (y axis) and VO2 (x axis);
VE/VO2 and VE/VCO2 (y axis) and time (x axis);
VT(y axis) and VE (y axis);
RQ (y axis) and time (x axis);
End-tidal O2 and CO2 [etO2 and etCO2], and SpO2 (y axis) and time (x axis).
CPET gives rise to precise measures of exercise capacity, and allows the assessment of whether a truly maximal test was undertaken. Assessment of the degree of ventilatory and/or cardiovascular limitations to exercise can be made. Exercise testing using CPET has been vital to increasing our understanding of cardiorespiratory adaptation to exercise in CF.32,33
Figure 5 shows exercise tests undertaken on two teenage boys with CF. Boy A has normal exercise tolerance and FEV1 of 95% predicted, while Boy B has nocturnal hypoxaemia and an FEV1 of 34% predicted. Boy A has a high normal VO2 max at 55 mL/kg/min, whereas Boy B has a VO2 max of only 29 mL/kg/min which is well below that predicted for age.

Oxygen uptake on exercise testing for two boys with CF
Predicted peak heart rate for each boy using the formula 220-age was 206/minute. Boy A reached a peak heart rate of 205/minute, while boy B had a heart rate of 170 at peak exercise. Boy B thus has a degree of cardiac reserve at the end of maximal exercise suggesting that he may have been ventilatory-limited. Boy A increased his tidal volumes from 400 mL at rest to 1.8 L at peak exercise, while boy B had a resting VT of 300 mL and could only increase to 600 mL during exercise. Furthermore, boy A had a resting RR of 15/ minute which increased to 45 on exercise, whereas boy B had a resting RR of 40 and a rate of 80 at peak exercise. Although able to exercise to some degree, boy B is exercise-limited by an inability to increase his ventilation to meet the demands of ongoing exercise (Figure 6).

Plot of VE and RR against time showing normal exercise ventilation (Boy A) and ventilatory limitation on exercise (Boy B) in CF
Summary
Exercise in CF is associated with improvements in physical and psychological wellbeing. Exercise testing may have an important role in assessing exercise ability and tailoring patient-specific exercise programmes, and exercise-related outcome measures may prove very useful for research intervention studies. Exercise capacity is of known prognostic importance in both adults and children with CF, and the degree of mutual exclusivity that separates fitness from lung function suggests that exercise testing is a vital diagnostic tool for identifying patients at risk of decline.
The question of why exercise test in CF seems self-evident, but how to test is less clear-cut. A variety of field tests exist that are low-cost tests requiring minimal equipment. These act as surrogate tests of exercise capacity and can be submaximal in some cases. The gold standard test is CPET, a maximal test that provides precise exercise data. CPET is, however costly, needs highly specialized equipment and also requires technical expertise to supervise and interpret the test.
The choice of test depends upon the question one is trying to answer. The chosen exercise test should be one that allows maximal exercise to be achieved, and may also be influenced by equipment and expertise that is held locally. Research outcomes may need the precision of CPET, whereas if one is looking for year on year within patient comparison, selection of a field test or incremental treadmill or ergometer test without metabolic measures may be appropriate. A desire for precise and reproducible data on exercise capacity in CF, however, may demand CPET as the test of choice of the future.